Transcription
AMA Guides N E W S L E T T E RUpdates, authoritative guidance, practical information,and rationales for proper use of AMA GuidesIN THIS ISSUERating Survivors of COVID-19 forPermanent Impairment . . . . . . . . . . 3Medical Aspects of Causation forCOVID-19 . . . . . . . . . . . . . . . . . . 8Q&A: Cervical Facet Arthropathy . . 12Q&A: The Role of the QuickDASH inCarpal Tunnel Syndrome . . . . . . . 14July/August 2020Volume 25 Issue 4
AMA Guides NewsletterAdvisory BoardCalendar of EventsEDITORChristopher R. Brigham, MD, MMSHilton Head, South CarolinaDATEACTIVITIESOngoingWeb-based IME and Guides TrainingLOCATIONORGANIZATIONImpairment.comFor further information about training, contact:AMAIAIMEASSOCIATE EDITORJames B. Talmage, MDCookeville, TennesseeABIMEADVISORY BOARDAAOSGunnar B.J. Andersson, MD, PhDChicago, IllinoisAmerican Medical Association (www.amastore.com) . . . . . . . . . . . . . . 800-621-8335International Academy of Independent Medical Evaluators(www.iaime.org) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 312-663-1171American Board of Independent Medical Examiners(www.abime.org) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304-733-0095American Academy of Orthopaedics Surgeons (www.aaos.org) . . . . . . . . 847-823-7186Future Articles Overdiagnosis of Psychiatric DisabilityRobert J. Barth, PhDChattanooga, Tennessee Causation, Apportionment and SubstantialMedical Evidence in CaliforniaCharles N. Brooks, MDBellevue, WashingtonStephen L. Demeter, MD, MPHLas Vegas, NevadaLorne K. Direnfeld MD, FRCP(C)Kahului, HawaiiInterested in being an AMA Guides Newsletter contributor?Dwight K. Dowda, MB BS, MPHSydney, AustraliaLee H. Ensalada, MD, MPHTucson, ArizonaThe AMA is looking for impairment evaluationsubject matter experts willing to share originalarticles, case studies, legal findings, questionsand answers, and/or books or resources review.Marjorie Eskay-Auerbach, MD, JDTucson, ArizonaSteven Feinberg, MDPalo Alto, CaliforniaLuAnn Haley, JDTucson, ArizonaTo become a contributor, send your materials forpotential publication to Guides6@ama-assn.org.Richard T. Katz, MDSt. Louis, MissouriLes Kertay, PhDChattanooga, Tennessee 2020 American Medical Association. All Rights Reserved.Order InformationJ. Mark Melhorn, MDWichita, Kansas1 year (6 issues)AMA members. . . . . . . 150Nonmembers. . . . . . . 2002 years (12 issues)AMA members. . . . . . . 240Nonmembers. . . . . . . 320Back IssuesAMA members. . . . . . . 19.95Nonmembers. . . . . . . 29.95Phone Orders and Change of Address: Call (800) 621-8335If you have any concerns regarding and/or if you did not receive your issue of the GuidesNewsletter, email Guides6@ama-assn.org.Kathryn L. Mueller, MD, MPHDenver, ColoradoMohammed I. Ranavaya, MD, JD, MSHuntington, West VirginiaRobert D. Rondinelli, MD, PhDDes Moines, IowaE. Randolph Soo Hoo, MD, MPHHonolulu, HawaiiAMA StaffLaurie A.S. McGrawSenior Vice PresidentHealth Solutions GroupDave SosnowVice President, Product ManagementLisa Chin-JohnsonSenior Developmental EditorMary Ann AlbaneseProduction SpecialistAsim AhmedMarketing ManagerAMA Guides Newsletter (ISSN 2642-0880) is a peer-reviewed publication that complements the AMA Guides series of reference and work books. The Newsletter is published six times a year by the American MedicalAssociation. Beginning with the July/Aug 2020 issue, the Newsletter will include volume and issue numbers inaddition to the bimonthly designation.2020 American Medical Association. All Rights Reserved. AMA,, AMA Guides and the distinctive “G” design are registered trademarks of the AMA.AMA trademarks and the contents of this publication may not be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise,without the prior written permission of the publisher.The contents of this publication represent the views of the author(s) and should not be construed tobe the views or policy of the AMA, or the institution with which the author(s) may be affiliated, unlessotherwise indicated.Cover Image: Getty Images Premium Access
Rating Survivors of COVID-19 for Permanent ImpairmentJames B. Talmage MD, Mark H. Hyman MD, Robert B. Snyder MDAMA Guides Newsletter. 2020; 25(4):0-00. tractThe current pandemic of COVID-19 cases includes cases identified in emergency medical technicians, nurses, physicians, andothers with occupational exposure to the SARS-CoV-2 virus. Many of these health care professionals have filed workers’ compensation claims that have been accepted. Each accepted claim will eventually need a physician to declare the individual “at maximalmedical improvement” or the equivalent phrase in the jurisdiction involved. The next step is for the physician to rate permanentimpairment, if present, so the case can be administratively closed. The AMA Guides to the Evaluation of Permanent Impairment(AMA Guides) is used by many jurisdictions, but the AMA Guides do not mention COVID-19 or have guidance on how to assessindividuals for impairment after recovery from this illness. This article provides preliminary guidance on rating permanent impairment within the respiratory, cardiac, vascular, neurologic, renal, gastrointestinal, and/or mental systems in COVID-19 survivors.Current references on the manifestations of COVID-19 illness in these body systems are included, which can be used as referencesto support documented impairment related to this illness.KEYWORDS: COVID-19; Coronavirus; Impairment rating; MMI;Outcome; PPI; SARS-CoV-2IntroductionAlmost everyone is aware of the presence of coronavirus2019 (COVID-19) illness, caused by the severe acuterespiratory syndrome coronavirus 2 (SARS-CoV-2).Classifying COVID-19 as an occupational illness iscontroversial, with several US states passing legislationgranting the rebuttable presumption of causation byworkplace exposure to some occupations (healthcareworkers, first responders, etc). This area of law is changing rapidly, and physicians will have to check the currentstatus of such law in the applicable jurisdiction to a casebefore them.Administrative requests for impairment ratingsbefore literature is published on the long-term outcomes in COVID-19 survivors will be seen in the nearfuture. Because many journals use a two-year outcomeassessment as a criterion for “long-term” outcomes,the information in this article should be considered as“interim advice.”Individuals who claim to have had COVID-19 but whotested negative for the virus by polymerase chain reaction(PCR), and individuals who state they were ill and werenot permitted to be tested, will likely have to have thecausation question formally adjudicated before physiciansare asked to assess for maximal medical improvement(MMI) and permanent physical impairment (PPI).For those cases either accepted by a workers’ compensation insurer or administratively adjudicated as workcompensable, these questions will need to be answered:When is the person at MMI? How should PPI be rated?We offer several clinical scenarios to consider for administratively accepted cases for which an MMI date and PPIrating are requested.Volume 25 Issue 3Clinical ScenariosScenario 1: Individuals who are tested when asymptomatic only because they are known contacts of a personwho tested positive. An example would be a healthcareworker in a hospital or nursing home with known caseswho is tested despite the absence of any symptoms. If thisindividual remains asymptomatic but did test positive onPCR for having the live virus, there are no known longterm complications in those with subclinical infection.These individuals can be considered to be at MMI a fewweeks after the positive test, and there is no permanentimpairment.Scenario 2: For those who are pre-symptomatic, ie, havenot yet become symptomatic at the time of testing but dolater become symptomatic, the average onset of illness isabout 2 to 5 days later.1, 2 These individuals would be ratedsimilar to the following scenarios 3 and 4.Scenario 3: Individuals who test positive and who havemild disease. They are not hospitalized, and they recoverat home, never having been significantly dyspneic. Oncerecovered, they are asymptomatic. When they canreturn to normal activity without symptoms, they canbe declared to be at MMI and with no PPI (0%). Thereare currently no case reports of individuals with milddisease, who recover at home, and yet who have persisting symptoms suggesting permanent consequences. Ifnecessary, to support this opinion, symptom validity canbe verified by stress echocardiography (eg, stress echocardiogram) and pulmonary function testing (PFT) (eg,spirometry).Scenario 4: Individuals who have moderate disease, ie,test positive, hospitalized, and treated with supplementaloxygen but are not placed in the intensive care unit (ICU)or on a ventilator. They usually have abnormal chest computed tomography (CT) scans and may have abnormalchest X rays. Some are more seriously ill and required anMay/June 2020 AMA Guides Newsletter3
Rating Survivors of COVID-19 for Permanent Impairment , continuedICU stay, or were placed on a ventilator, or both. In thesecases, review of hospital records is required to objectivelydocument the organ systems with objective pathology.The most common concern in these cases will be residual pulmonary or cardiac pathology either from the virusor from the ventilator. There may also be cases in whichsignificant pulmonary involvement was documented byoutpatient or emergency room imaging, and the personconvalesced at home. Psychological illness may also bepresent, which is discussed later in the article.For patients who required mechanical ventilationfor an acute respiratory distress syndrome (ARDS)illness, past experience has been that 50% of survivorsmay not have returned to work by 1 year from hospitaldischarge.5-9 They also point out that on spirometry, lungvolumes show about a 20% reduction that frequentlyresolves in 6 months. Thus, it would be logical to waituntil hospitalized survivors are 6 months from dischargebefore evaluating for MMI and PPI.HistoryBlood testing for complete blood count and comprehensive metabolic panel should be obtained unlessresults from prior convalescent testing are available andnormal.If residual pulmonary impairment is plausible, thenfull spirometry (including measurement of diffusioncapacity of carbon monoxide [DLCO], impendence testing, or nitrogen washout) should be obtained. The testresults should be evaluated to verify that they meet theAmerican Thoracic Society (ATS) criteria for full effortand reliability.10-12Pulmonary impairment can be rated using Table5-4, Criteria for Rating Permanent Impairment dueto Pulmonary Dysfunction (6th ed, p 88), in the AMAGuides to the Evaluation of Permanent Impairment(AMA Guides). In jurisdictions using the Fifth Editionof the AMA Guides, ratings come from Table 5-12,Impairment Classification for Respiratory Disorders,Using Pulmonary Function and Exercise Test Results (5thed, p 107). Many of the Sixth Edition internal medicine chapters have a footnote in the relevant table thatidentifies the “key factor” to be used for class assignment.Although Table 5-4 does not have such a footnote, onpage 87, it does indicate , “The examiner should note thatthroughout this chapter the objective test results are usedas the primary or ‘key factor’.”13 To be class 0, each of thespirometry results for which tests are available must benormal, as defined by the numbers in the table. For class1 to class 4 impairment, the worst of the tests determinesclass placement. Thus, if the DLCO results in a higher-class assignment than the forced vital capacity (FVC)or the forced expiratory volume in 1 second (FEV1), theclass would be determined by the DLCO result. ACOEMpoints out that lung diffusion abnormalities, if present,may take 5 years to resolve after ARDS. On spirometry,the DLCO is the test that best reflects diffusion abnormalities. There are no published studies of spirometryresults in COVID-19 survivors, but the pathophysiology so far appears to be predominantly diffuse alveolardamage, hyaline membranes, and microangiopathic processes.14 The DLCO may be the most impaired pulmonaryfunction on spirometry.Cardiovascular injuries that are seen in ARDSand could occur in COVID-19 include the followingconditions:If these individuals have persisting complaints of dyspnea on exertion or fatigue, the first assessment shouldbe face-to-face in an office setting (not via telemedicine).Using release-of-information forms to obtain recordsfrom the primary care physician before the onset ofCOVID-19 and from healthcare providers and hospitalsrelated to the treatment of COVID-19 will provide objective evidence of illness and help with questions aboutpre-existing status. Records should include evidence ofa positive PCR test for the presence of the virus. Chest Xray or chest CT scan results would confirm pulmonaryinvolvement occurred, as would physician-measuredoxygen saturation below 95%.Physical ExaminationThe physical examination should include traditionalpulmonary and cardiac assessments and pulse oximetry.An additional and simple in-office screening test is the6-minute walk test while the patient is wearing a pulseoximeter. Norms for distance walked by age are available,3but the most important information would be change inpulse from sitting to walking, and whether desaturation(oxygen level on pulse oximeter) occurs during walking.Tachycardia (pulse 100) and less than normal distancewalked with preserved oxygen saturation would suggestdeconditioning and not permanent impairment.GuidelinesThe American College of Occupational andEnvironmental Medicine (ACOEM) guidelines onCOVID-19 (April 24, 2020 update)4 contains a sectionon disability and return to work. They state that basedon prior experience with other similar viral illnesses,patients who recovered without hospitalization will generally be adequately recovered from post-infection fatigueand ready to return to work after 2 to 3 weeks. This isabout the time when some patients may be retested to seeif they are still shedding the virus. The clinical significance of a recovered patient still having viral sheddingis unclear and may not be a barrier to returning towork. For patients with documented pneumonia or whorequired supplemental oxygen therapy, recovery wouldbe estimated to be 4 to 8 weeks after hospitalization orclinical recovery.4AMA Guides Newsletter Volume 25 Issue 4Laboratory Testing
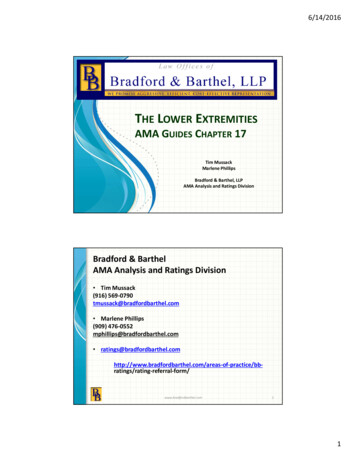
Rating Survivors of COVID-19 for Permanent Impairment , continuedConditionAMA Guides, Fifth EditionAMA Guides, Sixth EditionCardiomyopathyTable 3-9, page 47Table 4-7, page 59ArrhythmiaTable 3-11, page 56Table 4-9, page 64Cardiac muscle injuryTable 3-6a, page 36Table 4-6, page 55Pulmonary emboliTable 4-6, page 79Table 4-14, page 72Carotid occlusionChapter 13 or possibly by analogy, Table4-3, page 70Chapter 13Deep vein thrombosisTable 4-5, page 76Table 4-12, page 69Desaturation during exercise with normal spirometrywould suggest impaired cardiac output (left ventricle ejection fraction (LVEF) by echocardiogram) orinterstitial lung disease for which full metabolic stressechocardiogram would be needed. If the echocardiogramis normal, then other systemic illness such as anemiaor lung abnormalities are most likely. If the spirometrywas normal, but stress testing showed the individualcrossed the aerobic threshold (first ventilatory thresholdon cardiopulmonary stress exercise testing ([CPX])15 ormetabolic stress echocardiogram) and the subsequentmaximum oxygen (VO2 max) consumption was abnormal, the VO2 max measurement mentioned in eitheredition of the AMA Guides can be used for class assignment (6th ed, Table 5-4; 5th ed, Table 5-12). The formalinterpretation for the test may provide evidence as to thepathophysiology of the individual (lung diffusion abnormality, pulmonary hypertension, reduced cardiac output,deconditioning or lack of effort on testing, etc).COVID-19 patients can have cardiac complications.Some COVID-19 patients have ST-segment elevation onelectrocardiogram (EKG) and have corresponding clotsin major epicardial coronary arteries from the hypercoagulable state many of these patients experience.16 Thesepatients can be rated as any other myocardial infraction patient. Some have viral myocarditis without largeartery induced infarcts.17 These patients can be rated asany other cardiomyopathy patient. LVEF by echocardiogram or cardiac catheterization); brain natriureticpeptide (BNP) level, METs of exertion achieved on atreadmill test, or VO2 max on CPX or metabolic stressechocardiogram (if performed) are the test results discussed in the Sixth Edition, that are used as key factorsto assign a class.Pulmonary emboli may occur due to a hypercoagulable state18 or prolonged inactivity.19 Impairment would beevaluated by spirometry (infarction-reduced FVC) andby echocardiogram or metabolic stress echocardiogramshowing pulmonary hypertension.There are patients having large-vessel strokes, presumably due to the hypercoagulable state known to occur insome patients with COVID-19.20 These would be ratedlike any other large-vessel stroke, and if cranial nerve orvisual impairment is present, they would be rated according to Chapters 11 and 12 in either AMA Guides edition.Volume 25 Issue 3Some severely ill patients with COVID-19-related ARDShave neurologic deficits while in the ICU, and some stillhave mental status alteration in short-term follow up.21The AMA Guides point out that the more subtle thepersisting mental status deficit is, the more likely formal neuropsychological testing is to formally verify anddocument the deficit (6th ed, Section 13.3d, 330; 5th ed,Section 13.3d, 319).An unusual symptom being reported in some individuals with COVID-19 is anosmia, or loss of sense of smell.It is not clear from early reports whether this is just lossof sense of smell, or whether there is also loss of taste.Most of our sense of what food tastes like is determinedby our sense of smell. Subjective loss of sense of smellis not always validated on testing. Loss of sense of smellfrom upper respiratory tract infections (URTIs) is knownto recover in 32 to 66% of cases,22 so olfaction should betested with the University of Pennsylvania smell identification test (UPSIT) or the Burghardt Sniffin’ Sticks.Guillain-Barré syndrome and its variants have beenreported during and just after COVID-19 illness, 23, 24 andthese are ratable using the chapter on the central andperipheral nervous system in both the AMA Guides, Fifthand Sixth Editions. This diagnosis should not be usedfor subjective complaints of weakness and fatigue withno objective documentation of Guillain-Barré actuallybeen present, by accepted criteria.25 The residual respiratory and limb consequences of objectively documenteddisease are ratable.Note that the central and peripheral nervous systemchapter also has a rating methodology for myopathy26or for generalized peripheral neuropathy (Section 13-9in either edition) that could be used in cases of theseproblems after objective documentation with electrodiagnostic tests and/or muscle ultrasound or magneticresonance imaging (MRI) during the acute illness.27, 28While COVID-19 patients may have a hypercoagulable state (elevated D-dimer, etc) there are no currentreports of persistent hypercoagulable state after recovery.Individuals with a persisting or permanent hypercoagulable state (6th ed, Table 9-12, or 5th ed, Table 9-4) maybe rated, but this will probably not be used in COVID-19survivors. If thrombosis of a vessel(s) resulted in extremitycomplications, these would be rated using the extremitychapters. Similarly, if thrombosis in abdominal vesselsJuly/August 2020 AMA Guides Newsletter5
Rating Survivors of COVID-19 for Permanent Impairment , continuedoccurred, it would be rated from the gastrointestinal (GI)or genitourinary (GU) chapter(s).Acute hepatic injury and acute kidney injury, whenthey occur in patients with COVID-19, are usually markers of impending death, and survival with impairments inthese organs is not common.29 If an individual did survivethese complications, they are ratable from the GI and GUchapters, like any other liver or kidney disease patient.Providing care to COVID-19 patients can be stressful;30, 31 some individuals may present with post-traumaticstress disorder (PTSD) symptoms. Some had actualCOVID-19, some were first responders or healthcareworkers who witnessed first-hand illness or deaths, 32-34and some had both of these experiences. Several stateshave created a legal presumption (sometimes rebuttable)that PTSD in these situations is presumed to have beencaused by COVID-19.The mental and behavioral disorders chapter uses thenow antiquated DSM-IV-TR criteria for PTSD diagnosis,and most mental health professionals are now using themore liberal diagnostic criteria in DSM-V. If the diagnosis is administratively accepted, and the MMI and PPIquestions are asked, there are some caveats. Chapter 14in either edition of the AMA Guides is largely silent abouthow MMI and permanency are to be objectively established in mental disorders. Modern systematic reviewsindicate cognitive behavioral therapy (CBT) has betteroutcomes compared to medications35-37 and, therefore,12 to 18 sessions of CBT should logically have occurredbefore MMI is established. A further consideration isthe stability of employment. If the individual is still in a“temporary” off-work status, the outcome of PTSD witha change in employment is not known. Thus, if a healthcare worker is still unwilling to return to work after CBT,an alternate career choice may need to be made, and PPIshould logically be assessed after re-employment.For jurisdictions that apportion, the mental andbehavioral disorders chapter recommends that the ratingbe performed twice, once using three assessment toolsbased on symptoms and function before the incitingworkplace exposure, and then using the same tools todescribe the current symptoms and function. Subtractingthe pre-existing impairment from the current impairment yields the impairment because of the currentmental disorder of interest.ConclusionThe information provided in this article is preliminaryadvice for those who are asked to rate permanent consequences of COVID-19 illness in those administrativelyaccepted or adjudicated cases. With further clinical experience, the approach to rating may need to be modifiedslightly. However, the suggestions outlined should remainapplicable for most of the foreseeable future.6AMA Guides Newsletter Volume 25 Issue 4References1.Arons MM, Hatfield KM, Reddy SC, et al. PresymptomaticSARS-CoV-2 infections and transmission in a skilled nursingfacility. N Engl J Med. 2020;382:2081-2090. DOI: 10.1056/NEJMoa20084572.He X, Lau EH, Wu P, et al. Temporal dynamics in viral sheddingand transmissibility of COVID-19. Nat Med. sanova C, Celli BR, Barria P, et al. The 6-min walk distancein healthy subjects: reference standards from seven countries.Eur Respir J. 2011; 37: 150–156. doi:10.1183/09031936.00194909.4.Hegmann KT, Cowl CT, Harber P, Hyman MH, et al. Coronavirus(COVID-19) April 24, 2020 Update. 020/04/COVID-April-24-2020-public.pdf. Accessed July 6, 2020.5.Chen J, Wu J, Hao S, et al., Long term outcomes in survivors ofepidemic Influenza A (H7N9) virus infection. Scientific Reports.2017;7(1): 1-8.6.Chiumello, D., Cappola S, Froio S, et al. What’s next after ARDS:long-term outcomes. Respiratory Care. 2016;61(5): 689-699.7.Dinglas, VD, Chessare CM, Davis WE, et al. Perspectives ofsurvivors, families and researchers on key outcomes for researchin acute respiratory failure. Thorax. 2018;73(1): 7-12.8.DiSilvio, B, Young M, Gordon A et al, Complications andoutcomes of acute respiratory distress syndrome. Critical CareNursing Quarterly. 2019;42(4): 349-361.9.Herridge, MS, Moss M, Hough CL, et al, Recovery and outcomesafter the acute respiratory distress syndrome (ARDS) in patientsand their family caregivers. Intensive Care Med. 2016;42(5): 725738. doi: 10.1007/s00134-016-4321-8.10.Graham BL, Steenbruggen I, Miller MR, et al. Standardizationof Spirometry 2019 Update. An Official American ThoracicSociety and European Respiratory Society Technical Statement.Am J Resp Crit Care Med. 2019;200(8): e70-e88. doi:10.1164/rccm.201908-1590ST. 01908-1590ST11.DHHS (NIOSH) Publication No. 2012-116 January 2012.Spirometry Quality Assurance: Common Errors and Their Impacton Test Results. 116.pdf. Accessed July 6, 2020.12. Hyman MH, Harber P. Working with common pulmonaryproblems in AMA Guides to the Evaluation of Work Ability andReturn to Work, Second Edition. American Medical Association,2011.13. Rondinelli RD, ed. AMA Guides to the Evaluation of PermanentImpairment, 6th ed. Chicago: American Medical Association;2008: 87.14.Xu Z, Shi L, Zhang J, et al. Pathological findings of COVID-19associated acute respiratory distress syndrome. Lancet Respir Med.2020; 8: 420-422. ezzani A. Cardiopulmonary exercise testing: basics ofmethodology and measurements. Ann Am Thorac Soc. 2017; 14(Suppl 1): S3-S11.16.Bangalore S, Sharma A, Slotwiner A, et al. ST-segment elevationin patients with covid-19–a case series. N Engl J Med. 2020;382(25):2478-2480. doi:10.1056/NEJMc2009020.17.Inciardi RM, Lupi L, Zaccone G, et al. Cardiac involvement ina patient with Coronavirus Disease 2019 (COVID-19). JAMACardiol. doi:10.1001/jamacardio.2020.109. Accessed July 6, 2020.
Rating Survivors of COVID-19 for Permanent Impairment , continued18.Bowles, L, Platton S, Yartey N, et al. Lupus anticoagulant andabnormal coagulation tests in patients with covid-19. N Engl JMed. 2020; doi:10.1056/NEJMc2013656.19.Casey K, Iteen A, Nicolini R, et al. COVID-19 pneumonia withhemoptysis: acute segmental pulmonary emboli associated withnovel coronavirus infection. An J Emerg Med. 2020; doi: 10.1016/j.ajem.2020.04.011.20. Oxley TJ, Mocco J, Majidi S, et al. Large-vessel stroke as apresenting feature of Covid-19 in the Young. N Engl J Med.doi:10.1056/NEJMc2009787. Accessed July 6, 2020.21.Helms J, Kremer S, Merdji H, et al. Neurologic features in severeSARS-CoV-2 infection. N Engl J Med. 2020; 328(23):2268-2270.doi:10.1056/NEJMc2008597.22. Boesveldt S, Postma EM, Boak D, et al. Anosmia—a clinicalreview. Chemical Senses. 2017;42(7): 517.23. Toscano G, Palmerini F, Ravaglia S, et al. Guillain–Barrésyndrome associated with SARS-CoV-2. N Engl J Med. 2020;382(26);2574-2576. doi:10.1056/NEJMc2009191.24. Gutiérrez-Ortiz C, Méndez A, Rodrigo-Rey S, et al. Miller Fishersyndrome and polyneuritis cranialis in COVID-19. Neurology.2020; doi:10.1212/WNL.0000000000009619.25. Dimachkie MM, Barohn RJ. Guillain-Barré syndrome andvariants. Neurol Clin. 2013 May; 31(2): 491–510. doi: 10.1016/j.ncl.2013.01.005.26. Mao L, Jin H, Wang M, et al. Neurologic manifestations ofhospitalized patients with coronavirus disease 2019 in Wuhan,China. JAMA Neurol. 2020;77(6):683-690. doi:10.1001/jamaneurol.2020.1127.27.Koch S, Wollersheim T, Bierbrauer J, et al. Long-termrecovery in critical illness myopathy is complete, contrary topolyneuropathy. Muscle Nerve. 2014; 50(3): 431-436. doi:10.1002/mus.24175.29.Richardson S, Hirsch JS, Narasimhan M, et al. Presentingcharacteristics, comorbidities, and outcomes among 5700patients hospitalized with COVID-19 in the New York City area.JAMA. 2020;323(20):2052-2059. doi:10.1001/jama.2020.6775.30. Lai J, Ma S, Wang Y, et al. Factors associated with mental healthoutcomes among health care workers exposed to coronavirusdisease 2019. JAMA Netw Open. 2020;3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976.31.Walton M, Murray E, Christian MD. Mental healthcare for medical staff and affiliated healthcare workersduring the COVID-19 pandemic. Europ Heart J. 2020;doi:10.1177/2048872620922795.32. Burrer SL, et al. Characteristics of health care personnelwith COVID-19 — United States, February 12–April 9, 2020.Morb Mortal Wkly Rep. 2020 Apr 17; 69:477-481. https://doi.org/10.15585/mmwr.mm6915e6.33. Chow EJ, Schwartz NG, Tobolowsky FA. Symptom screening atillness onset of health care personnel with SARS-CoV-2 infectionin King County, Washington. JAMA. 2020 Apr 17; ing A, et al. Transmission of COVID-19 to health carepersonnel during exposures to a hospitalized patient — SolanoCounty, California, February 2020. Morb Mortal Wkly Rep. 2020Apr 17; 69:472-476. https://doi.org/10.15585/mmwr.mm6915e5.35. Charney ME, et al. Evidence based treatment of PTSD: anupdated review. Harvard Rev Psychiatry. 2018; 26 (3): 99-115.36.Giummarra MJ, et al. Early psychological interventions forposttraumatic stress, depression, and anxiety after traumaticinjury: a systematic review and meta-analysis. Clin Psychol Rev.2018; 62:11-36.37.Ostacher MJ, Cifu AS. Management of posttraumatic stressdisorder. JAMA. 2019; 321(2): 200-201.28. Lacomis D. Electrophysiology of neuromuscular disordersin critical illness. Muscle Nerve. 2013 Mar;47(3):452-463.doi:10.1002/mus.23615.Volume 25 Issue 3July/August 2020 AMA Guides Newsletter7
Medical Aspects of Causation for COVID-19James B. Talmage MD, Robert B. Snyder MDAMA Guides Newsletter. 2020; 25(4):0-00. tractThe decision about whether a case of documented COVID-19 illness is accepted as occupationally acquired and thus work compensable is made by insurers, or if contested, by judges or administrative bureaus. Ca
AMA Guides NEWSLETTER Updates, authoritative guidance, practical information, and rationales for proper use of AMA Guides July/August 2020 Volume 25 Issue 4