Transcription
UTI: An Opportunity for AntimicrobialStewardshipGhinwa Dumyati, MDProfessor of MedicineCenter for Community HealthUniversity of Rochester Medical CenterFebruary 8, 2017
Project to Implementing Antimicrobial Stewardship inNursing Homes-Funded by NYSDOHPrimary Objectives:1. Implement antimicrobial stewardship programs in LTCF2. Reduce the use of quinolones for the treatment of UTI andpneumonia3. Reduce the overall incidence of CDISecondary Objective:1. Monitor and report CDI through implementation and use ofNHSN
Project Implementation Recruited 7 LTCF: 4 large facilities 3 hospital affiliated facilities Implementation of the antimicrobial stewardship interventionoccurred successively at each of these LTCF Intervention was tailored to each LTCF context and needs
I. Stewardship TeamsHospital Team Hospital infectious diseasesphysician Hospital antimicrobial stewardshippharmacist Project coordinator Project infection preventionistLTCF Team Medical Director Nursing Director Infection Preventionist Nursing Educator In house dispensing Pharmacist NP/PA Director of Quality Nursing Home Administrator
Antimicrobial Stewardship CollaborationMicrobiology labMedical Director Advisory TeamDirectors of other NH in the communityHospital Team membersTreatment guidelines for UTI andPneumoniaLTCF TeamAntibiogram and list of urine culturesDispensing pharmacyIn-house and a large dispensing P CDI dataHospital TeamImplementation of guidelinesDiagnosis and Treatment guidelinesAntibiotic Reviews and feedbackData summariesUrine culture testing and treatment reviewEducation, pocket cards, postersCDI NHSN reportingAssistance with NHSN reporting
II. Measuring Antimicrobial Use
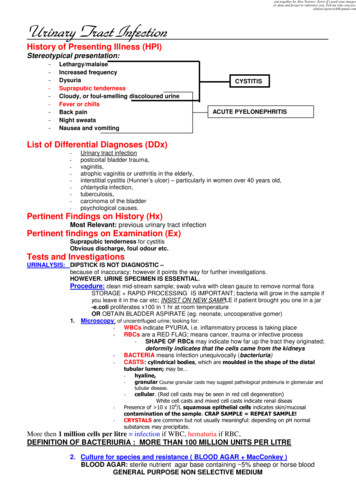
LTCF1-Top 12 Indications
LTCF1-12 Top Indications by Number of ResidentsUTI/PNEUMONIAPEMPHIGOIDOTHER GI INFECTIONUNSPECIFIED ABSCESSUTI PROPHYLAXISHEENT INFECTIONC. DIFFBRONCHITISDENTAL/SURGICAL PROPHYLAXISPNEUMONIASKIN/SOFT TISSUE INFECTIONUTI0204060Number of Residents80100120
Most Common Agents Used for UTI
UTI AntibiogramNursing home A- 2013Urine Isolates: % ulfamethoxazoleAztreonam50AmpicillinEscherichia coli 50# of isolatesAmpicillin-SulbactamOrganismGRAM-NEGATIVE ORGANISMS*Limitations prevent the testing and reporting of ampicillin-sulbactam and imipenem for P. mirabilis.&Differences in the % susceptibility for an organism represented by 30 isolates may not be statistically significant from year to year.
III. ActionImprove Antibiotic use for Urinary Tract InfectionsModified CDC assessment of appropriateness of antibiotics for UTI form: ion.html
Development of Minimum Criteria for Initiation ofAntibiotics-Loeb, 2001Guidance on when to start antibiotics for common infections
Revised Surveillance Definitions of Infections for NursingHomes Surveillance definitions are not the same as the clinical criteria to start treatment Surveillance definitions are a tool to assess the percentage of antibiotics used thatfit the criteria understand the gaps in knowledge, processes and guide improvement
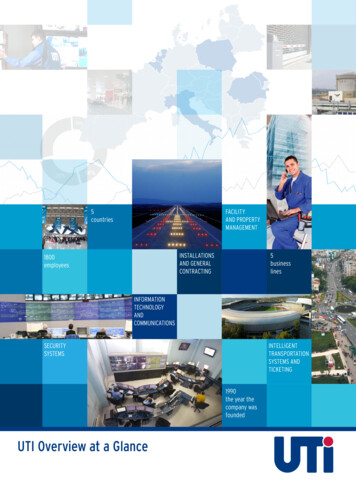
Appropriateness of UTI Testing and Treatment:Symptom Breakdown (n 42), Facility ANew onset quency4Other3Fever3Urgency3New Onset Retention2Incontinence & Bladder Spasm2Hematuria22Elevated WBCFlank Pain1None1Suprapubic Pain002468Number of Patients*12 patients, confusion delirium was the only symptom that triggered a urine culture10121416
Revised McGeer Criteria for UTI1. Need a positive urine cultureand2. Localizing signs and symptoms to the genitourinary tract
For Patients without an indwelling catheterSigns and symptomsAt least 1 of the following sign or symptomsubcriteria1. Acute dysuria or acute pain, swelling, ortenderness of the testes, epididymis, orprostate2. Fever or leukocytosis and at least 1 of thefollowing localizing urinary tract subcriteriaIf no fever: 2 of the localizing urinary tractsubcriteria1. Acute costovertebral angle pain ortenderness2. Suprapubic pain3. Gross hematuria4. New or marked increase in incontinence5. New or marked increase in urgency6. New or marked increase in frequencyUrine Culture1. At least 105 cfu/mL of no more than 2species of microorganisms in a voidedurine sample2. At least 102 cfu/mL of any number oforganisms in a specimen collected by inand-out catheter
For Patients with an Indwelling CatheterSigns and SymptomsAt least 1 of the following sign or symptomsubcriteria:1. Fever, rigors, or new-onset hypotension, withno alternate site of infection2. Either acute change in mental status oracute functional decline*, with no alternatediagnosis and leukocytosis3. New-onset suprapubic pain or costovertebralangle pain or tenderness4. Purulent discharge from around the catheteror acute pain, swelling, or tenderness of thetestes, epididymis, or prostate*The definition of acute functional decline is also based on changes in ADLs according to thescoring system in MDSCulture Urinary catheter specimen culture with atleast 105 cfu/mL of any organism(s)
Confusion Assessment Method (CAM) CriteriaAcute onsetEvidence of acute change in resident’s mental status from baselineFluctuatingBehavior fluctuating (eg, coming and going or changing in severityduring the assessment)InattentionResident has difficulty focusing attention (eg, unable to keep track ofdiscussion or easily distracted)Disorganized thinkingResident’s thinking is incoherent (eg, rambling conversation, unclearflow of ideas, unpredictable switches in subject)Altered level of consciousnessResident’s level of consciousness is described as different frombaseline (eg, hyperalert, sleepy, drowsy, difficult to arouse,nonresponsive)
A patient with advanced dementia may be unable to report urinary symptoms, in thissituation, it is reasonable to obtain a urine culture if there are signs of systemic infectionsuch as Fever, (increase in temperature 2o F(1.1o C) from baseline) Elevated WBC Chillsin the absence of additional symptoms (e.g. new cough) to suggest an alternative source ofinfection
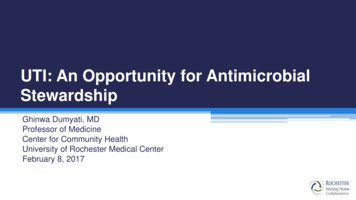
Revised McGeer Surveillance Criteria*Did not meet criteriaDBA0102030405060Percentage708090100*Stone ND et. al. Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria. Infection control andhospital epidemiology:2012;33(10):965-977
Findings of Medical Record ReviewMost of the residents are tested and treated for asymptomatic bacteriuriaTreatment 47% were treated empirically 30% organisms non susceptible 53% were treated after culture results Evaluation and follow up at 48-72 hours minimal A positive culture drives the decision to treatDuration of treatment Mean 5 days (range 3-14 days)
Asymptomatic BacteriuriaIf you obtain a urine specimen from all female residents in your nursing home,how many would be positive?a. 10%b. 80%c. Up to 50% Elderly LTCF Women 25-50% Elderly LTCF Men 15-40% Short term catheterization 9-23% Long term catheterization 100%
A Positive Urine Test, What Does it Mean?Bacteria in UrineUrinary Tract SymptomsNoAsymptomaticBacteriuria(ASB)YesUrinary Tract Infection(UTI)
Asymptomatic Bacteriuria Is CommonAsymptomatic bacteriuriaWomen less than 60 years3-5%Elderly in lderly in Nursing HomesPatient with indwelling catheter100%Nicolle LE, Clinical Infectious Diseases 2005;40(5): 643–54
IV. Education- Medical ProvidersSmall group sessions Presentation of facility antibiotic use, CDI andUTI review data Review appropriate testing and treatment of UTI Review antibiogram Review locally created treatment guidelines Provided pocket treatment cards Recommended Improvement of the documentation of signs andsymptoms Clinical evaluation for every antibiotic prescriptionand at 48 hours, i.e. antibiotic “time out”
Education- Nursing StaffSmall group sessions Review CDI and UTI review data Review appropriateness of urine testingand treatment Recommended the use of an on-lineeducation program Recommended the use of the SBAR Emphasized the importance ofdocumentation of signs and symptoms Created posters
Education- Family Created a brochure on appropriatetreatment of UTI Created a newsletter fordistribution to residents andfamilies Recommended coaching of nursingstaff on best method to deliver thebrochure information to families
V. Feedback of Data
LTCF1. Rate of Antibiotic Starts for UTI and Urine Culture Rate
LTCF1. Change in Ciprofloxacin DOT for UTI
Example How Data Was Used for Action Goal to capture all urine cultures and UTItreatment Worked with micro lab to get list of testedresidents Worked with pharmacy to get new antibiotic startsfor UTI Uncovered the limitation of the 24 hour report Performed monthly assessments of tested andtreated residents for signs and symptoms of UTI Feedback to nurses and in house medicalproviders on the appropriateness of testing andtreatment“We used towork in silos,now we talkto each other”
Action: Improve Documentation of AntibioticIndicationI make sure all theantibiotic ordershave an indication
Dispensing Pharmacist Antibiotic Review and FeedbackSuggestions:Thank You,Signature of PharmacistPlease contact me in the Pharmacy (ext 6108) if additional information is required on the matter.RESPONSE:The above comments or suggestions were reviewed by me and my response is:Agree and have taken follow-up action.Don’t AgreeWill Review and Respond.See following comments:Signature of Physician/NP/PAPLEASE RETURN TO THE PHARMACY WHEN COMPLETED
Acknowledgments Elizabeth Dodds Ashley, PharmD Christina Felsen, MPH Gail Quinlan, RN, CIC Grant Barney All the LTCF Medical Directors,Medical and Nursing staff LTCF Pharmacists Vince Galetta, Buffalo Pharmacies
Nursing Documentation
Urinary Tract Infection (UTI) Urinary Tract Symptoms No Yes. Asymptomatic Bacteriuria Is Common Nicolle LE, Clinical Infectious Diseases 2005;40(5): 643-54 . education program Recommended the use of the SBAR Emphasized the importance of documentation of signs and symptoms Created posters .