Transcription
An Approach to TreatingDiabetic Foot UlcersGayle E. Reiber, MPH, PhDVA Career Scientist,VA Puget Sound Health Care SystemProfessor of Epidemiology andHealth Services, University of WashingtonFunding Support from VA Rehabilitation R&D, HSR&D, VISN 20
Acknowledgments Greg Raugi, MD, PhD, Study Co-PIGeoff McCarthy, MD, VISN 20Don Rowberg, MD, Walla WallaCarol Flaugher-Rupe, RN, PA-C, CWOCNRoyalann Evans, RNJennifer Miller, OTR/LSara Uribe
Statement of the Problem The most common causal pathways leading to leg amputation include a foot ulcerOne in six people with diabetes will have a footulcer during their lifetime82,000 US lower limb amputations occurred inpeople with diabetesA majority of amputations could be avoidedif the events leading to the foot ulcer couldbe ameliorated or if the foot ulcer was treatedpromptly and aggressively with “goodwound care”
The VA Situation 5,000,000 patients in the VA system 1,000,000 have diabetes 150,000 will develop a foot ulcer sometime during their lives
Unique VA Diabetic Foot Ulcer andAmputation Patients by SettingFY 2003-2004TertiaryPrimary and CommunityCareSecondaryBasedCenters (66)CareOutreachCenters (91) Clinics (862)Totalnumber ofunique 7
VA Foot Ulcer Care VA ulcer care providers have different backgrounds Use a vast spectrum of therapies, somein place of repetitive, painstaking,routine “good wound care” Busy providers must balancecompeting demands ofacutely ill patients vs.medically and socially complex,time-consuming, foot ulcer patients
Research on VA Foot Care ShowsThere are “Opportunities” for Enhanced provider communicationand coordination Resolution of structural issues:system organization including clinicsand personnel; transportation Electronic documentation (care forfoot ulcers is under-coded andunder-rewarded)
What Do the High-RiskVeterans From 8 VA’s Tell Us? Many can’t see or feel their feet They have not been given enougheducation on foot care They don’t know whom to call / when to call They have un-met foot care needs They are not adequately involved intheir care
Approach to Solving the ProblemSingle interventions targeting a modifiablerisk factor ?No single magic bullet is sufficiently robustto achieve long-term prevention in allpatients in all health care settings This is a complex systemic problemrequiring a complex set ofinterventions
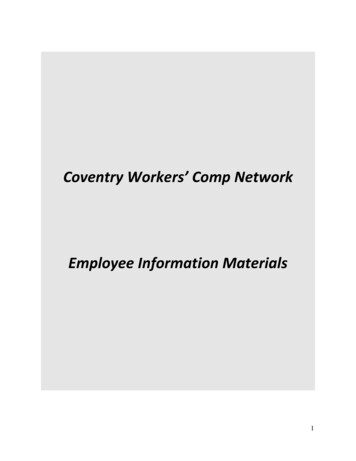
The Chronic Care ModelA roadmap to guide thesolution to complex systemicproblems, address themismatch between needs ofpatients with chronicillness and a caresystem designedfor acute illness.
The Chronic Care Model Applied toFoot Ulcer Care
The Chronic Care Model Applied toFoot Ulcer Care
The Chronic Care Model Applied toFoot Ulcer Care
What Is Good Wound Care?ÎSet of principles that should be applied toevery patient at each encounter Debride callus, devitalized tissue Measure the wound Treat invasive bacterial infection Offload weight Provide moist wound healing environment Provide a global assessment Schedule regular follow-up—continuity of care
Key QuestionsV Will good wound care be delivered anddocumented more frequently in diabeticfoot ulcer patients during the interventionperiod compared to the comparisonperiod?V Will delivering a package of good woundcare to veterans be associated withdecreases in time to healing andincreases in ulcer-free survival?
Key QuestionsV Will delivering a package of good woundcare improve patient, provider, andinstitutional acceptance for organizedfoot ulcer care?V Will a package of good wound care besafe and transportable for a subsequentVA clinical trial of diabetic foot ulcertreatment in non-tertiary care facilities?
Identifying a place in need of adiabetic foot ulcer intervention?.
Walla Walla VAPrimary and Secondary Care VA Medical Center Serves 70,000 veterans; catchment area of 42,000square miles3 CBOC’s 12.5 primary care providers¾ 1 hospitalist¾ 3 PCP have specialty training (one endo, one pulmonary, oneinfectious diseases)¾ No full-time specialists¾ Community podiatrists – contract care 26-bed Skilled Nursing Home
Walla Walla ProjectHypothesis: Delivering a package of goodwound care in a non-tertiary care VA centerwill be feasible, acceptable, and safeTimetableStudy Interval (24 nterventionPeriod; FootUlcer TeamProvidesTreatmentFollow-upPeriod; AnalyzeandDisseminateFindingsTimeInterval:24 months6 months9 months12 months3 months
Foot Ulcer Treatment at WWVA1. Review of administrative data on foot ulcersand amputations180 foot ulcer coded patients in 2003-4Î 125 unique patient recordsÎ 26 had diabetic foot ulcer (diabetes, at least onefoot, and an ulcer at or below the malleoli – 21%)Î 99 did not have a diabetic foot ulcer - decubitusulcer, acute trauma (e.g. punctures, or insect bite),acute arterial insufficiency (e.g. dry gangrenoustoe), surgical wounds or the result of vasculitis,pyoderma gangrenosum, gout (79%)
Good Wound Care DeliveryWalla Walla 2003-41st visitN 26f/u visitsN 81Glycemic control documented35%n/aHbA1c reported42%n/aPeripheral circulation documented46%n/aSensory exam documented27%n/aAnatomic abnormalities documented15%n/aDebridement performed4%16%Wound measurements (l x w)recorded23%21%Global assessment recordedn/a41%Statement of infection (or not)73%75%Offloading strategy documented35%35%Moist wound healing prescribed19%35%Element of GWC
2) Assessed institutional interest level(administration and providers)Î Interviews with key Walla Walla VA andcommunity providersÎ Surveyed providers, 77% responded;identified a need for organized wound careÎ CMO identified personnel for wound careteam
3) Wrote, negotiated, and signed a cooperativeagreement with the site PI (CMO)9999We agreed to purpose, time frameWalla Walla leadership selected peopleWe train and monitor teamWe both provide resources (as did VISN20)9 We provide clinical back-up9 We provide Foot Ulcer CPRS template
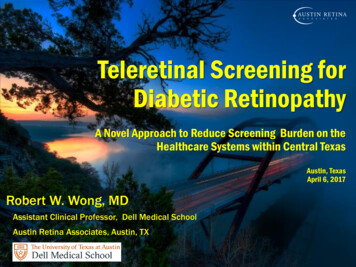
Core Organization and FlowTele-consultationPatient withFoot UlcerTreatment inWound ClinicPrimaryCare
The Walla Walla Model
Start-up Period Victories Training team members PA - Carol Flaugher-Rupe RN - Royalann Evans PCC - Sara Uribe Offloading therapist - Jennifer Miller Organizing a NEW Clinic; scheduling system Pharmaceutical and dressing formulary Same day, on site off-loading or footwear Coordination with Primary Care, CBOC’s,Community Podiatrists, Tertiary Care Centers –developed care pathways Tele-wound consults, weekly phone card roundsand 24/7 back-up Continuing foot education bimonthly w/community
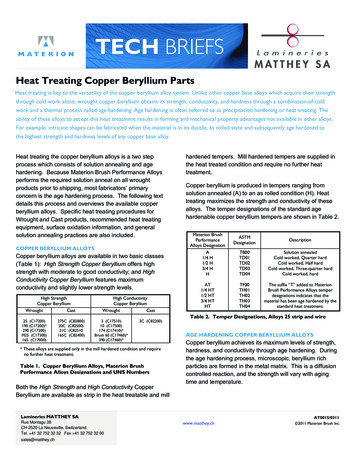
Chart Note Template
Making the Clinical InformationSystem Work Notebook computers with stylus Foot ulcer data collection template built into CPRS Automatically gathers information from prior encounters and “feed forward” to today’s visitBased on principles of “good wound care” thuscollects and integrates the proper dataPrevents important deletions .Allows oversight by off-site experts/casemanagers; pictures, x-rays, images sharedStreamlines ordering, justifies coding, anddocumentationFacilitates communication with PCPs
Start-up Period FindingsDistribution of Wound Diagnoses 88 unique veterans in 8 months28% diabetic foot ulcersIndividualized patient problem solving based onbaseline diabetes surveyPatient Satisfaction - veterans mail Seattle a1 page satisfaction survey after each visit –uniformly describe care as “excellent”Needed full 9 months to prepare intervention
The FutureVISN 20 Network of Wound CareVA Puget Sound - MagnetProviders interested and willing to work together CPRS templates by type of woundComputer experts (CAC) develop with cliniciansTraining and retraining on evidence based infoWound care procedure manualsFormularies for wound care medications andproducts Wound care providers highly valued, supported!
VISN 20What are the VISN 20 Wound Problems?% DiabetesFoot ulcers47Venous ulcers55Arterial ulcers46Pressure ulcers28Minor amputations83Major amputations72Total N3,1401,7947331,28110895
Who is Next?9 Seattle/American Lake9 Roseburg– Eugene CBOC
Summary and Conclusions Excellent scientific evidence supports good wound care elementsGood Wound Care is not difficult—it isrepetitive, physically demanding, patientcentered and time-consumingIt is all about the details (organization,personnel, CPRS)We hope to decrease the “Double Troublein Walla Walla ” by the end of theintervention!
26-bed Skilled Nursing Home. Walla Walla Project Hypothesis: Delivering a package of good wound care in a non-tertiary care VA center will be feasible, acceptable, and safe Study . Element of GWC 1stst visitvisit N 26 f/u visits N 81 Glycemic control documented 35% n/a HbA 1c reported 42% n/a Peripheral circulation documented 46% n/a