Transcription
Payer ID: 86052, 33628Mercy Care PlanMercy Care Regional Behavioral Health Authority (RBHA)835EDI Enrollment Instructions: Please save this document to your computer. Open the file in the Adobe Reader program and typedirectly onto the form. Complete the form using the provider’s billing/group information as credentialed with this payer. Once completed, save for your records, print and obtain appropriate signature(s). EDI enrollment processing timeframe is approximately 30 business days. To check status of EDI enrollment, please contact Mercy Care at 800-624-3879.837 Claim Transactions:EDI enrollment applies to ERA only and is not necessary prior to sending claims.835 Electronic Remittance Advice:Mercy Care Electronic Remittance Advice Authorization AgreementComplete all applicable fields.NOTE: There are two Change Healthcare Remittance forms enclosed. Only submit the form applicableto the Type of business you are credentialed for: Professional OR Institutional. Only submit both ifyour practice is credentialed for both types of business.Submit Completed Document:Email to Mercy Care sinc.com2020-04-29
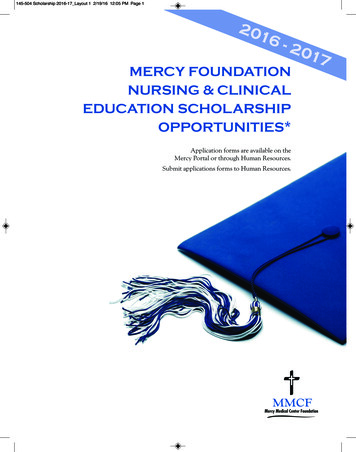
Send completed form to:Batchenrollment@changehealthcare.comFax: (615) 885-3713RemittancePayer InformationCPID3433Payer ID Payer86052TypeMERCY CARE PLAN of ARIZONAProfessionalEst DaysMulti CH14NoSpecial Enrollment InstructionsForms must be sent directly to the payer for processing. Payer contactinformation can be found on the enrollment. Forms that are received atChange Healthcare will be rejected.Vendor Information*460477436,,*Submitter IDSubmitter NameClaimRemedi460477436Provider InformationTax IDNPIProvider NumberAddressNameCityContact NameContact PhoneContact Email AddressConfirmation AddressesPrimary Email AddressSecondary Email AddressEnrollment@claimremedi.comERA ReceiverDistribution DetailclmremedFor Change Healthcare use onlyState Zip
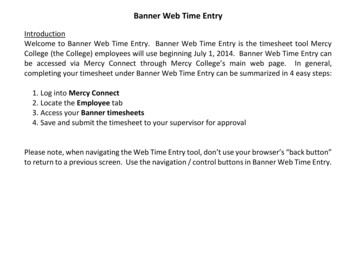
Send completed form to:Batchenrollment@changehealthcare.comFax: (615) 885-3713RemittancePayer InformationCPID3530Payer ID Payer86052TypeMERCY CARE PLAN of ARIZONAInstitutionalEst DaysMulti CH14NoSpecial Enrollment InstructionsForms must be sent directly to the payer for processing. Payer contactinformation can be found on the enrollment. Forms that are received atChange Healthcare will be rejected.Vendor Information*460477436,,*Submitter IDSubmitter NameClaimRemedi460477436Provider InformationTax IDNPIProvider NumberAddressNameCityContact NameContact PhoneContact Email AddressConfirmation AddressesPrimary Email AddressSecondary Email AddressEnrollment@claimremedi.comERA ReceiverDistribution DetailclmremedFor Change Healthcare use onlyState Zip
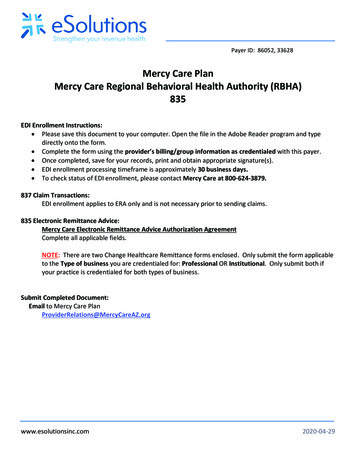
602-263-3000/ 1-800-624-3879Fax 860-975-3201Electronic Remittance Advice (ERA) Authorization AgreementPage 2 – Definitions for DEG group data elements contained in Appendix.DEG1PROVIDER INFORMATIONProvider NameDoing Business As Name(DBA)Provider AddressStreetCityState/ProvinceZip Code/Postal CodeDEG2PROVIDER IDENTIFIERS INFORMATIONProvider Federal Tax IdentificationNumber (TIN) or EmployerIdentification Number (EIN)National Provider Identifier(NPI)DEG3PROVIDER CONTACT INFORMATIONProvider Contact NameTelephone NumberEmail AddressFax NumberDEG7ELECTRONIC REMITTANCE ADVICE INFORMATIONPreference For Aggregation of Remittance Data (e.g., Account Number Linkage to Provider Identifier) - Select frombelowProvider Tax Identification Number(TIN)National Provider Identifier(NPI)Method of Retrieval ClearinghouseDEG8ELECTRONIC REMITTANCE ADVICE CLEARINGHOUSE INFORMATIONClearinghouse Name EmdeonClearinghouse ContactEnrollment Help DeskNameTelephone Number 866-924-4634Email Address ION INFORMATIONReasons For Submission – Select from belowNew EnrollmentChange EnrollmentCancel Enrollment
602-263-3000/ 1-800-624-3879Fax 860-975-3201Electronic Remittance Advice (ERA) Authorization AgreementPage 3 – Definitions for DEG group data elements contained in Appendix.Authorized SignatureWritten Signature of PersonSubmitting EnrollmentPrinted Name of PersonSubmitting EnrollmentPrinted Title of PersonSubmitting EnrollmentAuthorization Agreement – By signing above, I hereby agree that I have read and agree to the terms and conditionsstated in the Authorization Agreement below.Authorization AgreementElectronic Remittance Advice (ERA)An ERA is an electronic version of a payment explanation of benefits (EOB) explaining claims payment or denial.This authorization is to remain in effect until Mercy Care has received an ERA cancellation notification from me thataffords Mercy Care a reasonable opportunity to act on it. Please allow 10-15 business days for processing onceenrollment is received. Processing times may vary depending on number of enrollments received, accuracy of theinformation provided and how legible the form is.Additional Required Information For Enrollment – MUST BE COMPLETED ERA Receiver Information**Receiver IDDistribution Method PXVW LQGLFDWH RQH PHWKRG 460477436 )73 ,QWHUQHW /RJ ,' FKDUDFWHUV 762 ,' 1'0V 1RGH 1DPH XQLTXH YHQGRU ,' ORZHUFDVH &KDQJH HDOWKFDUH 2IILFH HPDLO DGGUHVV &KDQJH HDOWKFDUH 3D\PHQW 0DQDJHUDistributionclmremedERA Receiver Information and Distribution Method Choices**:1. ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Office*** is a suite of ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ practice management products, which includes aŵƵůƚŝƵĚĞ ŽĨ provider products. ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Office should only be selected if you as the provider use thesuite of ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Office practice management products.2. FTP Internet- this may be an FTP log on or it may be used to list the payment manager connection. MEDICOMis the distribution method when using payment manager.3. TSO Mailbox- this is a dial up connection.4. NDM S Node- this is typically used for 837 claim submissions.5. ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Payment Manager – Enter Payment Manager as the Receiver ID even if enrolling for PaymentManager as part of this ERA enrollment.
602-263-3000/ 1-800-624-3879Fax 860-975-3201Additional Information Required If Enrolling in ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Payment Manager – Offered at noadditional cost&KHFN WKH FRUUHFW ER[ WR LQGLFDWH D 3D\PHQW 0DQDJHU UHTXHVW ,I 3D\PHQW 0DQDJHU GRHV D 8VHU ,' DOUHDG\ H[LVW" HV 1R %RWK (5 DQG 3D\PHQW 0DQDJHU HV 1R 3D\PHQW 0DQDJHU 8VHU ,' Additional National Provider Identification (NPI) to be NPIGeneral Reference InformationPayer InformationPayer ID:Mercy Care Ͳ 86052 DĞƌĐLJ Z , Ͳ ϯϯϲϮϴTax ID:86-0ϱϳϳϯϴϭ ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ Confirmations – Internal Use OnlySend ŚĂŶŐĞ ,ĞĂůƚŚĐĂƌĞ 835 enrollment confirmations to:ProviderRelations@MercyCareAZ.orgPrint
An ERA is an electronic version of a payment explanation of benefits (EOB) explaining claims payment or denial. This authorization is to remain in effect until Mercy Care has received an ERA cancellation notification from me that affords Mercy Care a reasonable opportunity to act on it. Please allow 10-15 business days for processing once