Transcription
Career Development Pathways inImplementation ScienceElizabeth M. Yano, PhD, MSPHSteven Asch, MD, MPHAlison B. Hamilton, PhD, MPHVA HSR&D Career Development Award Enhancement Initiative1October 10th, 2017
Background Implementing research evidence into routinepractice and policy requires:– Diverse skills, training and experience Most academic programs do not coverrequisite didactic or experiential needs– Training opportunities in implementation sciencemethods remains limited– Need theoretical frameworks, measurement, trialdesigns, multilevel stakeholder engagement2
Purpose of Session Explore career development pathways ofimplementation experts– Examples from an epidemiologist, generalinternist, and anthropologist Elucidate commonalities across differentapproaches to developing careers in the field3
Polling Question #1 What is your primary role in VA?– Student, trainee, or fellow– Clinician– Researcher– Administrator, manager, or policymaker– Other4
Polling Question #2 What best describes your implementationscience experience to date?– Have not done implementation research– Have collaborated on implementation research– Have conducted implementation research myself– Have applied for implementation research funding– Have led a funded implementation research grant5
So let’s get started Elizabeth (Becky) Yano, PhD, MSPH– Epidemiology, health services research,program evaluation, organizations Steven Asch, MD, MPH– General internal medicine, ClinicalScholar, epidemiology, palliative care,quality improvement Alison Hamilton, PhD, MPH– Medical anthropology, communityhealth sciences, vulnerable populations6
Pathway #1 (Yano) Started off in program evaluation– Required anchoring in the “client” (funder andprogram being evaluated)– Evaluations outside VA working with foundations,community-based organizations, county staff – VA entré through evaluation of the early VA PilotAmbulatory Care & Education (PACE) Program Regional demonstration project to test academic globalcare teams, ambulatory care education, early EMR, etc. Multiple stakeholders (including academic affiliates)7
Building Blocks Pre-doctoral fellowship RAND Health Policy– Medical Outcomes Study, Six Hospital Study onvariations in processes and outcomes of care, etc. UCLA PhD in Epidemiology but – Was working fulltime in evaluation/HSR– Integrated HSR/health policy into epidemiology toget to how health systems influence pop health Experiential work created breadth/depth inabsence of didactic/fellowship opportunities8
Mentorship & Experiential Work Worked with Lisa Rubenstein, MD, MSPH– Pre-QUERI implementation vision with QI anchor– Depression collaborative care (TIDES/WAVEs)– To QUITS (Sherman/Yano) and EQUIP (Young)– Development of evidence-based QI (EBQI) tenetsSupportive mentorship, hands-on engagement,experiential immersion, methods development,leadership opportunities in context of studies,expansion of teams (Seattle, Little Rock, Durham)9
10
Embrace team science, uncertaintyand varying to no control Team science aspects very important– Implementation science requires unusual degree ofcollaboration, partnership and trust building– Data sharing, multilevel stakeholder engagement,multidisciplinary, translation of data/findings intolanguage useable by non-scientists (incl patients)– Understanding contextual factors (try walking in“another’s shoes”) and adaptations needed Comfort w/uncertainty, nimbleness to adapt,recognize you have no authority in this space11
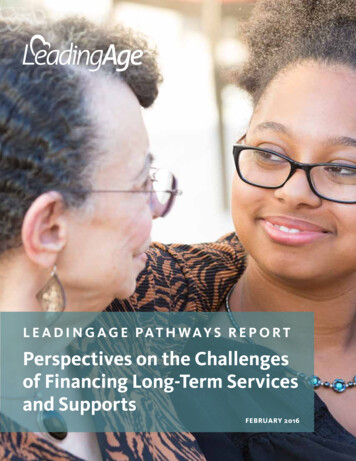
Building and Leveraging1st orgsurveyEarly investment inpartner-oriented work2001 vs 2007Organization of women’s primary careWHOrg ofCareEvaluation/organization of primary carePACEEvaluation2nd orgsurveyVA FirmSystemsAnalysisPerformance ofVA PC DeliveryModels1st org survey2nd org surveyImpact ofPract Struxon QCOrg Variationsin CRCScreen’g RatesQUITSEvaluationChanges inWH CareVA QualityTransformationTIDES & WAVES &COVES, ReTIDESEvaluationsPC practice change, org influences on implem operationsfunded HSR&D orQUERI funded12
Building and LeveragingChanges inWH CareWHResearchAgendaWHResearchNetworkWomen’sMH CareModelsGenderSensitiveMH CareImplem &Impact of VAPCMHTIDES & WAVES &COVES & ReTIDESEvaluationsVAIL(VISN22 PACTDemo Lab)CREATE combined threadsAccelerate Implementation ofComprehensive WH CareImpact ofComprehensiveWomen’s Health CareImplementation ofWomen’s Health PACT 3 other CREATE studies operationsfunded HSR&D orQUERI funded13
Filling the gaps Develop new collaborations and mentors– Reach out for study design expertise as needed– Engage expert consultants where possible Look beyond the usual suspects, many of whom arenow oversubscribed AcademyHealth Dissemination & Implementationattendees, workshops, professional networks VA Implementation Research Group (and work groups)– Virtual collaboration a norm rather than exception14
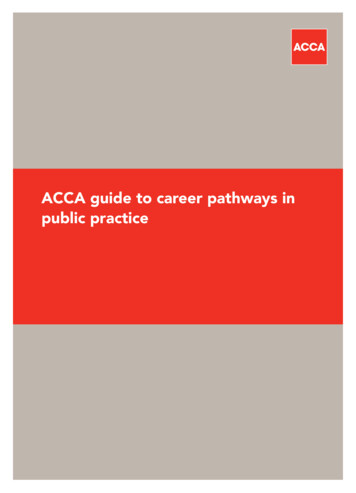
Pathway #2 (Asch)HighlightingPoor AccessShouldMotivatePolicy
MeasuringQuality ShouldSpur BetterQuality in US
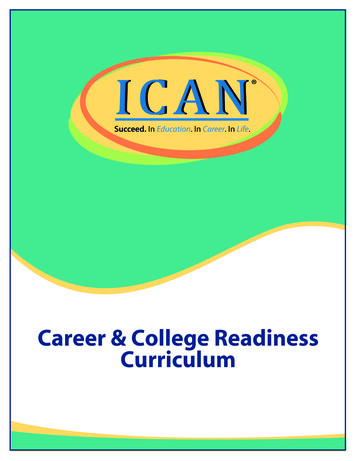
Adjusted Overall Quality by Income(52-54)(54-56)(56-58)17
Adjusted Overall Quality by Income(56-58)(54-56)(52-54)18
World’s Response: “Interesting”But Not Much Changed Disparities between groups pale beforedisparities between current and desiredperformance Right wing think tanks used data to justifyrestricting public insurance subsidies to poor Subsequent longitudinal studies have shown fewtrends toward better quality nationally19
20
The ultimate goal ofD&I scienceis to ensure thatadvances in healthscience becomestandards for carein all populationsand all healthcaresettings.(Glasgow, AJPH, 2012)21
TheYinandYangofQualityImprovementandResearch22
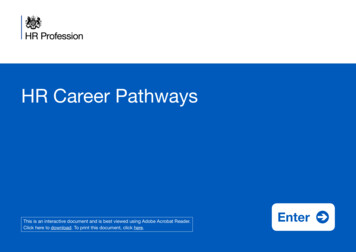
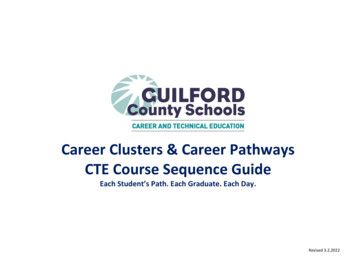
QUERI-HIV/Hepatitis - VHA COLLABORATIONSOffice of Patient CareServicesMulti-VISN QILeadershipPublic Health StrategicHealthcare GroupMulti-VISN QI, Rapid Test,Rapid Test in ER, Homeless Test (J. Burgess;R. Valdiserri; D. Ross; J. Halloran)Casefinding (L. Mole & L. Backus)Multi-VISN QI (VISN 1,3,16,22 Directors and CMOs)Rapid Test (VISN 22; K. Clark, Director; T.Osborn, QMO)HITIDES (VISN 16 Director)Multi-VISN QI (M. Agarwal)HITIDES(M. Shelhorse)QUERI CentersEducationCommitteesHITIDES (MH, SUD)RT SUD (H. Hagedorn; H. Anaya; R. Henry)QUERI Resource Center (S. Asch)VISN QI(VISN 22, CPC)Multi-VISN QI(All VISN 22 sites: Primary Care, ITS, HIV managers)HITIDES (Little Rock,Houston, Atlanta HIV clinics)Rapid Test, Rapid Test in ER(VA GLAHS primary care group)ClinicalManagement &Provider GroupsMulti-VISN QI(IT managers at all VISN 3 and VISN 16 sites)Center for Health Quality, Outcomes and Economic ResearchCenter for the Study of Healthcare Provider BehaviorPatient Centered HCVVACSACTION NetworkCenters ofExcellenceOffice of Information andTechnology,Facility- based IRMSOther HIV and HCVStudy Groups23
Dances I have attended withmentees Participants wanted to refer patients rather thanrandomize: VA multimorbid management trial (Zulman) VA Lean program leadership changed national rolloutstrategy during evaluation (Vashi) Cancer center shifted intervention from nurse coordinatorsto patient navigators (Winget) Good dangers adjust to our partners’ moves, and learn.24
Lessons from Dancing with theDevil You Know Shift research topics to where you can make the mostdifference Building research enterprise for partner eased byrelationship planning, programmatic funding Partnership improves research and makes “dead mouseresearch” less likely Researchers can serve two masters – truth and relevance25
“To that person who devoteshis life to science, nothing cangive more happiness thanincreasing the number ofdiscoveries.But his cup of joy is full whenthe results of his studiesimmediately find practicalapplications.”—Louis Pasteur26
Pathway #3 (Hamilton) Started off as the “qualitative person”– Background in medical and psychologicalanthropology– What was in my toolkit? Strengths in interviewing,analysis, theory27
Building Blocks Before “implementation science” (late ’90s, early2000s)– CSAT Methamphetamine Treatment Project:implementing evidence-based intervention incommunity-based treatment organizations– VA opportunity with Alex Young and Amy Cohen:EQUIP-1 NIDA K01 (Career Development Award), 2006-2011– MPH in Community Health Sciences as trainingcomponent28
Building Blocks (cont.) Professional growth growth of implementationscience as a field (mid-2000s)– VA QUERI-funded Center for ImplementationPractice & Research Support (CIPRS) w/ BrianMittman: provided trainings– EQUIP-2: one of the first “hybrid type 2” studies– Expansion of implementation researchopportunities29
Being Trained and Training Others Implementation Research Institute, 2010-2012(and beyond)– Rigorous training with outstanding internationalfaculty– Expanded network of mentors and colleagues– Fostered opportunities for collaboration to presentday Implementation science workshops,presentations, courses– Focus on qualitative and mixed methods30
Nothing Like Hands-On Training Having a defined skill set opens doors across a variety ofstudies/topics/funding sources– Consumer providers in mental health (Chinman)– Genomics (Scheuner)– Hep-C & depression treatment (Kanwal)– Patient-centered medical home (Rubenstein/Yano)– Women Veterans’ comprehensive care (Yano)– Homelessness (Washington)– HIV services (Wyatt)– Children’s mental health services (Lau & Brookman-Frazee)31
Put Yourself Out ThereLet people know what you have to offer (yourskill set), what you’re thinking about: In writing At conferences On national calls In planning meetings At trainings32
CollaborationsOpportunities Implementation science is a team sport– A productive co-investigator role can launch acareer pathway Branch out: identify people who study a topicof interest, or use a method or design ofinterest– Ex. of guideline implementation– Review manuscripts for implementation sciencejournals (many are open access)– The field is friendly and interested in new ideas33
Polling Question #3 What would be most valuable for your careerdevelopment in implementation science?– Hands-on experience doing implementationresearch– Training/coursework– Grant-writing support– Funding opportunities– Mentorship34
Polling Question #4 What kinds of implementation sciencemethods do you need training/experience in?– How to apply theoretical frameworks– Implementation strategies– Implementation study designs (e.g., steppedwedge)– Mixed methods implementation evaluation– Measures of spread and/or sustainability35
Training Opportunities pportunities/ NIH/VA Implementation Research Institute: http://iristl.org/ Training Institute for Dissemination and Implementation Research in Health(TIDIRH) Columbia University: implementation-science University of Wisconsin Dissemination & Implementation Short Coursehttps://ictr.wisc.edu/dni-short-course-2017/ UCSF: elerate.ucsf.edu/training/ids#whatis Archived Enhancing Implementation Science (EIS) and other HSR&Dcyberseminars: logarchive.cfm36
Conferences NIH Conference on the Science of Dissemination -and-implementationhealth Society for Implementation Research archcollaboration.org/ Global Implementation out/ Nordic Implementation dicimplementation-conference37
Resources Dissemination & implementation models: D&I Resources list: tion-implementation/Global Implementation Initiative (resources): ment Science Research Network: http://isrn.net/University of Colorado, niversity of Washington: lementationscienceHarvard: lementation-scienceNHLBI: https://www.nhlbi.nih.gov/about/org/ctris/NCI: s-and-directionsCommunity Tool Box: http://ctb.ku.edu/en/toolkitsKT: https://knowledgetranslation.net/implementation38
Thank you!Becky Yano: elizabeth.yano@va.govSteve Asch: steven.asch@va.govAlison Hamilton: alison.hamilton@va.gov39
Pre-doctoral fellowship RAND Health Policy - Medical Outcomes Study, Six Hospital Study on variations in processes and outcomes of care, etc. UCLA PhD in Epidemiology but - Was working fulltime in evaluation/HSR - Integrated HSR/health policy into epidemiology to get to how health systems influence pop health