Transcription
DELAWAREPEDIATRIC DENTAL AND VISIONCOVERAGE BENEFITSUMMARYFOR SMALL GROUPSEffective January 1, 2022
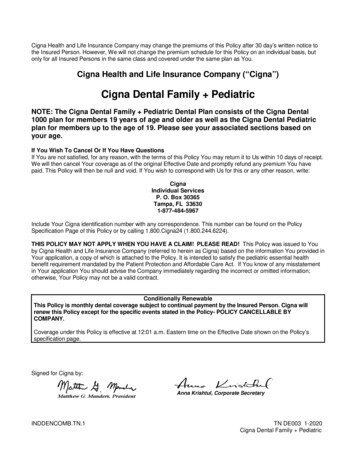
HIGHMARK BLUE CROSS BLUE SHIELD DELAWARE: SMALL GROUP ACA– 50 OR FEWER EMPLOYEES2022 Pediatric Vision Coverage Benefit SummaryNETWORK BENEFIT (Independents & Visionworks)*FREQUENCYELIGIBLE PARTICIPANTSMembers under 19 years of age(1)Eye examination (including dilation, as professionally indicated)Once every 12 monthsEyeglass lensesOnce every 12 monthsFrames**Once every 12 months**PLAN RESPONSIBILITYEYE EXAMINATION(including dilation, as professionally indicated)These benefitsapply toQualifiedHigh-DeductibleHealth Plans(QHDHP).100%FRAMESPediatric frame selectionEYEGLASS LENSES(2)100% after deductible(Per Pair)Single vision100% after deductibleBifocal100% after deductibleTrifocal100% after deductibleLenticular100% after deductibleVALUE ADDED BENEFITSLens options purchased from a participating providerwill be provided to the member at the amounts listed below.MEMBER RESPONSIBILITYLENS OPTIONSStandard progressive lenses (3) 50Premium progressive lenses 90(3)Polycarbonate lenses 0Intermediate vision lenses 30High-index (thinner and lighter) lenses 55Polarized lenses 75Fashion, sun, or gradient-tinted plastic lenses 11Ultraviolet coating 12Scratch-resistant coating 0Scratch Protection Plan Single Vision 20Scratch Protection Plan Multifocal 40Standard ARC (anti-reflective coating) 35Premium ARC (anti-reflective coating) 48Ultra ARC (anti-reflective coating) 60OPTIONAL EYEGLASS LENSES/COATINGS/TREATMENTS (per pair)Dependents will beterminated from visioncoverage at the end of themonth in which they turn 19.(2) Includes glass, plastic, oroversized lenses.(3) Progressive multifocals canbe worn by most people.Conventional bifocalswill be supplied at noadditional charge for anyonewho is unable to adapt toprogressive lenses. However,the member’s paymenttowards the progressiveupgrade will notbe refunded.(4) Disposable contact lenswearers will receive fourmultipacks of lenses.Planned replacement lenswearers will receive twomultipacks of lenses.* Vision benefits utilize theDavis Vision Network. Thereis no out-of-network coverage.Davis Vision is a separatecompany that administersHighmark vision benefits.Visionworks, also a separatecompany, is a provider withinthe Davis Vision Network.** Subject to deductible.(1) MEMBER RESPONSIBILITYCONTACT LENSES (in lieu of eyeglass lenses - per pair or initial supplyof disposable contact lenses from the pediatric contact lens selection)Contact lens evaluation and fittingDaily wearCovered in full when the performing providerdispenses from the pediatric contact lens selectionExtended wearCovered in full when the performing providerdispenses from the pediatric contact lens selectionPediatric contact lens selection (4)Standard daily wear contact lensesCovered In FullSpecialty contact lensesCovered In FullDisposable contact lensesCovered In FullMedically necessary contact lenses (prior approval required)Covered In Full1
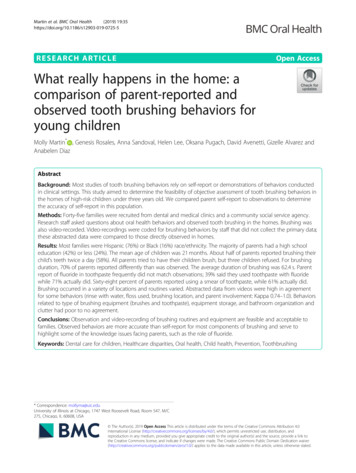
HIGHMARK BLUE CROSS BLUE SHIELD DELAWARE: SMALL GROUP ACA– 50 OR FEWER EMPLOYEES2022 Pediatric Vision Coverage Benefit SummaryNETWORK BENEFIT (Independents & Visionworks)*FREQUENCYELIGIBLE PARTICIPANTSMembers under 19 years of age(1)Eye examination (including dilation, as professionally indicated)Once every 12 monthsEyeglass lensesOnce every 12 monthsFramesOnce every 12 monthsPLAN RESPONSIBILITYEYE EXAMINATION(including dilation, as professionally indicated)These benefitsapply toNon-QualifiedHigh-DeductibleHealth Plans(Non-QHDHP).100%FRAMESPediatric frame selectionEYEGLASS LENSES(2)100%(Per Pair)Single UE ADDED BENEFITSLens options purchased from a participating providerwill be provided to the member at the amounts listed below.MEMBER RESPONSIBILITYLENS OPTIONSStandard progressive lenses (3) 50Premium progressive lenses 90(3)Polycarbonate lenses 0Intermediate vision lenses 30High-index (thinner and lighter) lenses 55Polarized lenses 75Fashion, sun, or gradient-tinted plastic lenses 11Ultraviolet coating 12Scratch-resistant coating 0Scratch Protection Plan Single Vision 20Scratch Protection Plan Multifocal 40Standard ARC (anti-reflective coating) 35Premium ARC (anti-reflective coating) 48Ultra ARC (anti-reflective coating) 60OPTIONAL EYEGLASS LENSES/COATINGS/TREATMENTS (per pair)MEMBER RESPONSIBILITYDependents will beterminated from visioncoverage at the end of themonth in which they turn 19.(2) Includes glass, plastic, oroversized lenses.(3) Progressive multifocals canbe worn by most people.Conventional bifocalswill be supplied at noadditional charge for anyonewho is unable to adapt toprogressive lenses. However,the member’s paymenttowards the progressiveupgrade will notbe refunded.(4) Disposable contact lenswearers will receive fourmultipacks of lenses.Planned replacement lenswearers will receive twomultipacks of lenses.* Vision benefits utilize theDavis Vision Network. Thereis no out-of-network coverage.Davis Vision is a separatecompany that administersHighmark vision benefits.Visionworks, also a separatecompany, is a provider withinthe Davis Vision Network.(1) CONTACT LENSES (in lieu of eyeglass lenses - per pair or initial supplyof disposable contact lenses from the pediatric contact lens selection)Contact lens evaluation and fittingDaily wearCovered in full when the performing providerdispenses from the pediatric contact lens selectionExtended wearCovered in full when the performing providerdispenses from the pediatric contact lens selectionPediatric contact lens selection (4)Standard daily wear contact lensesCovered In FullSpecialty contact lensesCovered In FullDisposable contact lensesCovered In FullMedically necessary contact lenses (prior approval required)Covered In Full2
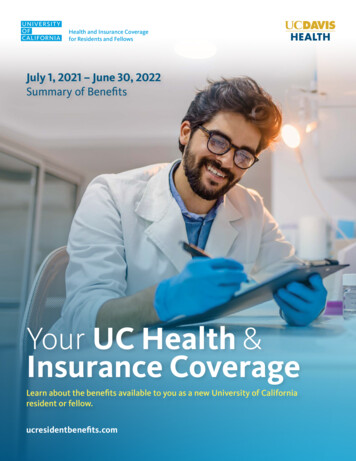
HIGHMARK BLUE CROSS BLUE SHIELD DELAWARE:SMALL GROUP ACA – 50 OR FEWER EMPLOYEES2022 Pediatric DentalCoverage Benefit SummaryThese benefits apply toQualified High-DeductibleHealth Plans (QHDHP).Contract Year Deductible per member:Combined with MedicalThis plan meets the minimum essential health benefitrequirements for pediatric oral health as required under theFederal Affordable Care Act.These benefits are only available for children through the end ofthe benefit period that they turn 19.Annual Maximum per member:UnlimitedThis plan will pay benefits for covered services shown belowsubject to exclusions and other policy terms. Payment is based onthe plan allowance for the specific covered service. Participatingdentists accept contracted plan allowance as payment in fullfor services.Out-of-Pocket (OOP) Year Maximumper member:Combined with MedicalSERVICE CATEGORYPOLICY PAYSWAITINGIN-NETWORKPERIODDENTISTS*POLICY PAYSOUT-OF-NETWORKDENTISTSAFTERDEDUCTIBLEOral Evaluations (Exams)None100%Not CoveredNoRadiographs (All X-rays)None100%Not CoveredNoProphylaxis (Cleanings)None100%Not CoveredNoFluoride TreatmentsNone100%Not CoveredNoPalliative Treatment (Emergency)NoneCoinsurance matches medical coinsuranceNot CoveredYesSealantsNone100%Not CoveredNoSpace MaintainersNone100%Not CoveredNoBasic Restoration Anterior AmalgamNoneCoinsurance matches medical coinsuranceNot CoveredYesBasic Restoration Anterior Composite NoneCoinsurance matches medical coinsuranceNot CoveredYesBasic Restoration Posterior Amalgam NoneCoinsurance matches medical coinsuranceNot CoveredYesCrowns, Inlays, OnlaysNoneCoinsurance matches medical coinsuranceNot CoveredYesCrown RepairNoneCoinsurance matches medical coinsuranceNot CoveredYesEndodontic Therapy(Root canals, etc.)NoneCoinsurance matches medical coinsuranceNot CoveredYesSurgical PeriodonticsNoneCoinsurance matches medical coinsuranceNot CoveredYesNon-Surgical PeriodonticsNoneCoinsurance matches medical coinsuranceNot CoveredYesPeriodontal MaintenanceNoneCoinsurance matches medical coinsuranceNot CoveredYesNoneCoinsurance matches medical coinsuranceNot CoveredYesNoneCoinsurance matches medical coinsuranceNot CoveredYesMaxillofacial ProstheticsN/ANot CoveredNot CoveredN/AImplant ServicesNoneCoinsurance matches medical coinsuranceNot CoveredYesSimple ExtractionsNoneCoinsurance matches medical coinsuranceNot CoveredYesSurgical ExtractionsNoneCoinsurance matches medical coinsuranceNot CoveredYesOral SurgeryNoneCoinsurance matches medical coinsuranceNot CoveredYesGeneral Anesthesia, Nitrous Oxide,and/or IV SedationNoneCoinsurance matches medical coinsuranceNot CoveredYesConsultationsNoneCoinsurance matches medical coinsuranceNot CoveredYesMedically Necessary OrthodonticsNoneCoinsurance matches medical coinsuranceNot CoveredYesProsthetics(Complete or Fixed Partial Dentures)Adjustments and Repairs ofProsthetics* Pediatric dental benefits utilize the United Concordia Advantage Plus 2.0 Network. Members must use a United Concordia provider. There is no out-of-network coverage for thisbenefit. United Concordia Companies, Inc., is a separate company that administers pediatric dental benefits for Highmark members.3
Dentally Necessary Orthodontics CoverageCoverage of Dentally Necessary OrthodonticsIn this section, “Dentally Necessary” shall mean dentalservices determined by a Dentist to either establish ormaintain a patient’s dental health based on the professionaldiagnostic judgment of the Dentist and the prevailingstandards of care in the professional community. Thedetermination will be made by the Dentist in accordancewith guidelines established by the Plan.1. Orthodontic treatment must be Dentally Necessaryand be the only method capable of:Orthodontic treatment limitations:2. Insured members must have a fully erupted set ofpermanent teeth to be eligible for comprehensive,Dentally Necessary orthodontic services.a) preventing irreversible damage to the Insuredmember’s teeth or their supporting structures and,b) restoring the Insured member’s oral structure tohealth and function.1. All pediatric orthodontic treatment is subject toPre-certification by the Plan, and must be part ofan approved written plan of care.3. All Dentally Necessary orthodontic services requireprior approval and a written plan of care.2. To be eligible for pediatric orthodontic treatment,a Member musta) continue to be enrolled during the duration oftreatment; andb) have a fully erupted set of permanent teeth3. Orthodontics Covered Services which are intendedto treat a severe dentofacial abnormality and are the onlymethod capable of preventing irreversible damage tothe Member’s teeth or their supporting structures, andrestoring the Member’s oral structure to healthand function.A Dentally Necessary orthodontic service is an orthodonticprocedure that occurs as part of an approvedorthodontic plan that is intended to treat a severedentofacial abnormality.4
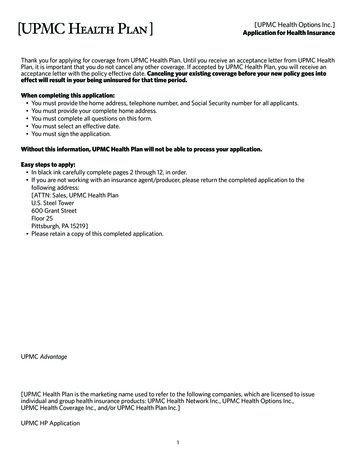
HIGHMARK BLUE CROSS BLUE SHIELD DELAWARE:SMALL GROUP ACA– 50 OR FEWER EMPLOYEES2022 Pediatric DentalCoverage Benefit SummaryThese benefits apply toNon-Qualified High-DeductibleHealth Plans (Non-QHDHP).Contract Year Deductible per member: 0This plan meets the minimum essential health benefitrequirements for pediatric oral health as required under theFederal Affordable Care Act.These benefits are only available for children through the end ofthe benefit period that they turn 19.Annual Maximum per member:UnlimitedThis plan will pay benefits for covered services shown belowsubject to exclusions and other policy terms. Payment is based onthe plan allowance for the specific covered service. Participatingdentists accept contracted plan allowance as payment in fullfor services.Out-of-Pocket (OOP) Year Maximumper member:Combined with MedicalSERVICE CATEGORYWAITINGPERIODPOLICY PAYSIN-NETWORKDENTISTS*POLICY PAYSOUT-OF-NETWORKDENTISTSAFTERDEDUCTIBLEOral Evaluations (Exams)None100%Not CoveredN/ARadiographs (All X-rays)None100%Not CoveredN/AProphylaxis (Cleanings)None100%Not CoveredN/AFluoride TreatmentsNone100%Not CoveredN/APalliative Treatment (Emergency)None100%Not CoveredN/ASealantsNone100%Not CoveredN/ASpace MaintainersNone100%Not CoveredN/ABasic Restoration Anterior AmalgamNone50%Not CoveredN/ABasic Restoration Anterior CompositeNone50%Not CoveredN/ABasic Restoration Posterior AmalgamNone50%Not CoveredN/ACrowns, Inlays, OnlaysNone50%Not CoveredN/ACrown RepairNone50%Not CoveredN/AEndodontic Therapy (Root canals, etc.)None50%Not CoveredN/ASurgical PeriodonticsNone50%Not CoveredN/ANon-Surgical PeriodonticsNone50%Not CoveredN/APeriodontal MaintenanceNone50%Not CoveredN/AProsthetics(Complete or Fixed Partial Dentures)None50%Not CoveredN/AAdjustments and Repairs of ProstheticsNone50%Not CoveredN/AMaxillofacial ProstheticsN/ANot CoveredNot CoveredN/AImplant ServicesNone50%Not CoveredN/ASimple ExtractionsNone50%Not CoveredN/ASurgical ExtractionsNone50%Not CoveredN/AOral SurgeryNone50%Not CoveredN/AGeneral Anesthesia, Nitrous Oxide,and/or IV SedationNone50%Not CoveredN/AConsultationsNone100%Not CoveredN/AMedically Necessary OrthodonticsNone50%Not CoveredN/A* Pediatric dental benefits utilize the United Concordia Advantage Plus 2.0 Network. Members must use a United Concordia provider. There is no out-of-network coverage for thisbenefit. United Concordia Companies, Inc., is a separate company that administers pediatric dental benefits for Highmark members.5
Dentally Necessary Orthodontics CoverageCoverage of Dentally Necessary OrthodonticsIn this section, “Dentally Necessary” shall mean dentalservices determined by a Dentist to either establish ormaintain a patient’s dental health based on the professionaldiagnostic judgment of the Dentist and the prevailingstandards of care in the professional community. Thedetermination will be made by the Dentist in accordancewith guidelines established by the Plan.1. Orthodontic treatment must be Dentally Necessaryand be the only method capable of:Orthodontic treatment limitations:2. Insured members must have a fully erupted set ofpermanent teeth to be eligible for comprehensive,Dentally Necessary orthodontic services.a) preventing irreversible damage to the Insuredmember’s teeth or their supporting structures and,b) restoring the Insured member’s oral structure tohealth and function.1. All pediatric orthodontic treatment is subject toPre-certification by the Plan, and must be part ofan approved written plan of care.3. All Dentally Necessary orthodontic services requireprior approval and a written plan of care.2. To be eligible for pediatric orthodontic treatment,a Member musta) continue to be enrolled during the duration oftreatment; andb) have a fully erupted set of permanent teeth3. Orthodontics Covered Services which are intendedto treat a severe dentofacial abnormality and are theonly method capable of preventing irreversible damageto the Member’s teeth or their supporting structures,and restoring the Member’s oral structure to healthand function.A Dentally Necessary orthodontic service is an orthodonticprocedure that occurs as part of an approvedorthodontic plan that is intended to treat a severedentofacial abnormality.6
Highmark Blue Cross Blue Shield Delaware is an independent licensee of theBlue Cross Blue Shield Association.To find more information about Highmark’s benefits and operating procedures,such as accessing the drug formulary or using network providers, please go toDiscoverHighmark.com/QualityAssurance; or for a paper copy, call 1-855-873-4109.Discrimination is Against the LawThe Claims Administrator/Insurer complies with applicable Federal civil rightslaws and does not discriminate on the basis of race, color, national origin, age,disability, or sex. The Claims Administrator/Insurer does not exclude people ortreat them differently because of race, color, national origin, age, disability, or sex.The Claims Administrator/Insurer: Provides free aids and services to people with disabilities to communicateeffectively with us, such as:– Qualified sign language interpreters– Written information in other formats (large print, audio, accessible electronicformats, other formats) Provides free language services to people whose primary language is notEnglish, such as:– Qualified interpreters– Information written in other languagesIf you need these services, contact the Civil Rights Coordinator.If you believe that the Claims Administrator/Insurer has failed to providethese services or discriminated in another way on the basis of race, color,national origin, age, disability, or sex, you can file a grievance with: Civil RightsCoordinator, P.O. Box 22492, Pittsburgh, PA 15222, Phone: 1-866-286-8295, TTY:711, Fax: 412-544-2475, email: CivilRightsCoordinator@highmarkhealth.org. Youcan file a grievance in person or by mail, fax, or email. If you need help filing agrievance, the Civil Rights Coordinator is available to help you. You can also filea civil rights complaint with the U.S. Department of Health and Human Services,Office for Civil Rights electronically through the Office for Civil Rights ComplaintPortal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail orphone at:U.S. Department of Health and Human Services200 Independence Avenue, SWRoom 509F, HHH BuildingWashington, D.C. 202011-800-368-1019, 800-537-7697 (TDD)Complaint forms are available at 21 Z MX965230
Highmark vision benefits. Visionworks, also a separate company, is a provider within the Davis Vision Network. These benefits apply to Non-Qualified High-Deductible Health Plans (Non-QHDHP). 2022 Pediatric Vision Coverage Benefit Summary HIGHMARK BLUE CROSS BLUE SHIELD DELAWARE: SMALL GROUP ACA- 50 OR FEWER EMPLOYEES