Transcription
Reuse of Needles White Paper 07D01507001512/20/0612:42 PMPage 1A Look at the Reuseof Insulin Needles1 Becton DriveFranklin Lakes, NJ 07417www.BDdiabetes.com/usBD and BD Logo are trademarks of Becton, Dickinson and Company. 2006 BD07D015070015ReuseWP
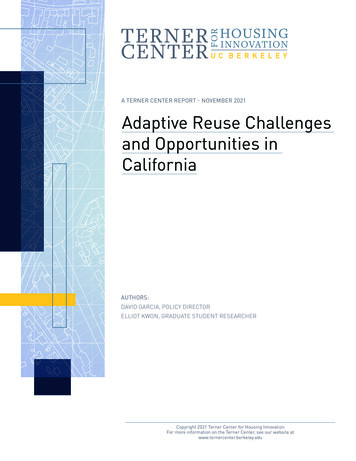
Reuse of Needles White Paper 07D01507001512/20/0612:42 PMMoving ForwardBD, the leading manufacturer of insulin needles,is making a commitment to begin educatingpatients about the risks associated with reuse ofinsulin needles by doing the following:1. A statement advising against reuse will beadded more prominently to syringe, penneedle and lancet boxes and syringe 10-packbags.2. Patient literature including photos from themicroscopy study will be included in syringebox inserts, patient mailings and in literatureavailable to health care professionals fordistribution to patients.3. Slides of the enlarged reused needles will beavailable for use at patient training classes,upon request.4. For pen users, BD will make available a smallpouch on a key-chain that can be used tomake it more convenient to carry needleswhen they are away from home.It is recommended that those training patientsto inject insulin do the following:1. Include a discussion on the risks of needlereuse in their patient training sessions. Patients should be taught to understand thatwhen they dispose of a syringe, pen needleor lancet after one use, they are not beingwasteful, but rather, they are helping reducetheir risk of tissue damage and of havingneedle tips embedded in their skin. Since as a practical matter, patients will notbe able to examine their reused needlesunder a high-powered electron microscope,all patients should be advised to assume thatthey are among the vast majority of patientsin whom the needle tips become hooked orbroken off with repeated use.2. Include the number of needles or lancetsneeded per day on all prescriptions forsyringes, pen needles and lancets and advisepatients not to accept fewer needles orlancets than they need, from their plan.Page 3ReferencesFood & Drug Administration: Compliancepolicy guidelines. Sec. 300.500, Reuse ofMedical Disposable Devices (CPG 7124.16)Washington DC (1997)Franzen I, J. Ludvigsson: Specific InstructionsGave Reduction of Lipomas and ImprovedMetabolic Control in Diabetic Children.Diabetologia Vol 40, Supplement 1: A615(1997)Ginsberg, B.H., J.L. Parkes, C. Sparacino: Thekinetics of insulin administration by insulinpens. Horm. Metab. Res. 26: 584-587 (1994)Hauner H., B. Stockamp, B. Haastert:Prevalence of lipohypertrophy in insulintreated diabetic patients and predisposingfactors. Exp Clin Endocrinol Diabetes 104:106-110 (1996)Look, D, K Strauss: Reuse of sharps in diabeticpatients: is it completely safe? DiabetesJournal 10: 31-34 (1998)Reach G, M. Cahane, M. Vins, et al.: HbA1c inchildren attending summer camps organisedby l’Aide aux Jeunes Diabetiques. Evidencefor a harmful effect of lipohypertrophies inthe early years of diabetes. Diabetes Metab.19: 194-200 (1993)Saez-de Ibarra, L., F. Gallego: Factors related tolipo- hypertrophy in insulin-treated diabeticpatients: role of educational intervention.Practical Diabetes International. 15: 9-11(1998)Wintrobe: Clinical Hematology, Lea & Febiger,9th edition (1993)A Look at the Reuse of Insulin NeedlesThe Early Days of Needle ReuseIn the early days of insulin administration,patients injected insulin using glass syringeswith detachable needles. The users had to boilthe needles between uses and soak them inalcohol to sterilize the needles as best theycould. To make the pain of injections morebearable, users spent hours sharpening theirneedles on a stone between uses to try toreverse the comfort deterioration fromrepeated use.Over the years, manufacturers have madedramatic improvements in the comfort andconvenience of insulin injections. With theintroduction of disposable, single-use insulinsyringes with attached needles, users were freedfrom the arduous tasks of boiling, soaking andsharpening. With the disposable syringes camethinner needles, improvements in the needlepoint geometry and a freshly lubricated needlefor every injection. Therefore, comfort ofinjections improved and the tissue traumaassociated with injections declined.Reuse and Disposable SyringesWhen disposable syringes were first introduced,most users fully embraced the concept of singleuse disposable syringes and used them once asintended. Others used the disposable syringes,but did not use them only once. “It is wastefulto throw away a perfectly good syringe afterone use” they may have reasoned. Thesepatients used their disposable syringes multipletimes, and may have made up their ownregimen to care for the syringes between uses;some continuing to soak them in alcoholbetween uses or wiping them with alcohol andothers storing them in the refrigerator.Call BD Health Care Professional Services at1-888-367-9539 (Monday-Friday, 9 a.m. to 5 p.m.,Eastern Time) if BD may be of service in helpingyou to help your diabetes patients.Consequently, there was and still is awarenessby professionals that some patients reusedisposable syringes. Despite syringe labels thatadvise single-use only, this perception appearsto have resulted in health care professionalsdeveloping occasional “unofficial” guidelinesranging from “use each syringe for no morethan one or two days” to “use a syringe until itis no longer comfortable.” Other cautions mayhave included directions not to soak the needlesin alcohol or wipe them with alcohol betweenuses (to avoid making the needles lesscomfortable by removing the lubricant).Although one might imagine that patients whoreused syringes would get infections at theinjection site from using non-sterile needles, infact infections were reported infrequently.There were studies documenting that painincreases with needle reuse, but acceptable painlevel was viewed as a personal matter for thepatient to decide, and not a medical matter aslong as the increased pain didn’t negativelyimpact compliance with the prescribed injectionregimen. As a result, some patients may havebeen advised that as long as only one personused the needles, bathed regularly and tookall of the required injections, they could reusethe syringes.Today, it is recognized that reuse of insulinneedles is not uncommon, even among youngerpatients who did not have the personal historyof having once used glass syringes withdetachable needles. The most common reasonfor reuse of insulin needles is not cost. Instead,convenience and a reluctance to throw awaysomething that is not yet “worn out” or“finished being used,” are the most prevalentreasons for reuse. Over 70% of patients whoinject insulin have insurance that covers theirneedles, and yet many still prefer to reuseinsulin needles.Needles Became Even ThinnerSince the introduction of disposable insulinsyringes, manufacturers have continued toinnovate and offer thinner, even morecomfortable needles. When the outer diameters ofthe needles became thinner, the inner diameters(inner lumen, that the insulin passes through)were not reduced in size proportionately. Onereason for this was that if the inner lumen weretoo narrow, it would take an unacceptably longtime to fill a syringe. Another was a concern thatthe force on the plunger, required to push theinsulin through a very narrow passageway, wouldbe too great. As shown on the chart below, whenthe outer diameters of the needles droppedsignificantly, so did the wall thickness of theneedles. The 0.063mm wall thickness of today’s31G needle is the thickness of 4 white blood cells.(Wintrobe, 1993).Needle Dimensions (mm)GaugeOuter DiameterWall Thickness24253031.559.508.305.254.133.133.076.063
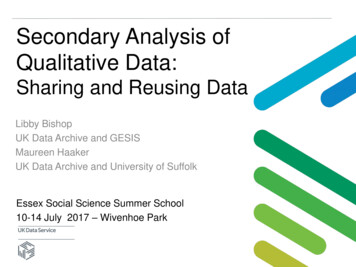
Reuse of Needles White Paper 07D01507001512/20/0612:42 PMPage 5As needles and their wall thickness becomesmaller, reuse becomes more of a problem,because of the potential of needle tips to bendinto the form of a hook and break withrepeated use. The needles are so fine that thetip damage cannot be seen with the naked eye.It can only be seen with high-resolutionelectron microscopes.INSULINSpecial Considerations for Pen NeedlesThere are additional concerns when it comes toreuse of insulin pen needles. Reuse of insulinpen needles is almost always accompanied bycarrying the pen with the needle attached. Forgreater convenience, some patients report usingonly one pen needle for each disposable pen orinsulin cartridge, carrying the device with theneedle attached, between uses. Therefore, penusers who carry their pens with the needleattached, risk micro-tissue damage. The same istrue of syringe users who reuse. A pen needle isa two-ended needle, with one end that puncturesthe insulin cartridge and the other end thatpenetrates the skin. By leaving a needleattached to a pen, even if the needle is covered,patients are leaving an open-passageway into theinsulin cartridge. A study entitled The Kineticsof Insulin Administration by Insulin Pens(Ginsberg, Parkes, and Sparacino 1994)demonstrated that air enters insulin cartridgeswhen the pen needle is left on the pen and thepen is exposed to alterations in temperature.When patients carry the pen from warm placesto cool places (such as when they go outdoors inwinter, or into an air-conditioned building insummer) the insulin in the pen contracts, drawingair into the cartridge through the attachedneedle. When there is added air in an insulincartridge, the dose delivered is very inaccurateand up to 2/3 of the dose may not be delivered.0AIRConversely, when patients carry the pen from coolplaces to warm places (such as when they gooutdoors in summer, or into a heated building inwinter), the fluid in the cartridge expands and leaksout though the attached needle. If the cartridgecontains NPH either alone, or as part of a premix,and the patient has not just re-suspended theinsulin chances are that the crystals will be settledon the bottom of the cartridge and what will leakout will be fluid without crystals. This will changethe concentration of the insulin that remains in thecartridge, altering the effectiveness of future dosesfrom that cartridge or pre-filled pen.The study concluded that “patients should beinstructed to remove the insulin pen needleimmediately after each injection and onlyreplace it with a fresh needle just before thenext injection.If patients follow this simpleprocedure and remove their needle after eachinjection, the insulin pen is a safe, accuratedevice.”There are some patients who do not carry theirpens with the needle attached, but who do reusethe needles. For these patients there is anadditional issue with how they keep the backend of the needle clean between injections.New pen needles come with a paper seal overthe end of the needle that penetrates the insulincartridge. Once this seal is removed to attachthe needle to the pen, there is not a good way tokeep the needle clean between uses.When syringes are reused the needle is placedinto the bacteriocidal insulin solution betweenuses. This may be why there are fewer infectionsthan expected. This is not true of pen needles inwhich bacteria are free to grow on the needles.Microscopy FindingsIn three studies on reuse conducted at theKlinik Hellbachtal in Germany in 1997 patientswere asked to save their pen needles andlancets after use, and label them with thenumber of times they had been used. Electronmicrographs were taken at the University ofGrenoble, France, during 1997 by Dr. JacquesGarden of pen needles and lancets that hadbeen used by patients, according to their ownnormal reuse patterns in the treatment of theirdiabetes. The needles were then photographedunder microscopic powers ranging from 370x to5000x. The observers noted the following (Look,Strauss 1998): Significant tip damage can occur after only oneinjection and was seen with all manufacturersstudied. The majority of needles and lancets showedtip damage when reused, despite the fact thatpen needles only penetrate human skin witheach use, not a vial stopper. Some needles were actually missing their tips— raising the question of whether the tipsmight be imbedded in the patient’s skin. Tip damage did not always increaseproportionately with the number of times theneedle was used. There were patients whoseneedles remained in good condition withrepeated use. Therefore, skin type andinjection technique may play roles in thedegree of needle tip damage after use. Inactual practice though, all reuse must bediscouraged, as the damage occurs to such asmall area of the needle tip that it cannot bedetected without a high powered electronmicroscope — even where the needle tip hasbroken off.While reused syringes were not included in thisparticular study, it is reasonable to assume thatthe damage to reused syringe needles is evengreater than the damage to reused pen needlesand lancets, as syringe needles must go thoughthe rubber stopper of syringe vials before eachskin penetration.Photographs showing the type of damage thatcan occur with needle reuse.*a correlation between reuse andlipodystrophy. While “lipos” are notfrequently reported, it is estimated that 2045% of injecting patients with Type 1diabetes mellitus and 3.6% with Type 2diabetes mellitus will have “lipos” (Saez-deIbarra, Gallego 1998) once a search isconducted. These are often easier to feelthan to see and can be disfiguring. Peopleoften prefer to inject into them because itis less painful.Lipodystrophy and ControlA study published at the 1997 InternationalDiabetes Federation (IDF) conference,Helsinki, Finland (Franzen, Ludvigsson, 1997)found that in the study group, versus control,HbA1C decreased with “lipo” decrease. Theaverage decrease was between 7.0 and 7.9% inthe experimental group, versus no change in thecontrol group. In the experimental group, theimprovement in lipohypertrophy and HbA1Ccame about after intensified instructionregarding injection technique (site rotation)and clean needle use while the controlgroup received traditional instruction ininjection technique.FDA GuidelinesUsed needlemagnified 370 timesSame used needlemagnified 2000 times* Photographs from Dieter Look and Kenneth Strauss study:"Nadeln mehrfach verwenden?" Diabetes Journal 1998, 10: S. 31-34.Medical Consequences of Needle Reuse“Reuse of Sharps in Diabetic Patients: Is ItCompletely Safe?” (Look, Strauss 1998)analyzed the three studies conducted by D.Look at the Klinik Hellbachtal in Molln,Germany in 1997 and drew the followingconclusions based on the evidencedemonstrated in the studies.1. Tissue microtrauma: When a deformed needleis used, it lacerates tissue, causingmicrotrauma. This can result in locallysignificant bruising and bleeding. Volunteersin the German studies who reused lancetswere found to have more residual bleeding insites where a more heavily reused lancet wasemployed for the blood letting.2. Embedded needle tips: The studies showedthat excessive reuse ( 7 times/needle) wasoften associated with a breaking off of themicroscopic end of the needle tip. Themedical consequence of embedded metal tipsis unknown at this time.3. Correlation with greater incidence oflipodystrophy: According to the analysis ofthe German studies cited above, local growthfactors may be released and join with insulinto form lumpy nodules called “lipodistrophy.”Although at this time there is not proof thatreuse leads to lipodystrophy (“lipos”), there isRecently there has been a great deal of mediacoverage about the practice of institutionsreusing medical devices that are labeled asbeing for single use. The FDA CompliancePolicy Guidelines Sec. 300.500 (1987) states:“Since disposable devices are not intended bythe manufacturer or distributor for reuse, anyinstitution or practitioner who re-sterilizesand/or reuses a disposable medical devicemust bear full responsibility for its safetyand effectiveness.Insurance ConcernsWhen patients who have been reusing syringesstop reusing, there are bound to be concernsabout whether their insurance will cover theincreased number of syringes that are required.For example, if a patient takes three injectionsper day, and in the past has been using eachsyringe three times, his or her mail order planmay have been sending one box of 100 syringesevery three months. In this case, the plan maybe dispensing one syringe per day, not becausethey expect their members to reuse, but becausethey were never advised that the patient wastaking three injections per day. If a plan doescover syringes, however, it should cover theproper number that will allow the patient to usethem according to the directions. Therefore, ifpatients are not being given enough syringes touse one syringe per injection, they should advisetheir pharmacist or plan of the number ofneedles they need per day. To help avoid theseproblems, prescribers should make it a practiceto indicate the number of needles needed perday on the prescription.
Reuse of Needles White Paper 07D01507001512/20/0612:42 PMPage 5As needles and their wall thickness becomesmaller, reuse becomes more of a problem,because of the potential of needle tips to bendinto the form of a hook and break withrepeated use. The needles are so fine that thetip damage cannot be seen with the naked eye.It can only be seen with high-resolutionelectron microscopes.INSULINSpecial Considerations for Pen NeedlesThere are additional concerns when it comes toreuse of insulin pen needles. Reuse of insulinpen needles is almost always accompanied bycarrying the pen with the needle attached. Forgreater convenience, some patients report usingonly one pen needle for each disposable pen orinsulin cartridge, carrying the device with theneedle attached, between uses. Therefore, penusers who carry their pens with the needleattached, risk micro-tissue damage. The same istrue of syringe users who reuse. A pen needle isa two-ended needle, with one end that puncturesthe insulin cartridge and the other end thatpenetrates the skin. By leaving a needleattached to a pen, even if the needle is covered,patients are leaving an open-passageway into theinsulin cartridge. A study entitled The Kineticsof Insulin Administration by Insulin Pens(Ginsberg, Parkes, and Sparacino 1994)demonstrated that air enters insulin cartridgeswhen the pen needle is left on the pen and thepen is exposed to alterations in temperature.When patients carry the pen from warm placesto cool places (such as when they go outdoors inwinter, or into an air-conditioned building insummer) the insulin in the pen contracts, drawingair into the cartridge through the attachedneedle. When there is added air in an insulincartridge, the dose delivered is very inaccurateand up to 2/3 of the dose may not be delivered.0AIRConversely, when patients carry the pen from coolplaces to warm places (such as when they gooutdoors in summer, or into a heated building inwinter), the fluid in the cartridge expands and leaksout though the attached needle. If the cartridgecontains NPH either alone, or as part of a premix,and the patient has not just re-suspended theinsulin chances are that the crystals will be settledon the bottom of the cartridge and what will leakout will be fluid without crystals. This will changethe concentration of the insulin that remains in thecartridge, altering the effectiveness of future dosesfrom that cartridge or pre-filled pen.The study concluded that “patients should beinstructed to remove the insulin pen needleimmediately after each injection and onlyreplace it with a fresh needle just before thenext injection.If patients follow this simpleprocedure and remove their needle after eachinjection, the insulin pen is a safe, accuratedevice.”There are some patients who do not carry theirpens with the needle attached, but who do reusethe needles. For these patients there is anadditional issue with how they keep the backend of the needle clean between injections.New pen needles come with a paper seal overthe end of the needle that penetrates the insulincartridge. Once this seal is removed to attachthe needle to the pen, there is not a good way tokeep the needle clean between uses.When syringes are reused the needle is placedinto the bacteriocidal insulin solution betweenuses. This may be why there are fewer infectionsthan expected. This is not true of pen needles inwhich bacteria are free to grow on the needles.Microscopy FindingsIn three studies on reuse conducted at theKlinik Hellbachtal in Germany in 1997 patientswere asked to save their pen needles andlancets after use, and label them with thenumber of times they had been used. Electronmicrographs were taken at the University ofGrenoble, France, during 1997 by Dr. JacquesGarden of pen needles and lancets that hadbeen used by patients, according to their ownnormal reuse patterns in the treatment of theirdiabetes. The needles were then photographedunder microscopic powers ranging from 370x to5000x. The observers noted the following (Look,Strauss 1998): Significant tip damage can occur after only oneinjection and was seen with all manufacturersstudied. The majority of needles and lancets showedtip damage when reused, despite the fact thatpen needles only penetrate human skin witheach use, not a vial stopper. Some needles were actually missing their tips— raising the question of whether the tipsmight be imbedded in the patient’s skin. Tip damage did not always increaseproportionately with the number of times theneedle was used. There were patients whoseneedles remained in good condition withrepeated use. Therefore, skin type andinjection technique may play roles in thedegree of needle tip damage after use. Inactual practice though, all reuse must bediscouraged, as the damage occurs to such asmall area of the needle tip that it cannot bedetected without a high powered electronmicroscope — even where the needle tip hasbroken off.While reused syringes were not included in thisparticular study, it is reasonable to assume thatthe damage to reused syringe needles is evengreater than the damage to reused pen needlesand lancets, as syringe needles must go thoughthe rubber stopper of syringe vials before eachskin penetration.Photographs showing the type of damage thatcan occur with needle reuse.*a correlation between reuse andlipodystrophy. While “lipos” are notfrequently reported, it is estimated that 2045% of injecting patients with Type 1diabetes mellitus and 3.6% with Type 2diabetes mellitus will have “lipos” (Saez-deIbarra, Gallego 1998) once a search isconducted. These are often easier to feelthan to see and can be disfiguring. Peopleoften prefer to inject into them because itis less painful.Lipodystrophy and ControlA study published at the 1997 InternationalDiabetes Federation (IDF) conference,Helsinki, Finland (Franzen, Ludvigsson, 1997)found that in the study group, versus control,HbA1C decreased with “lipo” decrease. Theaverage decrease was between 7.0 and 7.9% inthe experimental group, versus no change in thecontrol group. In the experimental group, theimprovement in lipohypertrophy and HbA1Ccame about after intensified instructionregarding injection technique (site rotation)and clean needle use while the controlgroup received traditional instruction ininjection technique.FDA GuidelinesUsed needlemagnified 370 timesSame used needlemagnified 2000 times* Photographs from Dieter Look and Kenneth Strauss study:"Nadeln mehrfach verwenden?" Diabetes Journal 1998, 10: S. 31-34.Medical Consequences of Needle Reuse“Reuse of Sharps in Diabetic Patients: Is ItCompletely Safe?” (Look, Strauss 1998)analyzed the three studies conducted by D.Look at the Klinik Hellbachtal in Molln,Germany in 1997 and drew the followingconclusions based on the evidencedemonstrated in the studies.1. Tissue microtrauma: When a deformed needleis used, it lacerates tissue, causingmicrotrauma. This can result in locallysignificant bruising and bleeding. Volunteersin the German studies who reused lancetswere found to have more residual bleeding insites where a more heavily reused lancet wasemployed for the blood letting.2. Embedded needle tips: The studies showedthat excessive reuse ( 7 times/needle) wasoften associated with a breaking off of themicroscopic end of the needle tip. Themedical consequence of embedded metal tipsis unknown at this time.3. Correlation with greater incidence oflipodystrophy: According to the analysis ofthe German studies cited above, local growthfactors may be released and join with insulinto form lumpy nodules called “lipodistrophy.”Although at this time there is not proof thatreuse leads to lipodystrophy (“lipos”), there isRecently there has been a great deal of mediacoverage about the practice of institutionsreusing medical devices that are labeled asbeing for single use. The FDA CompliancePolicy Guidelines Sec. 300.500 (1987) states:“Since disposable devices are not intended bythe manufacturer or distributor for reuse, anyinstitution or practitioner who re-sterilizesand/or reuses a disposable medical devicemust bear full responsibility for its safetyand effectiveness.Insurance ConcernsWhen patients who have been reusing syringesstop reusing, there are bound to be concernsabout whether their insurance will cover theincreased number of syringes that are required.For example, if a patient takes three injectionsper day, and in the past has been using eachsyringe three times, his or her mail order planmay have been sending one box of 100 syringesevery three months. In this case, the plan maybe dispensing one syringe per day, not becausethey expect their members to reuse, but becausethey were never advised that the patient wastaking three injections per day. If a plan doescover syringes, however, it should cover theproper number that will allow the patient to usethem according to the directions. Therefore, ifpatients are not being given enough syringes touse one syringe per injection, they should advisetheir pharmacist or plan of the number ofneedles they need per day. To help avoid theseproblems, prescribers should make it a practiceto indicate the number of needles needed perday on the prescription.
Reuse of Needles White Paper 07D01507001512/20/0612:42 PMMoving ForwardBD, the leading manufacturer of insulin needles,is making a commitment to begin educatingpatients about the risks associated with reuse ofinsulin needles by doing the following:1. A statement advising against reuse will beadded more prominently to syringe, penneedle and lancet boxes and syringe 10-packbags.2. Patient literature including photos from themicroscopy study will be included in syringebox inserts, patient mailings and in literatureavailable to health care professionals fordistribution to patients.3. Slides of the enlarged reused needles will beavailable for use at patient training classes,upon request.4. For pen users, BD will make available a smallpouch on a key-chain that can be used tomake it more convenient to carry needleswhen they are away from home.It is recommended that those training patientsto inject insulin do the following:1. Include a discussion on the risks of needlereuse in their patient training sessions. Patients should be taught to understand thatwhen they dispose of a syringe, pen needleor lancet after one use, they are not beingwasteful, but rather, they are helping reducetheir risk of tissue damage and of havingneedle tips embedded in their skin. Since as a practical matter, patients will notbe able to examine their reused needlesunder a high-powered electron microscope,all patients should be advised to assume thatthey are among the vast majority of patientsin whom the needle tips become hooked orbroken off with repeated use.2. Include the number of needles or lancetsneeded per day on all prescriptions forsyringes, pen needles and lancets and advisepatients not to accept fewer needles orlancets than they need, from their plan.Page 3ReferencesFood & Drug Administration: Compliancepolicy guidelines. Sec. 300.500, Reuse ofMedical Disposable Devices (CPG 7124.16)Washington DC (1997)Franzen I, J. Ludvigsson: Specific InstructionsGave Reduction of Lipomas and ImprovedMetabolic Control in Diabetic Children.Diabetologia Vol 40, Supplement 1: A615(1997)Ginsberg, B.H., J.L. Parkes, C. Sparacino: Thekinetics of insulin administration by insulinpens. Horm. Metab. Res. 26: 584-587 (1994)Hauner H., B. Stockamp, B. Haastert:Prevalence of lipohypertrophy in insulintreated diabetic patients and predisposingfactors. Exp Clin Endocrinol Diabetes 104:106-110 (1996)Look, D, K Strauss: Reuse of sharps in diabeticpatients: is it completely safe? DiabetesJournal 10: 31-34 (1998)Reach G, M. Cahane, M. Vins, et al.: HbA1c inchildren attending summer camps organisedby l’Aide aux Jeunes Diabetiques. Evidencefor a harmful effect of lipohypertrophies inthe early years of diabetes. Diabetes Metab.19: 194-200 (1993)Saez-de Ibarra, L., F. Gallego: Factors related tolipo- hypertrophy in insulin-treated diabeticpatients: role of educational intervention.Practical Diabetes International. 15: 9-11(1998)Wintrobe: Clinical Hematology, Lea & Febiger,9th edition (1993)A Look at the Reuse of Insulin NeedlesThe Early Days of Needle ReuseIn the early days of insulin administration,patients injected insulin using glass syringeswith detachable needles. The users had to boilthe needles between uses and soak them inalcohol to sterilize the needles as best theycould. To make the pain of injections morebearable, users spent hours sharpening theirneedles on a stone between uses to try toreverse the comfort deterioration fromrepeated use.Over the years, manufacturers have madedramatic improvements in the comfort andconvenience of insulin injections. With theintroduction of disposable, single-use insulinsyringes with attached needles, users were freedfrom the arduous tasks of boiling, soaking andsharpening. With the disposable syringes camethinner needles, improvements in the needlepoint geometry and a freshly lubricated needlefor every injection. Therefore, comfort ofinjections improved and the tissue traumaassociated with injections de
needles, and yet many still prefer to reuse insulin needles. Needles Became Even Thinner Since the introduction of disposable insulin syringes, manufacturers have continued to innovate and offer thinner, even more comfortable needles.When the outer diameters of the needles became thinner, the inner diameters (inner lumen, that the insulin .