Transcription
PromiseSummer 2008ACuriousMind
Cover story16A Curious MindAlex Vannier’s curiosity for knowledge is not slowed by cancer.Features6RSV—Mild or Menacing?One virus has two drastically different outcomes. St. Judescientists ask, “Why?”8Fighting FatigueInvestigators study one of cancer’s most debilitating side effects.11Legacy of HopeA gold medallion arrives just in time to save a boy’s life.14Making Tumor Cells DisappearScientists figure out how to transform brain tumor cells intonormal brain cells.19Photo FinishRemembering his son, Jeff Carlin reaches out to St. Jude kids.20Ahead of the GameOne St. Jude patient hits his stride on the links.23Home on the WebPartners In Hope family members have a new “home” online.Highlights2News and AchievementsPerspective24Howard LesterPartners for the Kids14Promiseis a quarterly publication of theDepartment of Public RelationsSt. Jude Children’s Research Hospital262 Danny Thomas PlaceMemphis, Tennessee 38105-3678St. Jude has changed its mailing address to reflectthe hospital’s historical roots. The new address,262 Danny Thomas Place, represents February 1962,the date St. Jude opened its doors.Hospital Director andChief Executive OfficerDr. William E. EvansALSAC Chief Executive OfficerJohn P. MosesSt. Jude/ALSACChief Communications Officerand Senior Vice PresidentKen FerberDirector of Public RelationsJudith W. BlackPrint Production ManagerEditorElizabeth Jane WalkerArt DirectorJessica W. AndersonContributing WritersSummer FreemanJanice HillTara MilliganMike O’KellyCarrie L. StrehlauBetsy TaylorJoyce M. WebbPhotographersOlivier Ayrault, PhDPeter BartaSeth DixonAnn-Margaret Hedges
PromiseA publication of St. Jude Children’s Research Hospital Summer 20081120J Renee PhotographyMatteo TorriEditorial Advisory BoardLisa BakerLeah BrooksLeslie DavidsonMark HendricksChristine KirkJon McCullers, MDAva MiddletonJoseph Opferman, PhDCarlos Rodriguez-Galindo, MDCarrie L. StrehlauPenny TramontozziRegina WatsonSally WiardAmy ScottJohn ZacherSteve Zatechka, PhDPublic Information:1-866-2STJUDE (278-5833),ext. 3306Donations: 1-800-822-6344Visit our Web site at www.stjude.org.St. Jude Children’s Research Hospital,American Lebanese Syrian AssociatedCharities and ALSAC are registeredtrademarks.On the cover: photo by Seth Dixon.St. Jude Children’s Research Hospital’s missionis to advance cures, and means of prevention, forpediatric catastrophic diseases through researchand treatment. Consistent with the vision of ourfounder, Danny Thomas, no child is denied treatment based on race, religion or a family’s abilityto pay.St. Jude is an Equal Opportunity Employer. For inquiries about stories in this publication, call (901)595-2125 or e-mail elizabeth.walker@stjude.org.Articles may be reprinted with written permission. 2008.
wpeter bartaHighlights“The breadth ofDr. Laver’s careerand expertise isan ideal fit for theneeds of St. Jude.”Joseph Laver, MD, MHA, gets to know 5-year-old Joel Pounds duringa visit to the hospital’s Rehabilitation Services department.Laver to head hospital’s clinical programsSt. Jude has named Joseph Laver, MD, MHA, as its newclinical director and executive vice president.Laver, a nationally recognized expert in pediatriconcology and bone marrow transplantation, comes toSt. Jude from Virginia Commonwealth University MedicalCenter, where he chaired the department of Pediatrics andheld the Jesse Ball duPont Professorship in Pediatrics.Laver will head St. Jude clinical operations, includingclinical care delivery and patient care quality, and willoversee the consulting physicians and adjunct clinicalfaculty programs. Additionally, Laver will supervise theplanning and managing of the overall clinical space,systems and staff.Laver also served as medical director of Children’sHospital in Richmond, Virginia. He is the recipient ofnumerous professional honors, including Best Doctors inAmerica recognitions for many years.“The breadth of Dr. Laver’s career and expertise isan ideal fit for the needs of St. Jude,” said Dr. WilliamE. Evans, St. Jude CEO. “He brings the experience andacumen needed to provide knowledgeable leadership inthe treatment and care of children with cancer and other2 Promise / Summer 2008catastrophic diseases. Dr. Laver is a gifted individual,an accomplished pediatrician and a highly regardedadministrator. He will be an outstanding addition to ourpatient care, our research capabilities and our institution.”Laver studied medicine in Israel before trainingin pediatric hematology/oncology and bone marrowtransplantation at Memorial Sloan-Kettering CancerCenter in New York. He previously served as director ofthe division of Hematology-Oncology and Pediatric BoneMarrow Transplantation Service at Medical University ofSouth Carolina, in addition to holding the vice chairmanposition in the institution’s department of Pediatrics.“I am honored to join the outstanding physicians andscientists at St. Jude,” Laver said. “The close alignmentbetween exceptional clinical care and world-class researchmakes St. Jude an institution of national and internationalimportance.”A fellow of the American Academy of Pediatrics,Laver is a member of the Children’s Oncology Group,the American Society of Clinical Oncology, the AmericanSociety of Hematology and the American Society ofPediatric Hematology/Oncology.
Scientists uncoversecrets of rare formof ALLSt. Jude researchers have foundevidence that a series of geneticmutations work together to initiatemost cases of an aggressive and oftenfatal form of acute lymphoblasticleukemia (ALL).The defects include the deletion ofa gene, IKZF1, whose protein, Ikaros,normally helps guide the developmentof a blood stem cell into a lymphocyte.The researchers also found thatloss of the same gene accompaniedthe transformation of chronicmyelogenous leukemias (CMLs) to alife-threatening acute stage.“These findings provide newavenues to pursue to gain a betterunderstanding of these diseaseprocesses and, ultimately, to developbetter therapies,” said James Downing,MD, St. Jude scientific director andPathology chair.The study, which he and hiscolleagues reported in an April 2008issue of the journal Nature, addsfurther support to a key conceptin cancer genetics: Malignanciesfrequently require mutations inmultiple genes in order to develop.St. Jude researchers sought toidentify genetic differences betweenCML and a form of acute leukemiaknown as BCR-ABL1–positive ALL.Both diseases are characterized bythe Philadelphia chromosome, whichresults when parts of two differentchromosomes join together, and BCRABL1 is expressed.The scientists’ findings mayultimately offer insight into a betterway to treat the disease, Downing said.NCI designates St. JudeComprehensive Cancer CenterSt. Jude recently received the prestigious recognition of being designatedas a National Cancer Institute (NCI) Comprehensive Cancer Center.The designation makes St. Jude the first and only NCI-designatedComprehensive Cancer Center solely focused on pediatric cancer.“It is always gratifying to see one of the NCI-designated cancer centersachieve comprehensive status: recognition of excellence, not only in stateof-the-art care and cancer research, but also in patient education, communityoutreach and the dissemination of vital information to professionals and thepublic,” said John Niederhuber, NCI director, in the May 16, 2008, issueof The Cancer Letter. “This enhanced designation is a timely recognitionof important contributions and advances made by the dedicated staff ofSt. Jude.”In addition to a proven track record and impact in laboratory, clinicaland population-based cancer research, NCI-designated ComprehensiveCancer Centers must have significant efforts in professional and lay cancereducation and provide notable community service and outreach.Of the hundreds of institutions in the country that treat cancer patients,only 63 are NCI-designated Cancer Centers and receive funds from theNCI to support their infrastructure. Of those centers, only 41 have the“comprehensive” designation.The recent addition of the epidemiology and population researchprogram established the final scientific component needed for NCIComprehensive Cancer Center consideration, said Michael Kastan, MD,PhD, St. Jude Comprehensive Cancer Center director. The non-scientificrequirements for comprehensive status are education and communityoutreach. St. Jude has a long history of significant efforts in both areas.“Being designated a Comprehensive Cancer Center is a prestigiousaccomplishment, and to be the only pediatric center is an incomparabledistinction for St. Jude,” said Dr. William E. Evans, St. Jude CEO. “St. Judeis well known for having innovative programs led by the best and thebrightest faculty and staff; now being awarded ‘comprehensive’ statureplaces an additional NCI imprimatur on St. Jude and further validatesour position among the country’s leading cancer centers. This also speaksvolumes about Dr. Kastan’s strong leadership as our Cancer Centerdirector.”“This enhanced designation is atimely recognition of importantcontributions and advances made bythe dedicated staff of St. Jude.”Summer 2008 / Promise 3
Highlights“We need to find out those who are at riskso that we can spare them from toxicity.”Molecular science could increasesurvival ratesBy using new scientific techniques, the dramatic increase that has occurred in the curerate for children with acute lymphoblastic leukemia (ALL) may someday be replicatedin older patients, said St. Jude experts in the March 2008 issue of The Lancet.But to raise the survival rate of adolescents and adults with ALL, researchers need amore thorough understanding of the biology of this form of leukemia, including the rolegenes play in therapies, said Ching-Hon Pui, MD, Oncology chair.St. Jude research contributed to the high cure rate for children with ALL. “Wealready have 94 percent surviving at 5 years,” Pui said. But adolescents with ALL do notfare as well as children; and among adults with ALL, only 30 to 40 percent are cured.Pui and his colleagues said two areas of molecular science hold promise forimproving the survival and quality of life of ALL patients: genome-wide analyses ofleukemic cells and pharmacogenetic studies of host normal cells.“By studying messenger RNA (protein-coding gene) and microRNA expressionprofiles that are differentially expressed between different genetic subtypes of leukemia,it has been possible to identify novel pathways in malignant transformation, mechanismsof drug resistance and new targets for therapy,” Pui said.Pharmacogenetics is the study of how genes influence a person’s responses to drugs.“Certain drugs may be good for 99 percent of patients but bad for 1 percent,”Pui said. “We need to find out those who are at risk so that we can spare them fromtoxicity.”4 Promise / Summer 2008How T cells avoidautoimmunityA St. Jude study shows thatT cells, the body’s masterimmune regulators, do notuse simple on/off switches togovern the cellular machinerythat regulates their developmentand function. Rather, theypossess sophisticated molecularcontrols that enable them toadjust their function withexquisite precision. Such subtleadjustment enables T cells tomodulate their development andfunction, including avoidingautoimmunity.In autoimmune disease,rather than attacking invadingmicrobes, the immune systemattacks the body’s own organs,tissues or cells. Some 80autoimmune diseases are known,including type 1 diabetes,multiple sclerosis, rheumatoidarthritis and lupus.“A relatively small defectin the efficiency of how T cellsrespond to stimulation could giverise to a subtle failing in what’scalled negative selection. Thisprocess eliminates harmful cellsthat could cause autoimmunity,”said Dario Vignali, PhD, St. JudeImmunology. “Over a longperiod of time, a few overlyactive T cells that might initiateautoimmunity could escape thisprocess. Our studies suggest thatyou don’t need a big reductionin the responsiveness of T cellsto have a defect in the negativeselection process.”Vignali is the senior authorof a report on this work thatappeared in the journal NatureImmunology in May 2008.
Protein trio prevents cells from dyingSt. Jude investigators have discovered that the presence of three proteins protects certain cells from undergoingapoptosis, also known as programmed cell death.Apoptosis rids the body of damaged, mutated or infected cells. For example, cells that suffer irreparable DNAmutations undergo apoptosis to prevent them from forming a tumor. But molecular malfunctions that trigger apoptosismay actually cause some diseases, including Parkinson’s disease.In a series of experiments, St. Jude researchers found that if any of three molecules—Hax1, HtrA2 or Parl—ismissing, certain cells lose the ability to protect themselves from apoptosis. A report on this work appears in theFebruary 2008 edition of the journal Nature.“This is probably the first description of what is happening mechanistically that contributes to the ability of cellsto delay apoptosis,” said the paper’s senior author, James Ihle, PhD, Biochemistry chair. “It provides incredible insightsinto how three proteins work and how they can control apoptosis.”The molecular interactions occur in nerve cells and blood cells that develop from blood-forming stem cells.Understanding the biochemical interactions that control the extent of apoptosis could help scientists learn tocontrol this process and could lead to new treatments.“It provides incredible insightsinto how three proteins work andhow they can control apoptosis.”Your hair cells are dancingSt. Jude investigators have found that an electrically poweredamplification mechanism in the cochlea of the ear is critical to the acutehearing of humans and other mammals. The findings will enable betterunderstanding of how some kinds of hearing loss can occur.For several years, Jian Zuo, PhD, Developmental Neurobiology, hasbeen studying hearing, since children often experience hearing loss as aside effect of cancer treatment.Sound is detected by the vibration of tiny, hair-like cilia that extendfrom cochlear hair cells. While the cochlea’s “inner hair cells” are onlypassive detectors, the so-called “outer hair cells” amplify the sound asit transforms into an electrical signal that travels to the brain’s auditorycenter.Zuo and his colleagues sought to find out how outer hair cellsproduce such amplification.Sound signals are amplified by a protein called prestin that isembedded in the outer hair cell membrane. Prestin is powered by voltageswithin the membrane that are produced by mechanical sound vibrations.When an outer hair cell is stimulated by sound, the cell body elongatesand contracts along with the sound, in a “dancing” action.Zuo found that the “dancing” movement of the outer hair cells iscritical to cochlear amplification. He is senior author of a report on thiswork that appeared in the journal Neuron in May 2008.By finding prestin’s role in hearing, Zuo and his colleagues may helpscientists better understand the mechanisms of hearing loss.Summer 2008 / Promise 5
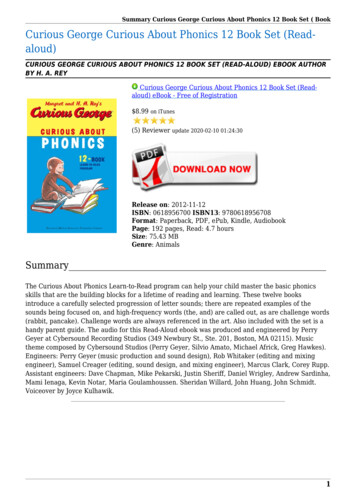
Devan Lore’s first bout with a common wintertime virus gave thetoddler a weeklong runny nose and cough. While the illness was anadded burden for the child, who was undergoing treatment for acutelymphoblastic leukemia, the virus soon cleared.At age 6, Devan again caught the respiratory syncytial (pronouncedsin-SISH-ul) virus, or RSV. This time the results were terrifying.Within days, the virus moved deep into Devan’s lungs, causingpneumonia, necessitating a move to the Intensive Care Unit at St. JudeChildren’s Research Hospital. The boy spent 12 hours a day in an oxygentent, where he inhaled an antiviral drug.“From 8 p.m. to 8 a.m. for five days,” recalls Gail Lore, Devan’smother. “I wanted to reach out, hold him, cuddle him—and couldn’t.”RSVB y S ummer F reemanMore than a coldDevan’s two brushes with thevirus typified how RSV infectioncan develop in completely differentways. In both instances, Devan’simmune system was weakenedfrom chemotherapy, but his firstround with the virus produced coldlike symptoms, while the secondthreatened his life.To better understand thedifference in response, investigatorsreviewed the cases of St. Judepatients who had experienced RSVinfections. The researchers soughta common thread that would helpthem identify which children were atgreatest risk.“Before our study, mostinformation about RSV infectionin patients with cancer came fromadult patients—information that wasnot necessarily applicable to thechildren we treat,” says Aditya Gaur,MD, of St. Jude Infectious Diseases.“We needed data from children andadolescents with cancer to be ableto put together RSV managementguidelines. We wanted to know ifthere were characteristics that wouldtell us up front which patients mighthave a particularly severe course ofRSV infection.”Mild or Menacing?Devan Lore’s first RSV infection made him cough. The second onesent him to the ICU. What accounted for the drastic difference?Following this regimen, Devan continued around-the-clock breathingtreatments.“It was two weeks before he was well enough to be taken off oxygen,and he was still so weak afterwards,” Gail says. “It was easily our roughestpatch at St. Jude.”Although usually associated with cold-like symptoms, RSV is the mostcommon cause of bronchiolitis and pneumonia among children under 1 yearof age. Repeated RSV infections can occur throughout life in otherwisehealthy people. The virus can present severe problems in those who areextremely young, elderly or in people who have compromised cardiac,pulmonary or immune systems. For children with cancer, especially thosewho have had recent bone marrow transplants, the virus can be deadly.6 Promise / Summer 2008His life-threatening bout with RSV behindhim, Devan Lore plays with bubbles onthe Target House playground.
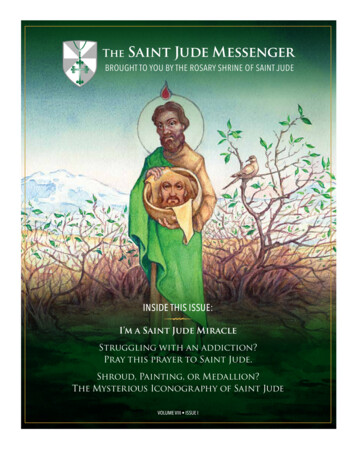
photos by peter barta“The new information isimportant because it helpsidentify children who are mostat risk for severe disease.”for infections based on patientshaving abnormally low levels ofneutrophils,” Gaur says. “But ourstudy shows that for RSV, low levelsof lymphocytes and not neutrophilsidentify those at risk for severedisease.” Total neutrophil count andtotal lymphocyte count are bothavailable as part of routine blood testsfor patients with cancer.Asking the right questionsAditya Gaur, MD, chats with Devan Lore in an isolation room at St. Jude. Gaurand his colleagues have discovered why some children develop serious illnessfrom RSV infections.Lymphocytes are keyThe research team studied theSt. Jude records of 58 children withcancer who had tested positive forRSV between 1998 and 2005.The investigators found thatchildren under 2 years old and thosewith low levels of lymphocytes—infection-fighting white blood cells—are at high risk for more severe RSVrelated disease.“The new information isimportant because it helps identifychildren with cancer who are mostat risk for severe disease by usingeasily available clinical information,”Gaur says. “The findings don’t implythat all patients with one or bothrisk factors will develop a seriousRSV infection, but they tell us whoneeds to be considered for antiviraltherapy, which is costly and ofteninconvenient to receive from a child’sperspective.”Investigators also found that theycould predict risk more accuratelyby evaluating a child’s lymphocytecount instead of the neutrophil count.Neutrophils are immune system cellsthat engulf and digest germs.“With cancer patients, cliniciansare used to identifying those at riskThe project began three yearsago, when Gaur and former St. Judefellow C. M. El Saleeby, MD, treatedtwo children who had life-threateningRSV infections.“When you have someone whois very sick, you try your best tofind the answer that will help and toask yourself whether the severity ofsickness could have been predicted,”Gaur recalls. “There was informationabout adults, but the informationwasn’t there for the children we weretrying to treat.”El Saleeby and Gaur started toask questions that were not beingposed about pediatric patients; in sodoing, they found new answers thatpromise to improve care for thesechildren.“While the RSV managementguideline that has been developedbased on our study’s findings is agood first step toward optimizingtreatment of this infection, furtherresearch is necessary,” Gaur says.“Ultimately, good, consistent handhygiene at home and in the hospitalis the most cost-effective way ofpreventing not only RSV but manyother viral infections.”All of these findings by Gaurand his colleagues are sure to makekids—as well as moms like GailLore—breathe much more easily. lSummer 2008 / Promise 7
FightingFatigueby elizabeth jane walkerNausea. Hair loss. Pain. These are just a few of“Dex time is coming, and my child is never my childthe problems that plague children undergoingduring dex,” parentscancer treatment. But the issue that kidswould say.overwhelmingly cite as the most debilitating ofCourtney soon learned the truth of that adage. “Whenall may surprise you. It’s fatigue—a bone-deep lethargy, aI was on dex, I was mean,” she admits. “That’s the niceponderous weariness that pins children to theway of putting it. I couldn’t sleep, and Ibed and interferes with their ability to laugh,would toss and turn all night. As a result, Ilearn and even heal. It’s more than just afelt really tired, and I was always grumpy.”minor inconvenience; it’s a serious problem.Watching her daughter’s distress evokedAnd researchers at St. Jude Children’sfeelings of utter helplessness in LauraResearch Hospital are determined to doBarnett.something about it.“I could do things to help the nausea;When Courtney Barnett began treatmentI could take care of some of her otherfor acute lymphoblastic leukemia (ALL),problems,” Laura says. “But when your childthe teen learned that she must take a steroidjust sits there and looks at you and criescalled dexamethasone for much of her twobecause she’s so tired, there’s nothing youIn the hospital’s fatigueand-a-half years of therapy. Traditionally,can do but hold her.”studies, patients wearpatients and parents have warned one another actigraphs that measureabout the drug’s effects.activity levels.8 Promise / Summer 2008SNOIATCINUMMOC LACIDEMOIBResearchers at St. Jude take aim at one of the mostserious side effects of cancer therapy—fatigue.
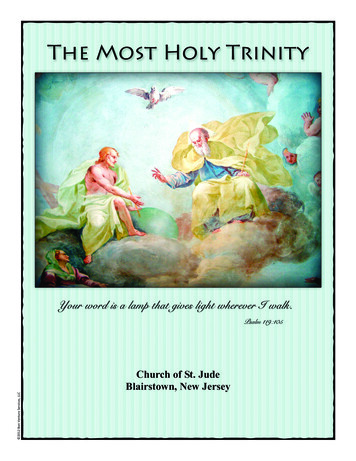
For kids undergoing cancer therapy, sleep isone of the best medicines, critical for proteinsynthesis and cell regeneration.Rude awakeningFor kids undergoing cancer therapy, sleep is one ofthe best medicines, critical for protein synthesis and cellregeneration. “Children are especially vulnerable becausethey are growing,” says Jami Gattuso, RN, who has beeninvolved in St. Jude sleep research for 10 years. “Theyneed energy for development of their brains and bonesand muscles. But on top of that, sleep is important foryour immune system, which can help in fighting cancer.”Children who are battling fatigue often miss outon school, extracurricular events and other enrichingactivities. They have problems learning, and they maybecome alienated from friends who lead more activelifestyles.When researchers from St. Jude approached theBarnett family about participating in a sleep and fatiguestudy, they enthusiastically agreed. After all, Courtney wasnot the only one affected by the problem. When kids haveinsomnia, parents keep vigil.“As a result, everybody in our family was prettyirritable,” Laura says. “But we knew that taking dex isone of those necessary evils. She had to take it for hertreatment and make the best of it.” The Barnetts hopedthat the research project would help other children avoidthe problems Courtney was experiencing.Studying slumberAs part of the study, 100 children and teensagreed to wear actigraphs, which resemble sleek, blackwristwatches. The device contains a computer chip thatrecords activity levels. Participants wore the monitors forfive days before and five days during administration ofdexamethasone.Some children needed reassurance before they wouldagree to wear the actigraphs, recalls Pamela Hinds, RN,PhD, St. Jude Nursing Research director. “One little guyDexamethasone causes patients like 7-yearold Jashaylin Jackson to suffer debilitatingweariness during treatment.Spring 2008 / Promise 9
seth dixonPamela Hinds (at right), RN, PhD, andJami Gattuso, RN, study how cancertreatment affects the fatigue level ofchildren. “Nocturnal awakenings formost kids who are older than age 2are generally zero to five per night.Our kids had, on average, 13 to 16 pernight—and sometimes up to 40,” saysHinds, who is leading a new project tohelp alleviate the problem.asked me, ‘If I wear this, can you tell if I’m lying?’ I said,‘No, I cannot tell when you’re lying.’ He said, ‘Well,then, I’ll do it.’” Other children pretended that the deviceimbued them with super powers.Patients and parents kept sleep diaries and completedsurveys that recorded activities, moods and fatigue levels.Researchers also conducted tests to determine how thechildren metabolized the drug.The investigators ultimately discovered what parentsalready suspected: Dexamethasone routinely disrupts thesleep of patients and is not just a problem that affectsspecific children or age groups.“Nocturnal awakenings for most kids who are olderthan age 2 are generally zero to five per night,” Hindssays. “Our kids had, on average, 13 to 16 per night—andsometimes up to 40.”Dream it, do itNow that they understand the extent of the problem,St. Jude researchers are focused on finding a solution.In the hospital’s newest ALL treatment study, thedexamethasone dosages in one phase of treatment arelower than the ones Courtney received. The study team isalso studying the pharmacogenetics related to sleep anddexamethasone. Using blood samples obtained duringthe previous study, scientists are exploring the role of aprotein called albumin. Investigators suspect that whenchildren have low levels of albumin, they may have moreexposure to dexamethasone and thus more disturbedsleep.The study team is also examining the blood samplesfor two cytokines, messenger proteins that allow cells tocommunicate with one another. The scientists theorizethat these cytokines become unbalanced and cause sleep10 Promise / Summer 2008disturbances. “There are treatments that can be usedwith cytokines to get them in balance,” Hinds explains.“So we’re hoping that through these mechanisms we’regoing to be able to help our patients avoid this negativeexperience.”A two-year study that begins this summer is aimedat reducing fatigue and disrupted sleep in children withthe brain tumor medulloblastoma. The study incorporatesseveral components: education about sleep and fatigue,relaxation techniques, window coverings to eliminateexcessive light, and “white noise” to muffle sounds andpromote a relaxing environment.Researchers have found that staff memberssometimes enter a child’s hospital room as many as 40times during the night. As part of the new study, nurseswill coordinate care, so that they do not have to enter theroom as frequently. “For instance, if a child needs vitalsigns taken and hydration—tasks usually done by twodifferent team members—the individuals will enter theroom together and do that care at the same time,” Hindssays.“Making the hospital environment more conducive tosleep will be great,” Gattuso predicts. “We’re excited tobe doing this intervention.”St. Jude families say they appreciate the researchers’attempts to reduce fatigue. Courtney’s mom says it’s justone more area in which St. Jude excels.“If every hospital in the country could be runhalf as efficiently as St. Jude, and half as caring, therewouldn’t be any problem with our medical system in theU.S.,” Laura says. “When Courtney was diagnosed, herpediatrician said that St. Jude was the best place that shecould go. And he was right.” l
Legacy of HopeB y J oyce M. W ebbphotos by Ann-Margaret HedgesWas it coincidence that twodistraught parents received a St. Judemedallion just as they were seeking ahospital to save their son’s life?Summer 2008 / Promise 11
SSometimes a “mere coincidence” can have life-changingconsequences. Just ask Patrick and Kristin Trysla. Anunexpected gift helped this couple make a decision thatsaved their baby’s life.Their son, Clayton “Clay” Trysla, was born with amuscular disorder that caused his head to tilt slightly toone side and eventually flatten in the back. The Tryslasrequested a CT scan, which showed no abnormalities.Kristin began to notice signs of extreme fatigue in hernormally energetic son. Then she noticed that Clay couldno longer use his left arm to grab his feet while having hisdiaper changed. A pediatrician suggested that his elbowwas out of socket, but Kristin’s maternal instincts told herotherwise.“I was very uncomfortable with that diagnosis,” sherecalls.Less than 24 hours later, Clay started throwing up.The Tryslas took him to the emergency room and askedfor another scan. That’s when a team of doctors deliveredthe disturbing news.“There’s no easy way to say this; he’s got a largemass in his brain, and it’s going to have to come out assoon as possible,” the doctors said.Million-dollar questionThe mass was an aggressive brain tumor known asprimitive neuroectodermal tumor or PNET, located in thepart of Clay’s brain that controls movement, orientationand recognition. This kind of cancer is extremely rare inchildren younger than 3 years old.At 7 months old, Clay underwent an operation toremove the tumor.“I remember these words exactly. They said, ‘We goteverything we could see.’ As a parent, you want to hear,‘We got it all,’” Kristin recalls.Because their local hospital had treated fewPNET cases like Clay’s, the Tryslas explored otherinstitutions that specialized in treating infants with rarebrain tumors. Clay’s dad, Patrick, tapped into his ownsiblings’ experience in health care to identify and consultwith leading neuro
Memphis, Tennessee 38105-3678 St. Jude has changed its mailing address to reflect . St. Jude from Virginia Commonwealth University Medical Center, where he chaired the department of Pediatrics and . Joseph Laver, MD, MHA, gets to know 5-year-old Joel Pounds during a visit to the hospital's Rehabilitation Services department. w