Transcription
Drug Testing in the PainManagement SettingSeptember 27, 2011Gwen McMillin, PhD, DABCCUniversity of Utah, ARUP Laboratories
DisclosureLaboratory director consultant forClinical Lab Consulting, LLC
Application of drug testingFORENSIC:Death investigationsCrime/accidentsEmploymentPain Competitive sportsManagementMilitary, DOTMEDICAL:Intoxications/EDTDMSurgery qualificationDrug abuse monitoringSOCIAL:Child custodySobriety testingLicensures
Objectiveso Compare strengths and limitations ofscreening and confirmation testing for drugsused in the pain management settingo List scenarios that could explain bothpositive and negative drug testing resultso Understand the limitations of urine drugtesting for evaluating dose adherence
Pain is a major health and social issuePain is the #1 reason people seek medical carePrevalence of chronic non-cancer pain ( 3 months)in the US is estimated at 20-60%, over a lifetimeChronic non-cancer pain is expensive– Leading cause of health-related absenteeism– Increased risk of depressive and anxiety disorders– Estimated medical costs in the US up to 635 billion/yr(Reuters US Online Report Health News June, 2011)
Pain management in medicinePain management is a medical specialty (AmericanBoard of Pain Medicine, 2200 diplomates, 2011)Treatment approach is multi-disciplinary; primarygoals to diagnose and treat the underlying causeof pain, restore/maintain function and well-beingCommonly used medications include opioids,benzodiazepines, antidepressants,anticonvulsants, THC, and muscle relaxants
Drugs in “Top 200” US scripts (2010) Opioid analgesics–––––– Benzodiazepine-likeHydrocodone (#1, 3, 34, 147)Oxycodone (#39, 54, 128, 141)Tramadol (#33, 122)Codeine (#66)Propoxyphene (#98, 169)Buprenorphine (#163)–––––Alprazolam (#46, 57, 88, 119)Clonazepam (#47, 116)Lorazepam (#78, 200)Diazepam (#106)Zolpidem (#24, 134, 186) Other medications Non-opioid analgesics– Ibuprofen (#21, 113)– Naproxen (#132, 187)– APAP (#1, 3, 34, 39, 54, 66, 98, 147, 169)––––Gabapentin (#87, 112, 140)Pregabalin (#74)Carisoprodol (#100)Antidepressants (#13, 20, 29, 35, 56,77, 83, 89, 103, 120, 138, 161, 184, 198)Rank #s e/2011/May2011/Top-200-Drugs-of-2010
Pain relievers are misused Pain relievers are the #1 new illicit drug in the U.S.National Survey on Drug Use in Health (NSDUH), 2009 It is estimated that 20% of Americans have usedprescription drugs for nonmedical reasons;including 15% of 12th graders www.drugabuse.gov 60% of people who use pain relievers fornonmedical reasons obtain the drug from a friendor relative SAMHSA, 2006
Estimates of profitabilityDrug“Street” Price(per pill)Retail PriceEstimate(per pill)Potential“Profit”(per pill)Oxycodone 12 - 40 6 34Oxycontin 50 - 80 74Percocet 10 - 15 9Hydrocodone 5 - 20Vicodin 5 -25 1.50 18.50 23.50CNN Money; June 1, 2011
Efforts to minimize drug trafficking US Department of Justice, Drug EnforcementAdministration, Office of Diversion Control:www.deadiversion.usdoj.gov Hotline for illicit pharmaceutical activity:877-RX-ABUSE (792-2873) Focus Topics––––Diversion awarenessDrug disposal (Secure and Responsible Drug Disposal Act of 2010)Internet pharmacy controlCurrent cases, and rulings, against doctors
Unintentional US deaths, Poisoning/brief.htm
“REMS” requirements by the FDAREMS Risk Evaluation and MitigationStrategies intended to“protect patients from serious harm”“ensure that the benefits of the drug continueto outweigh the risks of adverse outcomes”Sponsors/manufacturers of select long-acting or extendedrelease opioid formulations will be required to providetraining to prescribers for safe use, storage, and disposal rmationbyDrugClass/ucm163647.htm
Monitoring patients for misuse and abusePost-Approval REMS Notification, Appendix A, accessed n monitoring programsUrine drug testingScreening and referrals for substance abusetreatment
Clinical Practice Guidelines for Opioid Prescriberso VA/DoD Clinical Practice Guideline for the Management of OpioidTherapy for Chronic Pain, 2010o Canadian Guideline for Safe and Effective Use of Opioids forChronic Non-Cancer Pain Parts A and B, 2010o [Washington State] Interagency Guideline on Opioid Dosing forChronic Non-cancer Pain: An Educational Aid to Improve Care andSafety With Opioid Treatment, Updated 2010o Utah Clinical Guidelines on Prescribing Opioids for Treatment ofPain, 2009o APS-AAPM Clinical Guidelines For the Use of Chronic OpioidTherapy in Chronic Noncancer Pain, 2009o ASIPP Guideline: Opioids in the Management of Chronic NonCancer Pain — an Update of American Society of the InterventionalPain Physicians’ Guidelines, 2008
Objectives of drug testing1. Detect drug use Verify adherence to prescribedmedications Identify use of undisclosed drugs2. Discourage drug misuse Reduce likelihood of diversion Reduce likelihood of abuse
The “10 P’sProtect the patientProtect the practitionerProtect the pain therapy planProtect the communityProtect societyPromote cost-effectivenessProtect resourcesPractice safe and effective medicinePractice and fulfill ethics in medicinePreserve access to therapyChristo, Pain Physician 14:123-43, 2011
How do patients perform?
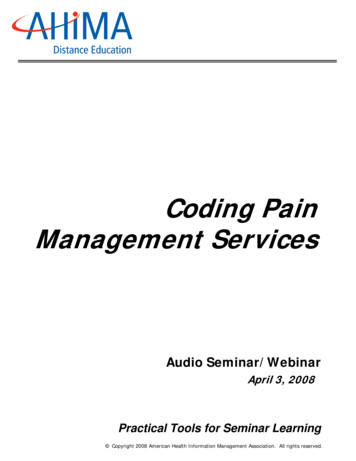
Urine drug testing (UDT) resultsReference lab study, representing 938,586 resultsExpected drug: 26%Illicits: 11%Unexpected prescription drug: 29%Missing drug: 38%0510152025303540Couto et al, Population Health Management 12(4), 185-90, 2009
Another example of UDT results Clinic-based study, retrospective, 470 patients Urine drug testing results confirmed by GC-MS All results reviewed/verified vs. patient charts forappropriateness of test results––––Expected opioidIllicitsUnexpected opioidMissing opioid55% (vs. 26%)20% (vs. 11%)15% (vs. 29%)10% (vs. 38%)Michna et al, Clin J Pain 23:173-9, 2007
Sources of variation in UDT Pharmacokinetic variability of drugs, drugformulations, and patients Limitations of urine Testing methods involved Drug Patient Sample Test Inappropriate interpretation of results
“Take-home” message #1Drug testing for pain managementREQUIRES synchronization between theclinic and the lab!oLittle standardization exists among laboratory teststodayoDrugs used in pain management have complicatedpharmacokinetics, interactions, and some are not “pure”oPatients are often “high risk”oConsequences of false positive or false negativeresults are severe, for all involved
Lab definitions Screen: a qualitative (positive/negative) test;usually designed to detect many drugs or drugclasses; confidence in results may be poor, butdepends on the assay. Commonly based onimmunoassay; may be accomplished with “point ofcare tests” (POCT). Confirmation: a test designed to provide a highdegree of confidence in identification of individualdrugs/compounds; may be qualitative orquantitative (reports the amount of drug present).Commonly based on a combination ofchromatography and mass spectrometry.
Selecting the best drug testDrug testing for pain management purposes shouldNOT mirror traditional drugs of abuse testing Objectives of testing are different Testing needs vary based on:– Patient population– Specific drug(s) of interest– Specimen– Sensitivity (cutoff)– Need for quantitative results– SpecificityScreenConfirm
Specificity and immunoassay resultsSPECIFICITYPoor FALSE negativeresultDefined by:Antibody,Cutoff, andCalibratorTRUE result,negative or positiveGood (forwrong drug) FALSE positiveresult
Substances with poor cross-reactivityDrug class esCompounds not detected Spice, K2MethylphenidateClonazepam, ZolpidemEDDPOxycodone, Fentanyl, Tramadol, BuprenorphinePossible FALSE negativeManchikanti et al, Pain Physician 13:E1-22, 2010Tenore, J of Addictive Diseases 29:436-48, 2010
Substances with good cross-reactivityDrug class taminesCompounds detected NSAIDs, PantoprazoleChlorpromazine, FluoroquinolonesOxaprozin, SertralinePropoxyphene, SeroquelDextromethorphan, MeperidineVicks, Desipramine, TrazodonePossible FALSE positiveChristoi et al, Pain Physician 14:123-43, 2011Tenore, J of Addictive Diseases 29:436-48, 2010
Detection limits reflectAssay method and cutoffDrug and formulationPatient pharmacokineticsSamplepositivecutoff– Type– Timing of collection– Quality of specimen(e.g. dilution)negative
Example: effect of urine dilution on drug screenAssume opiate cutoff of 300 ng/mLSamples contain 428 ng morphine/mg creatinineSample 1: positive– morphine: 856 ng/mL– creatinine: 200 mg/dLSample 2: negative– morphine: 214 ng/mL– creatinine: 50 mg/dL
Substitution may not be detectedSampleSample Check (%)Microgenics, CEDIACreatinine (mg/dL)Syva (Dade), EMITHuman urine80-100 5 (DOT)Dog urine (n 7)52 - 8587 - 28492104Energy drinks (n 44)72-1030-63Margarita mix (n 2)73-7471-76Fruit juice (n 8)39-810-62Horse urine (n 1)VP Villena, JAT 34:39-44, 2010
UDT in Pain ManagementResultsappropriateNo furtheraction, if patientis low riskUDTResults notappropriateConfirm results,specimen validityResultsappropriateNo furtheraction, if patientis low riskResults notappropriateConsidertest, drug, patient, and sampleConfirmation testing was required for 35%of POCT results in the Manchikanti 2011 studies
POCT in pain patientsDrug/Drug ClassSensitivitySpecificityAgreementMorphine, %Amphetamine47.0%99.1%98.2%Manchikanti et al, Pain Physician;14:175-87 & 259-70, 2011
When to “confirm” a result2nd immunoassay1. Screen results are inconsistentwith clinical expectationsChromatography2. Screen used does not detectthe drug(s) of interest3. Quantitative results arenecessary for interpretationMassspectrometry: GC-MS, LC-MS/MS, LC-MS/TOF
Interpretation:Evaluating negative and positive results
Reasons for a negative resulto Drug was not taken/administeredo Drug was taken incorrectly (less thanprescribed or less frequently than prescribed)o Drug delivery was variable Drugo Drug was not absorbed Patiento Accelerated metabolism/elimination Sampleo Specimen was collected too lateo Specimen was dilute, or adulterated Testo Clinic or lab mixupo Test performed is not designed to detect drug
“False” negatives for oxycodone commonDrug (ng/mL) Abbott Dade Roche BIOSITEFPIA Behring CEDIA Triage(Syva)DAUEMIT done10005,38810,00020,000The Clinical Toxicology Laboratory, AACC Press, 2003, pp. 491-2
Reasons for a positive resulto Drug was taken/administeredo Drug detected is an expected metabolite of aprescribed drug Drugo Drug detected is a process impurity Patiento Incorrect prescription filled Sampleo Prescription obtained elsewhere Testo Non-prescribed drug was usedo Drug was added to urine after collectiono Clinic or lab mixupo Result is a false positive (e.g., test specificity)
Interpreting concentrationsPatient results2033 ng/mL Morphine15 ng/mL HydromorphonePatient RxMS Contin (morphine sulfate)– Morphine is metabolizedto hydromorphone (minorpathway, 3% expected)– Thresholds forindependent use ofhydromorphone are notwell establishedCone et al JAT 32(4):319-23, 2008
Interpreting concentrations (cont.)Patient results2033 ng/mL Morphine15 ng/mL Hydromorphone8 ng/mL CodeinePatient RxMS Contin (morphine sulfate)
Simplified opioid metabolismcodeinehydrocodonepoppy romorphone* Not specifically detected by most assays
Interpreting concentrations (cont.)Patient results2033 ng/mL Morphine15 ng/mL Hydromorphone8 ng/mL CodeinePatient RxMS Contin (morphine sulfate)Codeine is not ametabolite of morphineor hydromorphoneCodeine can be animpurity in somemorphine preparations;up to 0.5% is allowedMRO Alert XXI, No. 3, 2010West et al, TDM 31(6):776-8, 2009
Opioid process itiesAllowablepharmaceuticalimpurity limit ycodone0.150.5MRO Alert XXI, No. 3, 2010
Interpretation:Detecting adulteration intended to mimicadherence to prescribed medications
Results suggesting drug was added to 00122,9203.81010,90073,0103.6McMillin et al., JAT, 2011, in pressNOTES:Glucuronides were 20 ng/mLExpected ratio ofBUP:Naloxone forSuboxone 4Average ratio ofBUP:Naloxone forthese patients: 4.4
Adulteration possible?
“Take-home” message #2Drug testing results should ALWAYS beinterpreted based on the clinicalscenario, including, but not limitedto, the drug, the patient, the sample, andthe test
Interpretation:Drug adherence vs. dose and dosingadherence
UDT cannot reliably evaluate dosingo Dose delivery may vary with formulationo Pharmacokinetics will vary by patiento Time of specimen collection vs. drug dosing is usually NAo Drug administration may or may not be timedo UDT specimens are not usually timed (prior collected void)o Urine varies based on hydration status, other medications,renal function, urine pH, etc.o Not all drug is eliminated in urineo UDT is based primarily on measurement of drugmetabolites which can arise from more than one drugo Routine/chronic administration of a drug affects the amountof drug and drug metabolites observed in the urineo Laboratory methods vary
Expected urine findingsParent drug% of a doseeliminated inthe urine within72 hrs% of a doseeliminated asFREE parent drug% of a doseeliminated asglucuronideconjugate ofparent drugMorphine 87% 10% 75%Hydrocodone 26% 12%NAHydromorphone 50% 6% 30%Oxycodone 72% 5%NAOxymorphone 49% 2% 44%Buprenorphine 27% 1% 9.4%Fentanyl 85% 6%NABaselt RC, Disposition of Toxic Drugs and Chemicals in Man, 8th Ed, 2008
Hydrolysis efficiency for morphinePercent (%) recovery of opioids usingdifferent hydrolysis methodsMorphineMetaboliteChemical(acid)Enzyme(P. vulgata, 2 hrs)Enzyme(H. pomatia, 16 hrs)Morphine-3glucuronide100 494 250 13Morphine-6glucuronide98 512 10 0Patient urine100 064 1935 20Wang et al, JAT 30:570-5, 2006
Urine concentrations with Duragesic 25 µg/h50 µg/h75 µg/h100 0-8604-13300-167014218485135FentanylMean (ng/mL)Range of central 90%NorfentanylMean (ng/mL)Range of central 90%Number of samplesPoklis and Backer, JAT 28:422-5, 2004
End of dose failure 1000 outpatients prescribed transdermal fentanylpatches for pain management 50% needed more analgesia before the end ofthe standard 72 hour dose period Average pain control was 63 hrsKim et al, Support Care Cancer 19(2):297-301, 2010Suggests variation in actual drug delivery and/orpatient pharmacokineticsSuggests random UDT may not verify adherence
“Take-home” message #3UDT cannot reliably determine thedose taken, or the frequency at whicha dose was taken
Conclusionso UDT has become an important part of routine painmanagement practiceso UDT offers many useful opportunities to identify andevaluate recent drug useo Testing technologies and frequency of testing shouldbe aligned with clinical needs/expectationso Results should be interpreted in the context of thetest, drug(s), patient, and sample(s) testedo Unexpected positive or negative results should bediscussed with the patient, and confirmed if neededo Dose and dosing of a drug cannot be reliablydetermined by UDT
Pain relievers are the #1 new illicit drug in the U.S. National Survey on Drug Use in Health (NSDUH), 2009 It is estimated that 20% of Americans have used prescription drugs for nonmedical reasons; including 15% of 12th graders www.drugabuse.gov 60% of people who use pain relievers for nonmedical reasons obtain the drug from a friend