Transcription
Public Behavioral HealthWorkforce WorkgroupStrategies for Meeting the Need in our CommunitiesDecember 2021
Table of ContentsExecutive Summary . 3Introduction . 5What is the Public Behavioral Health System? . 6What Types of Professionals Work in the Public Behavioral Health System? . 7Increasing Need for Behavioral Health Services . 7Increasing Pressure on the Behavioral Health Workforce . 9Strategies . 13Conclusion and Next Steps . 19Participating Organizations . 19Page 2
Executive SummaryOver the last several years, Tennessee State Government and the Tennessee General Assemblyhave made significant investments in both expanding and enhancing the state’s publicbehavioral health system. With primary funding coming from TennCare (the state’s Medicaidagency) and the Tennessee Department of Mental Health and Substance Abuse Services (thestate’s behavioral health authority), Tennessee’spublic behavioral health system exists to servePressures on the workforceMedicaid covered or uninsured Tennesseans livingcoexist with an increasingwith serious mental illnesses, serious emotionalneed for behavioral healthdisturbances, substance use disorders, and cooccurring disorders. This system is supported withservices. With challengesstate appropriations and federal funds and providesexacerbated by the COVID-19for a continuum of care that encompassespandemic, it is imperativeprevention, early intervention, treatment, andthat all partners in the publicrecovery support services. Through a large networkof community mental health centers, substance usetreatment centers, non-profit agencies, faith-basedbehavioral health systemassess for opportunities tocommunities, managed care organizations, andgrow and strengthen theother direct service providers, both TennCare andcommunity of professionalsthe Tennessee Department of Mental Health andSubstance Abuse Services (TDMHSAS) supportevidence-based services and supports that createpathways to recovery and independence for thosewho provide mental healthand substance use treatmentand supports.impacted by behavioral health disorders who areeither covered by Medicaid or uninsured.Despite the significant progress made in strengthening Tennessee’s public behavioral healthsystem, challenges persist. Like many other sectors and industries across the United States, thestate’s public behavioral health system has significant challenges in recruiting and retaining anappropriate workforce. These pressures on the workforce coexist with an increasing need forbehavioral health services. With challenges exacerbated by the COVID-19 pandemic, it isimperative that all partners in the public behavioral health system assess for opportunities togrow and strengthen the community of professionals who provide mental health andsubstance use treatment and supports.Page 3
Recognizing the impact of this ongoing challenge, TDMHSAS and TennCare convened theTennessee Public Behavioral Health Workforce Workgroup in June 2021. Serving as convenorsand facilitators of this workgroup, the agencies gathered a diverse group of stakeholders andprofessionals, each of whom was uniquely positioned to provide insight to this critical issue.This report represents the work of the Public Behavioral Health Workforce Workgroup andproposes short-term and long-term strategies that directly address recruitment and retentionopportunities that can be implemented by local behavioral health providers, colleges anduniversities, and various Tennessee State Government Departments.Recognizing that behavioral health needs of Tennesseans continue to grow, maintaining asteady and resilient workforce is more critical than ever. It is our hope that this report providesactionable steps that will strengthen the career pipeline into the public behavioral healthworkforce and assist in maintaining a labor force of qualified, competent, and dedicatedprofessionals who serve Tennesseans living with behavioral health challenges.Page 4
IntroductionThe State of Tennessee has consistently been lauded as a national leader in behavioral healthboth for its services at the community level and its cooperation, communication, andcollaboration at the state level. Efforts and initiatives ranging from integrated care (e.g.,Tennessee Health Link) and a statewide crisis system to supportive housing and substance usedisorder treatment are just a few examples of how Tennessee has worked to create anaccessible and effective system of care for individuals living with the most serious behavioralhealth issues. Notably, in the 2021 Mental Health America State of Mental Health in Americareport, Tennessee improved to 28th in the United States, up from 39th in the previous year.Beyond its innovative and cross-cutting programs, Tennessee is also unique for its very strongworking relationship between the state’s behavioral health authority, the TennesseeDepartment of Mental Health and SubstanceAbuse Services (TDMHSAS) and the state’sMedicaid agency, TennCare. It is through this“Future supply and demandlong-standing partnership that TDMHSAS andfor behavioral healthTennCare set out to address an issue troublingpractitioners will be affectedstates across the country, a public behavioralhealth workforce that is challenged by increasedby a host of factors related todemand and need.population growth, aging ofTo generate both short-term and long-termoverall economic conditions,strategies to address recruitment and retentionissues, TDMHSAS and TennCare launched thePublic Behavioral Health Workforce Workgroupthe nation’s population,expansion of insurancecoverage, changes in healthin June 2021. This workgroup consisted ofcare reimbursement,professionals representing the providerretirement, attrition,community, public and private institutions ofavailability of training, andhigher education, and other relevant statedepartments and professional associations.Meeting over the course of three months, thegeographic location of thehealth workforce.” Healthworkgroup operated under three overarchingResources and Servicesgoals:Administration (HRSA)Page 5
It is the hope of the Tennessee Public Behavioral Health Workforce Workgroup, TDMHSAS, andTennCare that this report is useful for key leaders and decisionmakers in Tennessee. Thisdocument will clearly frame the needs and gaps related to the public behavioral healthworkforce in Tennessee and, most notably, will provide strategies for consideration.While the organizers and participants in this workgroup recognize workforce issues impact allareas of behavioral health care, our focus for this report is on the public sector of services andsupports.What is the Public Behavioral Health System?The public behavioral health system generally refers to the network of organizations andprofessionals who care for people served by state Medicaid programs or people who areuninsured and indigent, including those who may be involved with the civil and justice legalsystems. These individuals traditionally have more intensive needs and require a wide range oftreatment and recovery services and supports. Examples of services provided in the publicbehavioral health system include crisis stabilization and inpatient psychiatric services,supportive housing and employment, peer support, intensive care coordination and casePage 6
management, partial hospitalization and substance use residential treatment, and otherrehabilitative and vocational programs.In addition to treatment and recovery supportservices offered in the public system, the publicsystem also includes prevention and early“The Mental Health DeliverySystem can only be as good asintervention services. In the State of Tennessee,the practitioners who staff it.”programs such as Substance Abuse PreventionFederal Action Agenda forCoalitions, suicide prevention initiatives includingthe Tennessee Suicide Prevention Network,the President’s New FreedomCommission on Mental Health (2002)school-based mental health programming, as well as the Regional Intervention Program(focusing on children ages 2-6) are just a few examples of prevention and early interventionefforts supported by the public system.What Types of Professionals Work in the PublicBehavioral Health System?The public behavioral health workforce includes a wide range of professionals with varyingdegrees of educational and work experience. These include clinical professionals such aspsychiatrists, psychologists, psychiatric nurses, social workers, professional counselors,addiction counselors, and non-clinical professionals such as case managers, peer supportspecialists, and recovery coaches. The public behavioral health workforce also includesindividuals trained in prevention, early intervention, and professionals who work with specialpopulations such as people experiencing homelessness or individuals who interface with thejustice system.Increasing Need for Behavioral Health ServicesPrior to the COVID-19 pandemic, Tennessee, like many other states, had observed notableincreases in drug overdoses and suicides among its population. Unfortunately, the COVID-19pandemic exacerbated both mental health and substance use issues, including those amongindividuals served by the public system. According to the Kaiser Family Foundation, as reportedin February 2021, “During the pandemic, about 4 in 10 adults in the U.S. have reportedsymptoms of anxiety or depressive disorder, a share that has been largely consistent, up fromone in ten adults who reported these symptoms from January to June 2019.” A KFF HealthTracking Poll from July 2020 also found that many adults reported specific negative impacts onPage 7
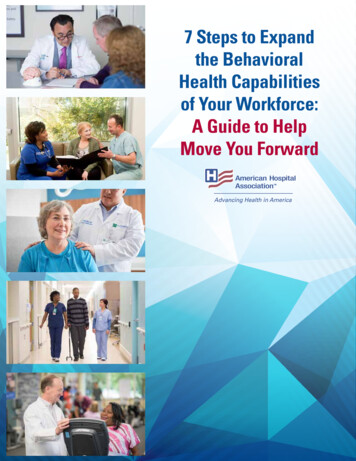
their mental health and well-being, such as difficulty sleeping (36%) or eating (32%), increases inalcohol consumption or substance use (12%), and worsening chronic conditions (12%), due toworry and stress over the coronavirus. As the pandemic wears on, ongoing and necessarypublic health measures expose many people to experiencing situations linked to poor mentalhealth outcomes, such as isolation and job loss.Indicators of Anxiety Disorder or Depressive DisorderBased on Reported Freqency of Symptoms in the Last 7 DaysJun 23 - Jul 5Jun 9 - Jun 21May 26 - Jun 7Apr 28 - May 10May 12 - May 24Apr 14 - Apr 26Mar 17 - Mar 29Feb 17 - Mar 1Mar 3 - Mar 15Feb 3 - Feb 15Jan 6 - Jan 18Jan 20 - Feb 1Dec 9 - Dec 21Nov 25 - Dec 7Oct 28 - Nov 9Nov 11 - Nov 23TennesseeOct 14 - Oct 26Sep 30 - Oct 12Sep 2 - Sep 14Sep 16 - Sep 28Aug 19 - Aug 31July 16 - July 21July 2 - July 7July 9 - July 14June 25 - June 30June 18 - June 23June 4 - June 9June 11 - June 16May 28 - June 2May 21 - May 26May 7 - May 12May 14 - May 19United StatesApr 23 - May 550454035302520151050Source: U.S. Census Bureau, Household Pulse Survey, 2020-2021In a 2020 study conducted by East Tennessee State University Applied Social Research Lab,slightly more than half (50.4%) of Tennessee respondents reported they had trouble sleeping inthe week prior to the poll – 19.4% had trouble sleeping most or all the time, 17.7% had troublesleeping occasionally or a moderate amount of time, and 13.3% had trouble sleeping some or alittle of the time. Similarly, a majority (53.5%) reported that they had felt nervous, anxious, or onedge at some point in the previous week. Many also reported feeling depressed (43.4%) andlonely (42.8%).As Tennessee progresses farther from the start of the pandemic, a fuller picture of the lastingeffects is becoming clear. According to a July 2021 report from the Centers for Disease Controland Prevention (CDC), preliminary numbers show that Tennessee saw more than 3,000 fataldrug overdoses in 2020, an increase of 44% from the prior year.Page 8
Increasing Pressure on the Behavioral HealthWorkforceWhile there is clear evidence that mental health and substance use issues are increasing acrossthe country and in Tennessee, there is also evidence that the workforce which serves peopleaffected by behavioral health issues is struggling. While the nation as a whole experiencesworkforce issues in the post-pandemic world, staffing and retention challenges related tobehavioral health are longstanding and have been exacerbated by pandemic concerns.The Public Behavioral Health Workforce Workgroup was tasked with clearly identifying gaps andneeds related to the public behavioral health workforce using relevant Tennessee specific dataand national data. The following data points illustrate those gaps and needs and howinvestment in the public behavioral health system yields returns that positively impact othersectors of society, including the economy and employment, healthcare as a whole, and thecriminal justice system.According to the Kaiser Family Foundation, as of September 30, 2020, only 13.2% of the needfor psychiatrists in Tennessee is being met. In other words, Tennessee is falling short ofmeeting the need for psychiatrists by more than 85%. This metric is computed by dividing thenumber of psychiatrists available to serve the population of the area, group, or facility by thenumber of psychiatrists that would be necessary to eliminate the Health Care ProfessionalShortage Area in mental health (based on a ratio of 30,000 to 1 (20,000 to 1 where high needsare indicated). iPage 9
The map on the preceding page uses Health Resources and Services Administration (HRSA) datato illustrate Health Professional Shortage Areas (HPSA). Scores range from 1 to 25 with higherscores and darker shades of blue reflecting the greater priority.According to HRSA, by 2030 Tennessee will experience troubling staffing shortages for severaldifferent behavioral health professions ii: Estimated shortage in 2030 for mental health counselors: 1,270 Estimated shortage in 2030 for psychologists: 890 Estimated shortage in 2030 for substance abuse counselors: 830 Estimated shortage in 2030 for psychiatrists: 780 (the bulk of these, 760, are estimatedto be adult psychiatrists) Estimated shortage in 2030 for marriage and family therapists: 140In addition, an analysis prepared by National Association of Social Workers Tennessee Chapter,using May 2020 information from the Tennessee Department of Health, highlights the currentchallenging shortage of social work professionals in many counties outside our major urbanareas.During a point in time search ofPay Rates Compared (Annual Mean Wages)Indeed.com conducted in mid-JuneJob TitleUSTNof 2021, there were 559 TennesseeOverall 56,310 47,530job openings for mental healthGeneral Social Workers 64,940 55,210counselors, 101 Tennessee jobMH/SA Social Workers 54,540 43,070openings for psychiatric nursePsychiatrist 217,100 210,770Nurse Practitioner 110,030 101,639Marriage and FamilyTherapist 56,890 41,440Registered Nurses 80,010 64,120practitioners, and 73 Tennessee jobopenings for psychiatrists.On average, pay rates for behavioralhealth workforce positions inSource: May 2020 State Occupational Employment and Wage EstimatesTennessee (psychiatrists, general social workers, mental health and substance abuse socialworkers, psychiatrists, nurse practitioners, marriage and family therapists) are lower than theUS average pay rates for these same positions. iii Specific to Tennessee, salaries for Departmentof Children Services (DCS) case manager far outpace those who work in community behavioralhealth. For example, the average salary for a DCS Case Manager 4 (master’s degree required/3Page 10
years’ experience) is 56,061 and for a DCS Case Manager 3 (bachelor’s degree/2 years’experience) is 49,179.Median wages across mental healthTennessee Social Worker Pay Rates ComparedNumberEmployedAnnual MeanWageMental Health andSubstance Abuse1,220 43,070an example, 72% hold a graduateChild, Family, andSchool6,000 44,090degree but get paid less than theHealthcare6,160 49,990median wages for all occupations inAll Others1,560 55,210occupations in Tennessee areJob Titlesignificantly lower than at thenational level. Furthermore, usingTennessee clinical social workers asTennessee combined.ivSource: May 2020 State Occupational Employment and Wage EstimatesThe Association of American MedicalAverage Debt of Behavioral Health ProfessionalsColleges notes that sub-parJob Titlereimbursement for mental healthproviders is common, compared toAverage DebtPsychiatrist 200,000Master of Science in Nursing 47,321Master Level Social Worker 46,592Bachelor Level SocialWorker 29,323Tennessee ranks 46th among the 50Bachelor Level Nurse 23,711states and the District of ColumbiaAssociate Level Nurse 19,928physical health providers, leavingmany mental health organizationschallenged to cover salaries. vwhen it comes to mental health workforce availability.viOn top of low pay rates, many professionals begin their behavioral health careers saddled withsignificant student debt. While this concern is certainly not unique to behavioral health, thesignificant debt combined with the sub-standard pay entices or forces many caringprofessionals to choose family financial needs over a job they love. Additional data on socialwork graduates provided by one public university in Tennessee paints a specific picture of theburden of student loanAverage Debt of Recent Social Work Graduatesdebt for recent socialwork graduates.19-20GraduatesPercent of Graduateswith DebtAverage DebtBA4480% 34,692MSW5578% 49,201DegreePage 11
Recently, the National Council for Mental Wellbeing released a report documenting nationwidetrends among community behavioral health providers, which mimic Tennessee on the demandfor behavioral health services and workforce shortages in meeting this demand. According tothe report, nearly all National Council members are experiencing increased demand; however,don’t have the staff to meet the growing need:97% say it has been difficult to recruit employees.82% say it has been difficult to retain employees.62% say their patient waitlist has grown over the past three months.As it relates to reimbursement rates, TDMHSAS recognizes that its provider rates need to beincreased as there has not been a significant increase in numerous years. TennCare rates aresubject to renegotiation but both TennCare providers and managed care organizations (MCOs)must renegotiate contracts to address rates. According to workgroup members, provider ratespreviously negotiated have not been adjusted for inflation or the current cost of doingbusiness. TDMHSAS has not moved forward with a cost-of-living increases but looks to speakto this in future state budget requests.Researchers agree on the high return oninvestment that comes with funding behavioralhealth care. For every 1 spent to expandResearchers agree on the highreturn on investment thattreatment for depression, the leading cause ofcomes with funding behavioraldisability worldwide, 7 in cost savings can behealth care. For every 1 spentexpected.viiInvestment in treatment for anxiety disorders,to expand treatment fordepression, the leading causethe most common category of mental illness inof disability worldwide, 7 inthe U.S., carries an expected 4 in cost savingscost savings can be expected.per dollar spent. For substance use disordertreatment, every 1 invested saves 4 in health care costs plus 7 in criminal justice costs. TheNational Institute on Drug Abuse reports that total savings can exceed addiction treatmentcosts by a 12 to 1 ratio. viii Investing in the provider community is vital to meeting the expectedgrowth in the need for services for Tennesseans and to meet any anticipated return oninvestment.Page 12
StrategiesThe Public Behavioral Health Workforce Workgroup has identified several recommendedstrategies that could be pursued by local, state, and institutional entities to address the publicbehavioral health workforce issue. These strategies fall into two categories: short-termstrategies focusing on retention and re-energizing of the current public behavioral healthworkforce and long-term strategies focusing on recruiting the next generation of publicbehavioral health workers and equipping the future workforce with the training and passion toserve an ever evolving and unique clientele from varying diverse backgrounds and all regions ofTennessee.While TDMHSAS and TennCare convened and facilitated the workgroup, the strategiesidentified in this report have been discussed and developed by the workgroup members. Assuch, TDMHSAS and TennCare cannot commit to implementing each strategy but arecommitted to working collaboratively to examine and explore each strategy. Both agencies willhave to work with the administration and legislative branch on items which the departmentsbelieve are in the best interest of Tennesseans living with behavioral health disorders.Strategy: Employee-Focused Incentives ShortTermActivities: Identify the means to fund and implement a PublicBehavioral Health sign-on bonus initiative to recruit and retainvital positions. Expanded bonus opportunities for ruralpositions and other underserved populations should beprioritized.Create a Public Behavioral Health Scholarship Programo Annual stipends or allowances to TDMHSAS/TennCareagencies to support professional development, specializedcertification, and clinical licensure hours.o Partnership with colleges/schools to provide tuitionstipends for behavioral health-related fields with thecommitment of post-graduation service at a public behavioralhealth provider.o Paid clinical supervision hours. rs,Colleges andUniversitiesBackground: TDMHSAS has submitted a proposal to offer funding to local providers to findopportunities to retain current staff and offer reimbursement for tuition costs. If funding isnot secured, TDMHSAS will work with local providers on seeking other funding opportunities.Page 13
Strategy: Employee-Focused Benefits ShortTermActivities: Continue to cross train staff inside organizations wherefeasible and develop relationships with partner organizationsto allow for similar cross training to better understand rolesand how the system functions and why their work matters. Regular trainings on Vicarious Trauma and ers Provide opportunities for flexible schedules, which couldinclude working from home. LongTermActivities: Identify the means and internal agency support needed toallow providers to offer more sabbatical opportunities. Create cross-provider collaborative learning opportunitieslike LEAD TN where networking and collaboration unityProvidersBackground: Retaining employees in the public-sector workforce is vitally important. Thiscould potentially be achieved through additional training and flexible schedules.Strategy: Research and Explore Costs of ServicesActivities: ShortTerm Create an inventory of all reimbursable services byTDMHSAS and TennCare indicating where both fund the samelevels of careo Workgroup members recommended that TDMHSAS andTennCare hire an external group to analyze service costs andreimbursement rates Produce a report that shows the costs andreimbursement rates to provide services and includespotential recommendations.o Analyze cost differences across rural and urban areas ofthe roviders Utilize new Federal funds to supplement the rates forcommunity services.Page 14
LongTerm Use the report showing the cost of providing services andsubsequent updates to develop a plan to address continuedfunding for provider rates and to address a means to provideregular rate review and unityProvidersBackground: To better understand the financial needs of the community providers,TDMHSAS and TennCare need to know the costs of providing the services and treatments.Strategy: Diversity and Inclusion in Public Behavioral Health ShortTermActivities: Create a comprehensive plan for diversity and inclusionthat includes all facets of service delivery (including outreach,education, marketing, training, etc.) and incorporatesviewpoints from everyone involved, not just human resourcesstaff. Invest in talent management for individuals alreadyemployed in the organization. Ensure organizational missions and vision statementsinclude diversity and inclusion as well as a focus on recoveryoriented values that promote hiring and retaining people inrecovery. LongTerm Recruit a workforce that closely resembles thepopulations served to foster mentoring relationships and thesupport of the community served. This kind of recruitmentcan result in increased community engagement and supportfor these Universitiesand Providers,TDMHSAS,TennCareBackground: Having a diverse and inclusive workplace and workforce increases the ability tobring varied viewpoints and thought processes to problem solving which leads to growth.There are also benefits in better connecting with individuals needing services who interfacewith the behavioral health workforce.Page 15
Strategy: Expand Internship OpportunitiesActivities:Expand Internship Opportunities with focus on:ο Increase number of paid internships, increase number ofinternships in rural areas.ο Increase opportunities for internships/trainings toeducate students on use of telehealth.ο Increase internship opportunities in Rural Tennessee. ShortTerm Create Public Behavioral Health Internship Portal for TNschools to connect students with opportunities at publicbehavioral health providers. We recommend that TDMHSAS and TennCare explorewhether services delivered by interns in various disciplinescan be reimbursed and under what lleges andUniversities,CommunityProviders Hold annual consortiums to gather providers andeducational institutions for discussion, collaboration, andeducation for supervision of interns or clinical hours. Consider reimbursement for LADAC I’s and supervisedLADACs in training.Activities: LongTerm Review scope of practice of internship levels (Bachelors,Masters, etc.) to identify ways to expand behavioral health.Often there are limits to what an intern can do within theinternship based on education level. There are alsolimitations on what services can be billed under an intern. Pursue the opportunity to have internship hours countedtoward the number of hours needed for licensure. Pursue a long-term goal of increasing opportunities forBH providers to employ interns as they graduate inprofessional ‘bridge’ programs in provider shortage areas.RelevantAgencies:Colleges S,TDHBackground: Colleges and universities have expressed barriers to finding providers forinternship opportunities, especially for baccalaureate level education. Local providers haveexpressed concerns with having adequate supervision and staff to take on interns and beingable to use them as staff, especially if their time cannot be billed. This provides anopportunity for more conversations between colleges and universities and providers.Page 16
ShortTermStrategy: Loan ForgivenessActivities: Increased marketing on existing behavioral health loanforgiveness opportunitiesWho’sResponsible:Colleges andUniversities,TDHActivities: Long Term Employer-based loan forgiveness programs available afteran employee reaches a specified tenure level Expansion of loan forgiveness programs specific tobehavioral health Expansion of loan forgiveness programs with special focuson underserved areas/populationsWho’sResponsible:Colleges andUniversities,TDH,CommunityProvidersBackground: Loan forgiveness options are often not known about or there is difficulty innavigating the application process. Making improvements could entice more students toenter the field.Strategy: Behavioral Health LicensureActivities: ShortTerm Paid supervision opportunities for clinical license hours Supervisory training for newly licensed staff to build poolof eligible supervisors Promote paraprofessional opportunities that can be usedas internship hours, LADAC hours for clinical supervision andCertified Peer Recovery Specialist (CPRS) hours.RelevantAgencies:TDH,Colleges es: Align required hours for supervision with othercontiguous states. LongTerm State to State License Transfer, make more accessible. More options for Continuing Education that are free oraffordable. Statewide training/credentialing opportunities that focuson networking and collaborative networks. Explore opportunity for a supervisory level of CPRSCertification. Explore the opportunities for a supervisory level CPRS tohave the ability to bill and supervise for services throughMedicaid and other behavioral health services.RelevantAgencies:Colleges andUniversities,TDH, NASWTN, otherprofessionalassociations,TDMHSAS,TennCarePage 17
Replicate and utilize the current Rural Health Associationof Tennessee (RHAT) program for apprenticeships for publicbehavioral health careers.Background: Graduating with a degree is an achievement, but often in the behavioral hea
behavioral health system. With primary funding coming from TennCare (the state's Medicaid agency) and the Tennessee Department of Mental Health and Substance Abuse Services (the state's behavioral health authority), Tennessee's public behavioral health system exists to serve Medicaid covered or uninsured Tennesseans living