Transcription
Pre-eclampsiaEtiology and Clinical PracticePre-eclampsia is one of the leading causes ofdeath and disability in mothers and babies. Overfour million women worldwide will develop thedisorder every year. This book, written by aninternational team of experts, focuses on both thescientific basis of pre-eclampsia and its management. The basic science section contains up-todate reviews of the most exciting research developments in pre-eclampsia. The clinical chaptersprovide a comprehensive review of the pertinentliterature, highlighting recent data and new ideasor developments in current management. There isa section in each chapter (where relevant) thatdeals with practical management, giving cliniciansa formulated treatment plan that they can implement directly. The book will be of interest to allprofessionals interested in the reproductivesciences, and to obstetricians and physicians withan interest in pre-eclampsia.Fioan Lyall is Professor of Maternal and FetalHealth at the University of Glasgow. She is ChiefEditor of the journal Hypertension in Pregnancy.Michael Belfort is Professor of Obstetrics andGynecology at the University of Utah. He isalso Director of Perinatal Research and Co-directorof Fetal Surgery at the Hospital Corporationof America in Nashville.
Pre-eclampsiaEtiology and Clinical PracticeFiona LyallUniversity of GlasgowMichael BelfortUniversity of Utah
CAMBRIDGE UNIVERSITY PRESSCambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São PauloCambridge University PressThe Edinburgh Building, Cambridge CB2 8RU, UKPublished in the United States of America by Cambridge University Press, New Yorkwww.cambridge.orgInformation on this title: www.cambridge.org/9780521831895 Cambridge University Press 2007This publication is in copyright. Subject to statutory exception and to the provision ofrelevant collective licensing agreements, no reproduction of any part may take placewithout the written permission of Cambridge University Press.First published in print format 2007eBook (NetLibrary)ISBN-13 978-0-511-29022-0ISBN-10 0-511-29022-5eBook 5hardback0-521-83189-XCambridge University Press has no responsibility for the persistence or accuracy of urlsfor external or third-party internet websites referred to in this publication, and does notguarantee that any content on such websites is, or will remain, accurate or appropriate.Every effort has been made in preparing this book to provide accurate and up-to-dateinformation that is in accord with accepted standards and practice at the time ofpublication. Nevertheless, the authors, editors and publishers can make no warranties thatthe information contained herein is totally free from error, not least because clinicalstandards are constantly changing through research and regulation. The authors, editorsand publishers therefore disclaim all liability for direct or consequential damages resultingfrom the use of material contained in this book. Readers are strongly advised to pay carefulattention to information provided by the manufacturer of any drugs or equipment thatthey plan to use.
For my mother,Patricia Stratton Wilson Belfort,1932 2006MBFor my mother, Margaret Stewart MalcolmStruthers Lyall (1935 1997) and my father,Alexander George Lyall.FL
ContentsList of contributorsPrefacepage xixviiPart I Basic Science1Trophoblast invasion in pre-eclampsiaand other pregnancy disorders13Robert Pijnenborg, Lisbeth Vercruysse,Myriam Hanssens and F. André Van Assche2Development of the utero-placentalcirculation: purported mechanisms forcytotrophoblast invasion in normalpregnancy and pre-eclampsia20Fiona Lyall3In vitro models for studyingpre-eclampsia37John D. Aplin and Ian P. Crocker4Endothelial factors50Muna Noori, Mina Savvidou and David Williams5The renin angiotensin system inpre-eclampsia78Fiona Broughton Pipkin6Immunological factors and placentation:implications for pre-eclampsia92Ashley Moffett and Susan E. Hiby7Immunological factors and placentation:implications for pre-eclampsia103C. W. G. Redman and I. L. Sargentvii
viiiContents8The role of oxidative stress inpre-eclampsia19121M. T. M. Raijmakers and L. Poston910Placental hypoxia, hyperoxia andischemia reperfusion injury inpre-eclampsiaImmune maladaptation in the etiologyof pre-eclampsia; an updatedepidemiological perspectiveGus Dekker and Pierre Yves RobillardGraham J. Burton, Tai-Ho Hung andGenetics of pre-eclampsia andcounseling the patient whodeveloped pre-eclampsiaEric JauniauxKenneth WardTenney Parker changes and apoptoticversus necrotic shedding oftrophoblast in normal pregnancy andpre-eclampsia2762013821Thrombophilias and pre-eclampsia295305Isobel D. Walker15222Peter Kaufmann and Berthold HuppertzMedical illness and the risk ofpre-eclampsia325Catherine Nelson-Piercy11Dyslipidemia and pre-eclampsia16423Carl A. Hubel12Pre-eclampsia a two-stage disorder:what is the linkage? Are there directedfetal/placental signals?24High altitude and pre-eclampsia25195Stacy Zamudio14The use of mouse models to explorefetal maternal interactions underlyingpre-eclampsiaPrediction of pre-eclampsiaLong-term implications ofpre-eclampsia for maternal health20917Classification and diagnosis ofpre-eclampsia2721528Measuring blood pressure in pregnancyand pre-eclampsiaAndrew H. Shennan and Annemarie De Greeff369The differential diagnosis ofpre-eclampsia and eclampsia380Complications of pre-eclampsia406Central nervous system findings inpre-eclampsia and eclampsia424Diane Twickler and F. Gary Cunningham23229Pathogenesis and treatment ofeclampsia437Joong Shin Park, Michael A. Belfort and241Errol R. Norwitz30243Anesthesia for the pre-eclampticpatient451Jose M. Rivers and Maya S. SureshRobyn A. North18Management of severe pre-eclampsiaGary A. Dildy III and Michael A. BelfortGordon C. S. SmithPart II Clinical Practice357Michael VarnerLeslie Myatt and Lavenia B. Carpenter16Management of mild pre-eclampsiaKristin H. Coppage and Baha M. Sibai26James C. Cross15339Tracey Glanville and James J. Walker183Jim Roberts13The kidney and pre-eclampsiaM. C. Smith and J. M. Davison31258Critical care management of severepre-eclampsiaJohn Anthony476
Contents32The role of maternal and fetal Dopplerin pre-eclampsia34489J. Hornbuckle and S. Robson33Pregnancy-induced hypertension the effects on the newbornJonathan CouttsMedico-legal implications of thediagnosis of pre-eclampsia522Jeffrey P. Phelan506Subject Index535ix
ContributorsJohn AnthonyUniversity of Cape TownDepartment of MedicineDivision of HypertensionCape Town, ZA-7925South AfricaJohn AplinDivision of Human DevelopmentFaculty of MedicineUniversity of ManchesterSt Mary’s HospitalManchester M13 0JHUKMichael BelfortDepartment of Obstetrics and GynecologyUniversity of Utah Health Sciences CenterSalt Lake City, UtahUSAFiona Broughton PipkinAcademic Division of Obstetrics & GynecologyMaternity Unit, City HospitalNottingham NG5 1PBUKGraham BurtonDepartment of AnatomyUniversity of CambridgeDowning StreetCambridge CB2 3DYUKxi
xiiContributorsLavenia CarpenterJ. M. DavisonDepartment of Obstetrics and GynecologyObstetrics & GynaecologyUniversity of Cincinnati College of Medicine4th Floor, Leazes WingP.O. Box 670526231 Albert Sabin WayRoyal Victoria InfirmaryNewcastle upon Tyne NE1 4LPCincinnati, OH 45267USAGus DekkerWomen’s and Children’s DivisionKristin CoppageLyell McEwin Health ServiceDepartment of Obstetrics and GynecologyNorthern Campus University of AdelaideUniversity of CincinnatiHaydown Road231 Albert Sabin WayM/L 0526Elizabeth Vale, SA 5112AustraliaCincinnati, OH 45267-0526USAGary DildyDepartment of Obstetrics and GynecologyJonathan CouttsLouisiana State University School of MedicineThe Queen Mother’s Hospital1542 Tulane AvenueYorkhillNew Orleans, LA 70112Glasgow G3 8SJ, UKUSAIan CrockerTracey GlanvilleDivision of Human DevelopmentLeeds Teaching Hospital TrustFaculty of MedicineSt James University HospitalUniversity of ManchesterBeckett StreetSt Mary’s HospitalLeeds LS9 7TFManchester M13 0JHUKUKMyriam HanssensJames CrossDepartment of Obstetrics and GynaecologyGenes and Development Research GroupUniversity Hospital GasthuisbergDepartment of Biochemistry and Molecular BiologyHerestraat 49Faculty of MedicineB3000 Leuven, BelgiumUniversity of CalgaryHSC Room 2279Susan Hiby3330 Hospital Drive NWCalgary, Alberta T2N 4N1Department of PathologyTennis Court RoadCanadaUniversity of CambridgeCambridge CB2 1QPF. Gary CunninghamUKDepartment of Obstetrics and GynecologyUT Southwestern Medical CenterJ. Hornbuckle5323 Harry Hines Blvd.Centre for Reproduction, Growth and DevelopmentDallas, TX 75390USAUniversity of LeedsUK
ContributorsCarl HubelLeslie MyattMagee-Womens’ Research InstituteDepartment of Obstetrics and Gynecology204 Craft AvenueUniversity of Cincinnati College of MedicinePittsburgh, PA 15213USAP.O. Box 670526231 Albert Sabin WayCincinnati, OH 45267Tai-Ho HungUSADepartment of AnatomyDowning StreetCatherine Nelson-PiercyCambridge CB2 3DY, UK10th floor, Directorate OfficeNorth WingBerthold HuppertzGuy’s and St. Thomas’ NHS FoundationInstitute of Cell Biology, Histology and Embryology,Medical University of Graz,Lambeth Palace RoadLondon SE1 8EHHarrachgasse 21/7UK8010 GrazAustriaEric JauniauxAcademic Department of Obstetrics and GynaecologyUniversity College London89 96 Chenies MewsLondon WC1E 6HX, UKPeter KaufmannDepartment of AnatomyUniversity Hospital RWTH AachenWendlingweg 2D-52057 AachenGermanyMuna NooriDivision of SORAImperial College LondonChelsea and Westminster Hospital309 Fulham RoadLondon SWIO 9WHUKRobyn NorthDepartment of Obstetrics and GynaecologyUniversity of AucklandPrivate Bag 92019New ZealandFiona LyallErrol NorwitzMaternal and Fetal Medicine SectionYale University School of MedicineDepartment of Obstetrics, Gynecology andInstitute of Medical GeneticsUniversity of GlasgowYorkhillGlasgow G3 8SJUKReproductive SciencesYale-New Haven Hospital333 Cedar StreetNew Haven, CT 06520-8063USAAshley MoffettDepartment of PathologyJoong Shin ParkTennis Court RoadDepartment of Obstetrics and GynecologySeoul National University College of MedicineUniversity of CambridgeCambridge CB2 1QPUKSeoul 110-744Koreaxiii
xivContributorsJeffrey PhelanJim Roberts959 East Walnut StreetMagee-Womens’ Research InstituteSuite 200204 Craft AvenuePasadena, CA 91106USAPittsburgh, PA 15213USARobert PijnenborgDepartment of Obstetrics and GynaecologyPierre Yves RobillardUniversity Hospital GasthuisbergNeonatologyHerestraat 49Center Hospitalier Sud-ReunionB3000 Leuven, BelgiumBP 350 97488Saint-Pierre cedexLucilla PostonMaternal and Fetal Research UnitReunionFranceDepartment of Women’s HealthSt Thomas’ HospitalLambeth Palace RdLondon SE1 7EHUKMaarten T. M. RaijmakersMáxima Medisch CentrumDepartment of Clinical ChemistryPO Box 77775500 MB VeldhovenThe NetherlandsChris W. G. RedmanStephen RobsonSurgical and Reproductive Sciences3rd Floor Leech BuildingMedical SchoolNewcastle upon Tyne NE2 4HHUKIan L. SargentNuffield Department of Obstetrics and GynaecologyJohn Radcliffe HospitalOxford OX3 9DUUKNuffield Department of Obstetrics and GynaecologyJohn Radcliffe HospitalOxford OX3 9DUUKMina SavvidouHarris Birthright Research Centre for Fetal MedicineKings College HospitalAnnemarie ReindersNieuweweg 47Denmark HillLondon SE9 5RS7241 ES LOCHEMUKThe NetherlandsJose RiversAndrew ShennanDepartment of AnesthesiologyMaternal and Fetal Research UnitSuite 1003Department of Women’s Health6550 Fannin StreetHouston, TX 77030St Thomas’ HospitalLondon SE1 7EHUSAUK
ContributorsBaha SibaiLisbeth VercruysseDepartment of Obstetrics & GynecologyDepartment of Obestetrics and GynaecologyUniversity of Cincinnati,University Hospital GasthuisbergCincinnati, OH 45221USAHerestraat 49B3000 Leuven, BelgiumGordon SmithDepartment of Obstetrics and GynaecologyCambridge UniversityIsobel WalkerRosie Maternity HospitalDepartment of HaematologyCambridge CB2 2SWGlasgow Royal InfirmaryUKGlasgow G4 0SFMarie SmithUKObstetrics & GynaecologyJames Walker4th Floor, Leazes WingLeeds Teaching Hospital TrustRoyal Victoria InfirmarySt James University HospitalNewcastle upon Tyne NE1 4LPBeckett StreetUKLeeds LS9 7TFMaya SureshUKDepartment of AnesthesiologySuite 1003Kenneth Ward6550 Fannin StreetHouston, TX 77030Department of Obstetrics and GynecologyUSA1319 Punahou Street, Room 824Honolulu, HI 96826, USADiane TwicklerKapiolani HospitalUniversity of TexasSouthWestern Medical CenterDepartment of Radiology5323 Harry Hines BlvdDallas, TX 75390USAF. André Van AsscheDepartment of Obstetrics and GynaecologyDavid WilliamsInstitute for Women’s HealthUniversity College LondonElizabeth Garrett Anderson HospitalHuntley StreetLondon WC1E 6DHUKUniversity Hospital GasthuisbergHerestraat 49B3000 Leuven, BelgiumStacy ZamudioUMD-New Jersey Medical SchoolMichael VarnerDepartment of Obstetrics, Gynecology andUniversity of Utah School of MedicineWomen’s Health185 South Orange Ave MSB -50550 North Medical Drive,Salt Lake City, UT 84132USANewark, NJ 07103-2714USAxv
PrefacePre-eclampsia complicates 2 3% of primigravidpregnancies and 5 7% of nulliparous women. It isone of the leading causes of death and disability ofmothers and babies. Over four million women willdevelop the disorder worldwide every year. Thisbook, written by scientists and clinicians whoare internationally recognized as experts in theirrespective fields, focuses on both the scientificbasis of pre-eclampsia along with management.The basic science section contains up-to-datereviews and theories focused on the most excitingresearch developments in pre-eclampsia. Theclinical chapters provide a comprehensive reviewof the pertinent literature highlighting recent dataand work that suggest new ideas or changesin current management. There is a section ineach chapter (when appropriate) that deals withmanagement on a practical level so that theclinician (residents/registrars/consultants) will beable to take away a formulated treatment plan thatthey can implement directly.The book will be of interest to scientists andstudents interested in reproductive sciences as wellas medical students, obstetricians and physicianswith an interest in pre-eclampsia.xvii
PART IBasic Science
1Trophoblast invasion in pre-eclampsia andother pregnancy disordersRobert Pijnenborg, Lisbeth Vercruysse, Myriam Hanssens and F. André Van AsscheTrophoblast invasion is a major feature of hemochorial placentation, notably in the human wherethis invasion is exceptionally deep comparedwith the few other primate species studiedso far (Ramsey et al., 1976). It is assumed thatpre-eclampsia/eclampsia, which occurs almostexclusively in the human species, is in someway associated with problems related to thisdeep invasion. So far, only a few case reportshave been published suggesting a similarcomplication in pregnant gorillas (Baird, 1981;Thornton and Onwude, 1992). Unfortunately nothing is known about trophoblast invasion in thisspecies.It is now common knowledge that duringpregnancy extensive vascular alterations takeplace in the spiral arteries which supply maternalblood to the placenta. In this chapter we will firstsketch briefly the historical context of the discoveryof structural changes in placental bed spiralarteries and the role of invading extravilloustrophoblast. The importance of this ‘‘physiologicalchange’’ of spiral arteries is highlighted by itsrestricted occurrence in pre-eclampsia, and therefore we will discuss next the evidence for impairedtrophoblast invasion preceding the onset of clinicalsymptoms of pre-eclampsia. In the third part thestructural features of invaded and non-invadedspiral arteries will be described in some detail, andfinally we will evaluate the occurrence of physiological changes and vascular lesions in otherdisorders of pregnancy.Impaired physiological changein spiral arteriesAlthough pre-eclampsia/eclampsia has beenrecognized for a long time in history as animportant pregnancy complication (Lindheimeret al., 1999), a possible histopathological basisfor this condition was only identified in thelate 1960s. The idea that maternal perfusion ofthe placenta is disturbed in pre-eclampsia is anold one, and was based on the regular occurrenceof placental infarcts in such cases (reviewed byRobertson et al., 1967). Searching for associatedvascular pathologies, atherosclerosis-like lesionswere described in spiral arteries of decidualfragments attached to delivered placentae,and the term ‘‘acute atherosis’’ was introducedfor the characteristic lesion of fibrinoid necrosisand accumulated foam cells (Hertig, 1945; Zeekand Assali, 1950). Following the suggestion that areduced uterine blood flow in primigravidaepredisposes to pre-eclampsia, attempts weremade to measure maternal placental flow innormal and pre-eclamptic pregnancies, using avariety of techniques (reviewed by MacGillivray,1983). Of all the early placental flow studies, thehighest impact was made by the demonstration ofBrowne and Veall (1953) of reduced maternal bloodflow in the placenta of hypertensive pregnancies.This paper provided the primary inspirationfor histological work on the placental bed inthe hope of identifying a pathogenic basis for3
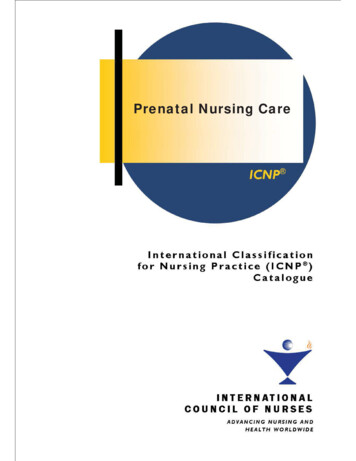
4R. Pijnenborg, L. Vercruysse, M. Hanssens and F. A. Van Asschethe disturbed flow. It was felt that restrictingoneself to vascular structures within decidualfragments attached to delivered placentas was notappropriate and therefore, for the first time,placental bed biopsies including myometriumand decidua were collected during Cesareansection (Dixon and Robertson, 1958). While lookingfor atherosclerotic lesions in these biopsies,however, other vascular alterations were discovered, and this was totally unexpected.During the initial studies of placental bedbiopsies it soon became obvious that in uncomplicated pregnancies normal arteries were virtuallyabsent from both decidua and myometrium.Instead, unusual structures were observed ofapparently vascular origin, which could be identified as spiral arteries only by tracing them to theirorigin from the radial arteries deep in the myometrium (Brosens et al., 1967). In specimens fromnormal pregnancies these vascular alterations,referred to as ‘‘physiological changes’’ to indicatethat they are not pathological, consisted of thereplacement of the smooth muscle wall by afibrinoid matrix material with embedded cells(Figure 1.1a). Although the nature of the embeddedcells was unknown at that time, it was postulatedthat they were derived from invasive trophoblast.Surprisingly, however, in specimens obtained frompre-eclamptic pregnancies recognizable arterialstructures could be found readily in the innermyometrium, and it was speculated that in suchcases the restricted occurrence of physiologicalchanges was caused by inadequate trophoblastinvasion, confined to the decidual segments of thespiral arteries (Brosens et al., 1972). These histological observations provided the structuralbasis for a new insight in maternal flow regulationto the placenta. Indeed, the physiological changesinvolve a loss of the musculo-elastic vascularcomponents resulting in substantial dilatation,thus allowing an uninterrupted maternal bloodsupply to the placenta. It was postulated that,in the absence of vascular smooth muscle,such vessels can no longer respond to vasoactiveagents. In pre-eclampsia, on the other hand,non-converted arteries remain muscular andnarrow, and maternal blood flow to the placentamust therefore be reduced. Some of theseunchanged vessels may develop acute atherosis,but an important conclusion of these studies wasthat it is not the atherotic lesion, which occurs inonly a minority of spiral arteries (Khong andRobertson, 1992), which is the main pathologicaldefect, but the absence of physiological changes.Meanwhile, evidence was obtained to supportthe hypothesis that embedded cells in physiologically changed spiral arteries are trophoblastic innature. The presence of endovascular cellsin lumina of spiral arteries had been reportedin occasional first-trimester pregnancy specimensas early as 1870 by Friedländer (quoted by Boydand Hamilton, 1970). Much later, a histologicalcontinuity was demonstrated between endovascular cells and extravillous trophoblast (Hamilton andBoyd, 1960; Harris and Ramsey, 1966). A moreextensive quantitative study of trophoblast invasion in whole pregnant uteri from 8 to 18 weeks wasthen undertaken, which highlighted the existenceof two spatial pathways, interstitial and endovascular (Pijnenborg et al., 1980, 1981, 1983). Theprocess of interstitial trophoblast invasion of boththe decidua basalis and the inner myometriumstarts at the center of the implantation site andspreads toward the placental bed margins. Duringthe early second trimester this invasion processoften results in a ring-like trophoblast distributionwith lower cell counts at the center of the placentalbed. The interstitial mononuclear trophoblasticcells show progressive clustering and subsequentlyfuse to multinuclear giant cells, which are thoughtto be no longer invasive. Some of the interstitialtrophoblastic cells may surround spiral arteries andtake up a perivascular position. While during thefirst few weeks of pregnancy mononuclear interstitial trophoblast cells are likely to enter the spiralartery lumina in the superficial decidual compartment near the placental decidual junction, thereis no direct evidence of a direct transmuralinvasion of interstitial cells into the spiral arteriesdeeper in the myometrial compartment. On the
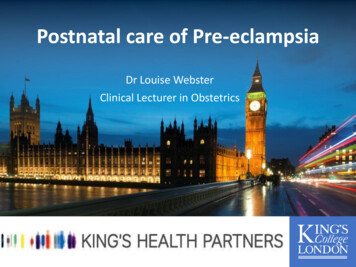
Trophoblast invasion in pre-eclampsia and other pregnancy disordersFigure 1.1 (a) Term placental bed biopsy showing spiral artery with physiological change near the decidual myometrial junction,characterized by replacement of the smooth muscle layer by fibrinoid (darkly stained) with embedded trophoblastic cells (T). PASstaining (bar ¼ 100 mm). (b) Same vessel. Cytokeratin immunostaining, revealing darkly stained trophoblast (T). (c) Same vessel. aActin immunostaining, showing replacement of the original vascular smooth muscle by fibrinoid. Streaks of intima thickening (*)stain for actin because of the presence of myofibroblasts. (d) Spiral artery with partial physiological change, showing intimalthickening (*) at the side of trophoblast invasion. PAS staining (bar ¼ 100 mm).contrary, histological continuity suggests anendovascular migration pathway from decidualto myometrial segments of spiral arteries, withmyometrial segments being invaded from 15 weeksonwards. In the original studies a time intervalof at least 1 month was found between endovascular trophoblast invasion of decidual andmyometrial segments, respectively (Pijnenborget al., 1983). Based on these observations theexistence of two successive waves of endovascularinvasion, with a temporary halt at the decidual myometrialjunction,waspostulated.In recent years this two-wave hypothesis hasbeen criticized, mainly based on studies of firsttrimester placental bed biopsies (Robson et al.,2001). Since biopsy material, in contrast tocomplete hysterectomy specimens, does not allowjudgment of the actual depth of invasion andassociated changes, this question needs to be reexamined.5
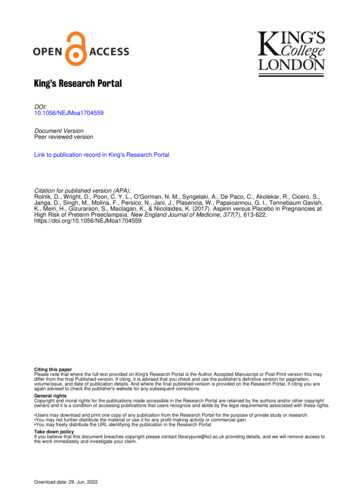
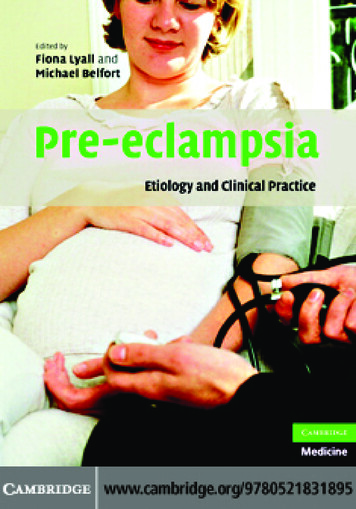
6R. Pijnenborg, L. Vercruysse, M. Hanssens and F. A. Van AsscheFigure 1.2 Diagrammatic representation of the different stepsin spiral artery remodeling. Step 1 shows endothelial (En)vacuolization. Step 2 involves early media (Sm) disorganizationand weakening of the elastica (Es), which is associated withbeginning dilatation of the vessel. In step 3, endovasculartrophoblast (T) appears in the arterial lumen. The next twosteps are depicted as a partial physiological change. In step 4,endovascular trophoblast becomes incorporated into the vesselwall, a process associated with fibrinoid (Fb) deposition. Theoriginal smooth muscle layer and elastica is replaced by thisfibrinoid material, while the embedded trophoblast acquires a‘‘spidery’’ shape. The final step (5) involves endothelial repairand occasional intimal thickening (left).In the myometrium as well as in the vasion. The associated spiral artery changesinvolve a series of steps, summarized diagrammatically in Figure 1.2 (more extensively reviewedby Pijnenborg et al., 2006). As a first step, earlychanges, involving vacuolation of endothelium andmedia, develop spontaneously, i.e. independent ofthe presence of the trophoblast. This first step isnot restricted to the placental bed, and maytherefore be associated with the decidualizationprocess (decidua-associated early vascular remodeling). The second step leads to further mediadisorganization as shown by a widening of intercellular spaces resulting in a loosely structured anddisrupted muscle coat. This early vascularremodeling is correlated with the presence of aninterstitial trophoblast, which therefore mayinduce extracellular matrix changes by phoblast-associated early vascular remodeling).As a third step, endovascular trophoblast appearsin the lumina of those vessels which have undergone the early remodeling. The fourth step involvesthe mural incorporation of this luminal trophoblast, which must therefore penetrate the vascularendothelium. It is often stated that at this stage thetrophoblast replaces the endothelium, but thereare indications that the latter is never completelylost and that trophoblast may penetrate theendothelium via intercellular gaps (J. N. Bulmer,personal communication, 2003). On the otherhand, there is evidence that the trophoblast isable to induce endothelial apoptosis, at least in anin vitro explant model (Ashton et al., 2005). Muralincorporation of the trophoblast is associated withthe deposition of fibrinoid material, which starts toaccumulate between trophoblastic cells while theyare still in a luminal position (Pijnenborg, 1996).The fibrinoid with incorporated endovasculartrophoblast then effectively replaces the vascularsmooth muscle layer, as can be demonstrated bythe absence of elastica and actin immunostaining.A remarkable feature of the fibrinoid-embeddedendovascular trophoblast is that it remains mononuclear, in contrast to the interstitial trophoblast.Furthermore, these trophoblasts also show acharacteristic ‘‘spidery’’ shape because of thepresence of irregular cell extensions, which isin marked contrast to the smooth outlines of thenon-fibrinoid-embedded interstitial trophoblast.The fifth and final step in the development of the‘‘physiological changes’’ involves the repair of
Trophoblast invasion in pre-eclampsia and other pregnancy disordersthe maternal endothelium, which may be associated with intimal thickening by proliferation ofmyo-intimal cells of maternal origin. Since endovascular trophoblast invasion only starts after thesecond step of interstitial trophoblast-related initialvascular remodeling, the full physiological changesof steps four and five will develop first in the spiralarteries at the center of the placental bed, graduallymoving to the more peripheral areas. Spiral arterychanges therefore follow the same spatial progression through the placental bed area as the interstitial trophoblast invasion. The time course of thesuccessive steps in the physiological change ofindividual spiral arteries is not known.At the time of the first histological mapping oftrophoblast invasion, all the evidence had to bederived from morphological continuities on serialhistological sections using standard staining techniques such as hematoxylin and eosin (H & E) andperiodic acid Schiff (PAS), because appropriateimmunohistochemical technology was not yetavailable. Later immunohistochemical studies onearly specimens largely confirmed the previouslydescribed patterns of invasion (Bulmer et al., 1984;Kam et al., 1999; Lyall, 2002; Robson et al., 2002).Extrapolating to pre-eclampsia, it was assumedthat absence of physiological changes in spiralarteries indicates a failure of the trophoblast toproperly invade the spiral arteries. This alsoimplied that, if impairment of trophoblast invasionis indeed a primary cause of pre-eclampsia, thedisease must originate in early pregnancy.Observations of restricted physiological conversion of spiral arteries in pre-eclampsia have beenconfirmed by many investigators over several years(Frusca et al.,1989; Gerretsen et al., 1981; Hanssenset al., 1998; Hustin et al., 1983; Khong et al., 1986;Lyall et al., 2001b; Meekins et al., 1994a; Moodleyand Ramsaroop, 1989; Pijnenborg et al., 1991;Sheppard and Bonnar, 1981). However, the originally proposed decidual/myometrial dichotomy,thought to reflect the two time-related waves ofendovascular trophoblast invasion, was counteredby the observation that restricted physiologicalchange did not exclusively involve the myometrialsegments of the spiral arteries, but that also someof the decidual segments might show defectivechange (Khong et al., 1986). The actual location ofthe spiral arteries in central or peripheral areas ofthe placental bed is probably an important determinant for the likelihood of failed conversion ofdecidual segments (Brosens, 1988).While searching for functional correlates of theextensive vascular changes or their absence inspiral arteries, maternal placental flow patternswere studied using Doppler imaging techniques.A correlation between the resistance index of theuterine arterial circulation and the depth ofphysiological changes in the placental bed wasindicated for the first time in a review article byMcParland and Pearce (1988), and has since thenbeen confirmed by other investigators (Aardemaet al., 2001; Lin et al., 1995; Olofsson, 1993; Sagolet al., 1999; Voigt and Becker, 1992). Flow patternscan also be obtained from individual spiral arteries.Matijevic and colleagues (1995) evaluated bloodflow through central and lateral spiral arteries at17 20 weeks, revealing lower resistance and pulsatility indices in the central arteries known toundergo p
Salt Lake City, Utah USA Fiona Broughton Pipkin . Pasadena, CA 91106 USA Robert Pijnenborg Department of Obstetrics and Gynaecology University Hospital Gasthuisberg Herestraat 49 B3000 Leuven, Belgium . Department of Radiology 5323 Harry Hines Blvd Dallas, TX 75390 USA F. Andre Van Assche