Transcription
NorthEasternHealthBoardBordSláintean OirThuaiscirtNorth Eastern Health BoardWound Management GuidelinesTreoirlínte ar Bhainistíocht Créachta20042004Bord Sláinte an Oir Thuaiscirt“We will develop policy,procedures and protocolsto guide decision-makingand service delivery”'Déanfaimid forbairt ar pholasaí,modhanna oibre agus prótacalchun cinnteoireacht agus solátharseirbhísí a threorú'.A Health Strategy for the People of the North-East, 2003, Action 4.4Straitéis Sláinte do Phobail an Oir Thuaiscirt, 2003, Gníomh 4.4
NEHBGuidelines for WoundManagementC l i n i c a l P ra c t i c e A re a s : Principles of Wound ManagementPressure Ulcer PreventionLeg Ulcer ManagementThe Management of the Diabetic FootC o m p i l e d a n d R e s e a rc h e d b y :The North Eastern Health Board (N.E.H.B.) Regional Wound Management Committee.PolicyWound Management GuidelinesVersion No.1Date of Authorisation9th August 2004Date of implementation17th December 2004Review DateJanuary 2006Reviewed By:DateApproved By:Date
Wound Care Policy - NEHBIt is the policy of the North Eastern Health Board that all decisions and actions pertaining towound care be based on current best practice.Information with regard to best practice is contained within the four documents listed below.The Principles of Wound Management, Guidelines for Practice is the guiding document,supported by the three specific documents, Pressure Sore Prevention, Leg Ulcer Managementand Management of The Diabetic Foot. These guidelines will be reviewed and updated on anannual basis. The review will include and take on board the views of practitioners.In developing this policy the Board is cognisant of the professional responsibility on allclinicians involved in wound care to keep themselves up-to-date with clinical practice and totake all necessary steps to maintain their competence.Guidelines documents include: A decision making algorithm Principles of Wound Management, Guidelines for Practice. Pressure Sore Prevention Leg Ulcer Management Management of the Diabetic Foot
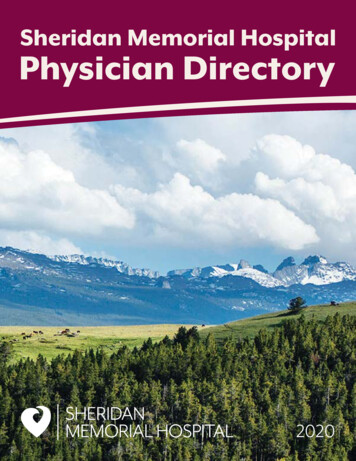
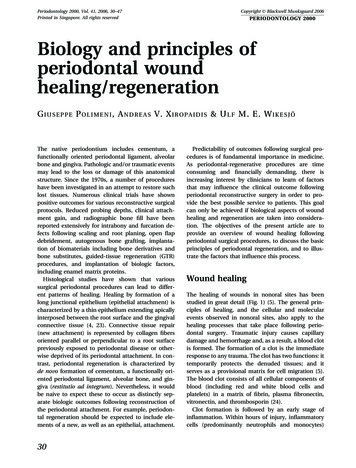
HospitalDoctorDietician Podiatrist/ Occupational Specialist TissueOrthotist TherapistConsultant ViabilityNurseRefer as Appropriate to Specialised AreaHolistic tyGPIn Partnership WithNursing Intervention in line withThe Scope of Nursing &Midwifery Practice(An Bord Altranais 2000)PhysiotherapistLeg UlcerManagementGuidelines/PathwayEarly ReferralToSpecialist CareCONTINUOUSREASSESSMENTPressure SorePreventionGuidelines /PathwayNEHBWound Care GuidelinesPrinciples of WoundManagementWOUND CARE MANAGEMENT PATHWAYDiabetic FootManagementGuidelines &Pathway
NORTH EASTERN HEALTH BOARDPRINCIPLES OF WOUND MANAGEMENTGUIDELINES FOR PRACTICE
TABLE OF CONTENTSF o re w o rd11 . P h y s i o l o g y o f Wo u n d H e a l i n g22 . F a c t o r s w h i c h A f f e c t Wo u n d H e a l i n g3Intrinsic and Extrinsic Factors2.1 Moist Wound Healing2.2 Wound Temperature2.3 Excess Wound Exudate2.4 Necrotic and Sloughy Tissue2.5 Oxygenation2.6 Protection of Wound2.7 General Pathophysiological Factors3 . Wo u n d A s s e s s m e n t3.13.23.33.43.53.63.7Site of WoundWound MeasurementSurrounding SkinWound BedExudateWound OdourWound Pain33344444555556664 . Wo u n d B e d C l a s s i f i c a t i o n75 . Wo u n d C l e a n s i n g9Key Points5.1 Cleaning Chronic Wounds5.2 Cleaning Traumatic Contaminated Wounds5.3 Surgical Wounds999106. Hand Hygiene117 . A s e p t i c Te c h n i q u e128 . Wo u n d M a n a g e m e n t P ro d u c t s148.1 Characteristics of the Ideal Wound Dressing8.2 Selecting a Suitable Dressing14159 . Wo u n d M a n a g e m e n t O b j e c t i v e s169.1 Necrotic wounds9.2 Sloughy Wounds9.3 Granulating Wounds9.4 Epithelialising Wounds9.5 Management of the Infected Wound9.6 Management of Wounds colonised with MRSA161617171719
10 .T h e R o l e o f N u t r i t i o n i n Wo u n d M a n a g e m e n t20Key Points10.1 Nutritional Assessment10.2 Nourish Scoring Chart10.3 Nutritional Requirements10.4 The Dieticians Role2122232425A p p e n d i x I - Wo u n d A s s e s s m e n t C h a r t s26A p p e n d i x I I - Formulary of Wound Management Products32Absorbent DressingsLow Adherent DressingsNon Adherent DressingsVapour Permeable DressingsHydrogel DressingsHydrocolloid DressingsHydrofibre DressingsAlginate DressingsPolyurethene Foam DressingsOdour Absorbing DressingsTulle DressingsEnzymatic AgentsAntibacterial AgentsVacuum Assisted pendix III - Principles Audit Sheet45A p p e n d i x I V - Wo u n d c a re M a n a g e m e n t S u b - C o m m i t t e eMembers46A p p e n d i x V - Pe r s o n n e l C o n s u l t e d W i t h D u r i n g T h eD e v e l o p m e n t P ro c e s s47A p p e n d i x V I - Pe r s o n n e l C o n s u l t e d f o r R a t i f i c a t i o n47Glossary48R e f e re n c e s49DisclaimerAny reference to specific products within theseguidelines is by way of an example only. It shouldnot be considered to constitute any form ofrecommendation or endorsement by the NorthE a s t e r n H e a l t h B o a r d.
FOREWORDThese comprehensive wound management guidelines reflect the current research and evidence based practice. They offera structured approach to the assessment, prevention and management of patients with wounds. They are designed tohelp healthcare practitioners both in the primary and secondary care setting, base their clinical decisions on the bestguidance available, so that they may optimise outcomes for both clients and the health service. By integrating ourapproach to care planning for individuals, and by basing our decisions on best available evidence, we will be offering acontinuum of quality care as proposed by our current health strategy ( Dept. of Health and Children 2001).These guidelines have been developed by healthcare professionals clinically involved in wound management and havebeen submitted to a multidisciplinary group of individuals for expert review (see appendix V). Sources of evidence thathave been accessed during the development of these guidelines include: Medline, Cochrane, CINAHL and the RoyalCollege of Nursing databases and information from other organizations such as the European Pressure Ulcer AdvisoryPanel, the International Leg Ulcer Advisory Board and the National Institute for Clinical Excellence ( NICE) in the UnitedKingdom. The North Eastern Health Board "Regional Woundcare Management Committee" wishes to acknowledge theClinical Resource Efficiency Support Team (CREST) in Northern Ireland, Our Lady of Lourdes Hospital, Drogheda, andCommunity Care Area 7, Dublin, whose respective publications "Guidelines on the Principles of Caring for Patients withWounds","Wound Management:Guidelines for Practice", and “Guidelines for Leg Ulcer Management" proved invaluable inthe compilation of these guidelines.Paul RobinsonChief Executive OfficerRéamhráSna treoirlínte cuimsitheach seo ar bhainistíocht créachta, tá na cleachtais is nua aimsire, atá bunaithe ar thaighdeagus fianaise an chleachtais. Tugann siad bealach céimnithe dúinn ar mheasúnú, ar sheachaint agus bainistíocht othaira bhfuil créachta orthu. Forbraíodh iad chun cabhair a thabhairt do chúramóirí sláinte i réimsí an phríomh agus an daraleibhéil chúraim, agus go mbeidh a gcinní cliniciúla bunaithe ar an treoir is fearr atá ann, chun an toradh is fearr a fháildon othar agus don tseirbhís sláinte. Mar chomhtháthú ar phleanáil an chúraim do dhaoine aonair agus ár gcinní abhunú ar an bhfianaise is fearr atá againn, soláthróidh muid cúram caighdeánach atá leanúnach, mar atá molta in árstraitéis sláinte reatha (Roinn Sláinte agus Páistí 2001).Tá na treoirlínte seo forbartha ag cúramóirí sláinte proifisiúnta a bhfuil baint cliniciúil acu le bainistíocht créachta.Cuireadh na treoirlínte faoi bhráid grúpa ildisciplíneach i gcomhair athbhreithniú shaineolach (féach aguisín V). Le linnforbairt na dtreoirlínte seo baineadh úsáid as na foinsí eolais seo a leanas: Medline, Cochrane, CINAHL agus dátabhunúsCholáiste Ríoga Altranais chomh maith le faisnéis ó eagraíochtaí eile: An Phainéil Comhairleach Eorpach arBhrú-Othrais (EPUAE), Bord Comhairleach Idirnáisiúnta ar Othrais na gCos agus Institiúid Náisiúnta um FeabhsúchánCliniciúil san Ríocht Aontaithe (NICE). Is mian le Coiste Réigiúnda Bainistíochta Chúram Chréachta de chuid Bord Sláintean Oir Thuaiscirt aitheantas a thabhairt don Fhoireann Tacaíochta Feidhmiúlachta ar Aiseanna Cliniciúla de chuidTuaiscirt Éirinn (CREST), Ospidéal Mhuire Lourdes, Droichead Átha, agus Ceantar Chúram Phobail 7, Baile Átha Cliath asucht an t-eolas fíorluachmhar chun na treoirlínte seo a scríobh a bhí ar fáil ina a gcuid foilseacháin -"Guidelines on thePrinciples of Caring for Patients with Wounds", "Wound Management: Guidelines for Practice", agus " Guidelines for LegUlcer Management".Paul RobinsonPríomhfheidhmeannach1
1PHYSIOLOGY OF WOUNDHEALINGThe physiological response of tissue to injury can be divided into three distinct, overlapping phasesInflammatory PhaseProliferative PhaseMaturation or Remodelling PhaseInflammatory Phase ( 0 -3 days)This phase begins with the process of haemostasis. This is achieved following reflex constriction of the damaged bloodvessel wall. Platelets and fibrin plug the bleeding vessel causing clot formation. Damaged tissue releases histamine andother mediators which cause vasodilatation of the surrounding intact blood vessels and increases the blood supply to thearea. The capillary walls become more permeable and allow serum, leucocytes, antibodies and some red cells to infiltratethe surrounding tissues. Polymorphonuclear leucocytes and macrophages migrate out of the capillaries into the damagedarea. These local responses give rise to signs of inflammation - heat, redness, oedema, swelling and pain.This phase prepares the wound bed for healing by removing necrotic and foreign material. Polymorphs engulf and destroybacteria. Macrophages clear the wound of debris, foreign material, devitalised tissue and excess fibrin. They alsostimulate the formation of fibroblasts which synthesise the structural protein collagen.P ro l i f e ra t i v e P h a s e( 3 - 24 days)Fibroblasts lay down ground substance and collagen fibres. New blood vessels infiltrate the wound. Capillaries areformed by endothelial budding, a process called angiogenesis. Granulation tissue begins to form which is pinkish / red incolour. Vitamin C is essential for collagen synthesis. Without it, collagen synthesis ceases, the unsupported new bloodcapillaries breakdown, bleed and wound healing ceases. Epithelial cells, at the wound margins, surrounding hair follicles,sebaceous glands and sweat glands, divide and begin to migrate over the newly formed granulation tissue. When cellsmeet, either in the centre of the wound forming islets of cells, or at the margin, they stop.M a t u ra t i o n P h a s e( 24 days - 1 year)This phase involves wound contraction and re-organisation of connective tissue. Cross-linking of collagen fibres occur,contracting the wound and increasing the wound's tensile strength.In reality, the phases of wound healing overlap and the duration of each phase and the time required to complete healingdepends on many factors including the size and site of the wound, the patient’s general physiological condition and manyother intrinsic and extrinsic factors (Morison 1992).2
2FACTORS WHICH AFFECT WOUNDHEALINGMany factors can affect wound healing. They may be intrinsic (patient related) or extrinsic.INTRINSICEXTRINSICAdverse Conditions at Wound SiteAdverse Effects of Other TherapiesDehydration or local oedemaFall in wound temperatureExcess exudateWound infectionRecurrent traumaHypoxia or hyperoxia depending onthe stage of wound healing.Presence of necrotic or sloughy tissueChemotherapy, Radiation,Steroid TreatmentGeneral Pathophysiological FactorsInappropriate Wound ManagementCardiovascular disordersEndocrine and metabolic disordersRespiratory DisordersDecreased resistance to infectionAnaemiaMalnutritionNormal Ageing ProcessSmokingPsychosocial factors, stress, anxiety, dehydrationInaccurate wound assessmentImproper use of topical agents and dressingsCareless surgical and dressing techniquesNegative attitudes of staff(Morison 1992 ; Miller and Dyson 1996).It is important to remember that wound healing is not always possible. In these situations care must be directed towardsthe individuals physical and psychological comfort.2.1 MOIST WOUND HEALINGWinter (1962) found that wounds covered with an occlusive dressing, which maintained a moist environment at thewound / dressing interface, epithelialised almost twice as quickly as wounds exposed to air and allowed to scab. Hededuced that, in dry wounds new epithelial cells were impeded from migrating across the wound by collagen fibres whichconnected the wound scab to the underlying dermis. In moist wounds the epithelial cells migrated more quickly becausethey did not have to break through the scab or the fibrous tissue underneath in order to cross the wound surface. Moistwounds move through the inflammatory phase of wound healing more quickly than dry wounds (Dyson et al 1988), theyare less painful with more collagen production and better contraction, resulting in less scarring (CREST 1998).2 . 2 W O U N D T E M P E R AT U R EThe optimum wound temperature necessary to promote healing is 37 degrees Centigrade. Exposure of the woundcontributes to drying at the wound surface and a drop in temperature. As the wound temperature drops, mitotic activityslows down and leucocyte activity and oxyhaemoglobin disassociation are severely disturbed. Wounds take 40 minutes toregain their original temperature and 3 hours for mitotic activity to return to normal after wound cleansing (Miller 1994).3
2 . 3 E X C E S S W O U N D E X U D AT EWounds produce a fluid known as exudate. It bathes the wound continuously, keeps it moist, supplies nutrients andprovides optimum conditions for the migration and mitosis of epithelial cells. It has antimicrobial properties, containsepidermal growth factors and is rich in leucocytes which help control bacteria in the wound (Leaper, Brennan andSimpson 1984). Although the wound dressing / interface should be moist, it must not be saturated. Excessive moisturecauses maceration and excoriation of the surrounding skin which may predispose to infection.2 . 4 N E C R OT I C A N D S L O U G H Y T I S S U EThe presence of necrotic tissue, excess slough and foreign bodies such as sutures and drains delay healing and increasethe risk of clinical infection developing. The inflammatory phase is prolonged preventing granulation andepithelialisation. Necrotic tissue must be removed surgically, enzymatically or with products such as hydrogels orhydrocolloids which encourage autolysis.N.B. The general condition of the patient must be carefully assessed by a competent practitioner before debridemente.g. Heels.2 . 5 O X Y G E N AT I O NIf factors essential to healing such as oxygen, amino acids, vitamins and minerals are slow to reach a wound because ofimpaired vasculature, healing is delayed. In the early stages of wound healing tissue oxygen is extremely low ( 10mmHg) indicating the absence of a working micro-circulation. A low oxygen tension is thought to stimulate fibroblastreplication and angiogenesis which encourages the production of granulation tissue. This helps improve the circulationand raises the level of oxygen in the tissues. When the tissue oxygen is greater than 10mm Hg collagen synthesis occursand healing continues.2 . 6 P R OT E C T I O N O F W O U N D F R O M I N F E C T I O N A N DTRAUMAProtection of the wound from invading pathogens is essential. Wound infection can delay healing and if uncontrolled maylead to cellulitis, bacteraemia and septicaemia. The majority of modern dressings are bacteria proof whereas paraffintulle, gauze and dry dressings are not. No dressing is bacteria proof when *strike through* occurs. Wounds must also beprotected from toxic agents such as antiseptic solutions or cotton wool fibres. Mechanical trauma may damage highlyvascular granulation tissue and newly formed epithelial tissue. Traditional dressings such as gauze and paraffin tulleadhere to the wound surface. Granulation tissue grows between the mesh in the paraffin tulle, and when the dressing isremoved, the granulation tissue is torn, resulting in destruction of new blood vessels and bleeding. Bleeding is a sign oftrauma.*Strike Through * : Where exudate soaks through a dressing and is visible on its outer surface.2 . 7 G E N E R A L PAT H O P H Y S I O L O G I C A L F A C TO R SA number of medical conditions are associated with poor wound healing. These include cardiovascular disease, diabetesmellitus, rheumatoid arthritis, anaemia and malnutrition. The mechanisms by which these diseases affect tissue repairare often complex, but may delay healing by reducing the availability at the wound site, of substances necessary forhealing.The creation of an ideal wound environment will accelerate healing. This environment is moist, untraumatised, warm, freefrom devitalised tissue and excess exudate, protected from pathogens and foreign particles, slightly acidic and hypoxic orhyperoxic depending on the phase of wound healing. The selection of a suitable dressing which meets these criteria willenhance and encourage wound healing.4
3WOUND ASSESSMENTThe systematic assessment of a wound is essential as it provides baseline data on which to evaluate healing and theefficacy of the treatment regime.Assessment and evaluation should be carried out at regularly stated intervals and the process clearly documented on aWound Assessment Chart. (Examples are given in Appendix I). Assessment is not a once off process, rather it is an ongoing, cyclical process. Initial wound assessment must be undertaken by a registered nurse. Subsequent assessmentsmay be done by a student nurse under the supervision of a registered nurse.3 . 1 S i t e o f Wo u n dIt is important to record the site of the wound for the following reasons: accurate record keeping helps differentiate between wounds the position of a wound may suggest its pathology, for example, venous leg ulcers tend to occur in the gaiter area,whilst ulcers on the foot are usually due to ischaemia or diabetes.3 . 2 Wo u n d M e a s u re m e n tThe accurate measurement of the physical size of a wound is vital for assessing the progress of healing. Although thereare many different ways of measuring wounds the most simple and accessible methods include:(i)ruler based assessment, e.g., width x depth x breath (maximum)(ii)transparency tracings,(iii)photography / Grid Camera.Cavity wounds should be gently probed (with a sterile swab stick) to establish the extent of undermining and / or thedepth of hidden tracts. Caution should be exercised where the wound overlies sensitive structures e.g. bowel.Measurement should be recorded in millimeters or centimeters. Weekly - to monthly measurements are usually sufficient.Note: In some instances a sinogram or x-ray will be required to establish the full extent of the wound.3 . 3 S u r ro u n d i n g S k i nThe condition of the skin surrounding the wound provides important information about underlying disease and theeffectiveness of current treatment regimes. For example, pink tissue on the wound margins may indicate epithelialisation,cool, shiny, hairless skin on the lower leg may indicate arterial disease and maceration may indicate an ineffectivedressing regime. A rolled (lipped) edge may indicate malignancy or another aetiology and may require biopsy. Documentthe skin colour, hardness, induration, dermatitis, the presence of oedema or any other abnormality.3 . 4 Wo u n d B e dThe appearance of the wound bed is said to indicate both the stage of healing and the health of the wound. The woundbed must be thoroughly assessed, as tissue type often provides the rationale behind the main treatment objective.One of the most effective ways to describe tissue type is by its colour. In general:Necrotic black or black / brownleathery textureSloughy yellow or yellow / whiteliquid or fibrous textureGranulating pinkish / redgranular textureEpithelialising pale pinkThe type of tissue on the wound bed can be further quantified through percentages, e.g. 50% red / granulation tissue 50 % yellow / slough.5
3.5 ExudateA knowledge of the level and type of wound exudate is extremely important, as it, in conjunction with the type of tissue onthe wound bed, will influence dressing choice. Wound exudate may be described as:S e ro u sSanguinousS e ro s a n g u i n o u sPurulentClear fluid with apparent visual absence of blood, pus or other debris.Bloody, appearing to be composed entirely of blood.Blood mixed with obvious quantities of clear fluid.Pus like in appearance, cloudy and viscous.It is very difficult to devise an accurate method of describing the level / amount of wound exudate.DryLowM o d e ra t eHighThe wound does not produce exudate.The wound bed is moist, i.e. there is scant or small amounts of exudate.The surrounding skin is wet and there is exudate in the wound bed.The surrounding skin is saturated (sometimes macerated) and the wound is bathed in fluid.Note: The dressing regime may add to or detract from the true level of wound exudate.3 . 6 Wo u n d O d o u rMalodour may cause the patient to suffer social or psychological isolation. It can also cause physical symptoms such asnausea and vomiting resulting in severe nutritional deficits. Wound odour may be caused by a heavy bacterial burden,infection, necrotic tissue or the use of certain dressing materials. The cause must be established and where possiblerectified, e.g. treat infection, remove necrotic matter or change dressing regime.Odour is very subjective and difficult to quantify. However, the following descriptive terms may be useful: none smell only noticeable on dressing removal and disappears when the dressing is discarded smell fills the room.3 . 7 Wo u n d Pa i nAlthough pain is subjective, its location, frequency and severity can be helpful in determining the presence of underlyingdisease, the exposure of nerve endings, the efficacy of local wound care and psychological need. Visual or verbal ratingscales can help patients to communicate the level of pain which they are experiencing. Local pain management policiesshould be implemented to ascertain the site, frequency and severity of pain experienced by the patient.S i t e o f Pa i nF re q u e n c ySeverity6Does the patient complain of pain at the wound site or in the surrounding areas. Does thepatient complain of pain elsewhere in his / her body.Ascertain the frequency of pain, e.g. none, at dressing change, intermittent, or continuous.Ask the patient how severe the pain is and where he / she would rate it on a scale of 1 -10.Identify the amount and type of analgesia required to alleviate it.
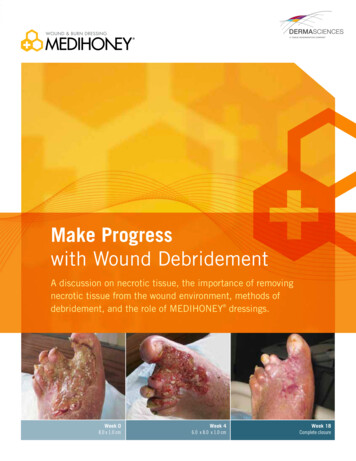
4WOUND BED CLASSIFICATIONSeveral categories of tissue may be observed in a wound. For information on the treatment of each type of woundtissue, please refer to Section 9 - Wound Management Objectives.T i s s u e Ty p eNecrotic Tissue [Black]Necrotic tissue is the result of tissue death secondary to ischaemia. It is usually black or black/brown incolour and hard, dry and leathery in texture.Sloughy Tissue [Yellow]Slough consists of dead cells and is yellow or yellow/white in colour. It may be liquid or fibrous in natureand can appear in increasing amounts in chronic or infected wounds.7
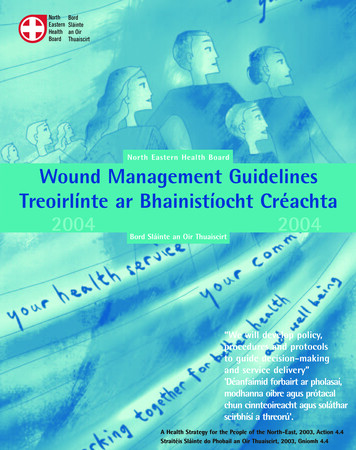
T i s s u e Ty p eGranulation Tissue [Pinkish / Red]Granulation tissue is a highly cellular, transient tissue, rich in macrophages and fibroblasts. Itsextracellular matrix is composed of collagen, hyaluronic acid and fibronectin and it contains a network ofnewly formed blood vessels. It is normally pinkish / red in colour and granular in appearance.Epithelialising Tissue[Pink]Epithelialising tissue is the new layer of epidermis that eventually covers granulation tissue. The first partof re-epithelialisation is the migration of epithelial cells across the wound surface. Following this, abasement membrane is laid down under the new epithelial covering. Epithelial tissue is pink in appearance.In large wounds, it may appear in isolated clusters or inlets within the wound.Overgranulating / Hypertrophic Tissue[Pinkish / Red]Overgranulation is an exuberant overgrowth of granulation tissue which stands proud or is raised above thesurface of the wound. It may be uniformly raised or be present in patches. It prevents epithelialisation.(Miller and Dyson 1996 , Morison et al 1997).8
5WOUND CLEANSINGWounds which are clean and those with light to moderate exudate with healthy granulation tissue do not requirecleansing.Cleaning may traumatise granulation tissue, reduce the surface temperature of the wound, remove exudate that hasbactericidal properties (Holn et al 1977) and other substances necessary for wound healing e.g. growth factors. However,wounds which contain debris, foreign bodies, devitalised soft tissue, slough or necrotic tissue should be cleaned. Suchmaterial may support the growth of pathogenic micro-organisms.Ke y Po i n t s If cleansing is indicated, the wound should be irrigated gently using normal saline (Bale and Jones 1997), chronicwounds such as leg ulcers can be cleansed using tap water (Lawrence 1991). Swabbing can result in the breakdown offragile granulation / epithelialising tissue, and does not reduce the number of bacteria on the wound surface butmerely redistributes them (Thomlinson 1987). Non-filamented gauze may be used to clean and dry the skinsurrounding a wound. Physiological saline (sodium chloride 0.9%) is the solution suitable for cleansing all woundtypes (Bale and Jones 1997). Studies indicate that saline and water should be warmed to body temperature (370C) - cold solutions slow downcellular repair. However, many practitioners will find it difficult to achieve this temperature in the practice setting.Therefore, it is recommended that cleansing solutions are kept at a minimum of room temperature. Antiseptics are limited in their effectiveness and are potentially harmful when used to clean granulating wounds(Morison 1992). If an antiseptic is required, one must balance its effectiveness as a bactericidal or bacteriostaticagent against the likely degree of damage it may cause to granulation tissue. Agents which have been reported asbeing harmful to granulation tissue include :Iodine compoundsChlorhexidineHydrogen PeroxideCetrimideHypochlorites such as Eusol and Milton5 . 1 C l e a n i n g C h ro n i c Wo u n d sAn aseptic technique is not always indicated. If possible, immerse the affected wound (e.g. leg ulcer) in a deep bucketlined with a plastic bag, with luke warm tap water. Soak for 10 minutes only. Open wounds have a tendency to absorbwater, which may increase the amount of exudate produced over subsequent days necessitating more frequent dressingchange (Morison et al 1997). Gently pat the skin dry with a clean towel or paper towels. Wash the bucket, rinse well andstore dry.5 . 2 C l e a n i n g Tra u m a t i c C o n t a m i n a t e d Wo u n d sTraumatic wounds may be contaminated by a variety of materials including dirt, oil, foreign bodies or bacteria. This typeof injury requires thorough cleansing and debridement and should be undertaken as soon as possible. This is bestachieved with large volumes of saline or tap water. Where tissue is heavily contaminated or is devitalised, surgicalcleansing and removal of debris is the treatment of choice.9
For minor traumatic wounds, asepsis is unnecessary until all gross contamination has been removed (Morison et al1997). Immerse the injured area in warm tap water or normal saline. This eases the pain and helps loosen debris. If anantiseptic solution is indicated, Hibitaine or Povidine Iodine may be used.5 . 3 S u rg i c a l Wo u n d s1. Protect with a sterile dressing for 24-48 hrs post operatively an incision that has been closed primarily (CDC 1999). Donot disturb the wound dressing for 48 hours following surgery. Micro-organisms may enter the wound from adjacentskin until such time as the wound surface has healed.2. In the immediate post operative period, dressings which become saturated with excessive drainage may be reinforcedtemporarily. These dressings must be changed as soon as possible.3. If the wound continues to leak after 48 hours, an absorbent dressing may be used to contain the exudate. Strictaseptic technique is required to prevent endogenous and exogenous infection and the possibility of cross infection.4. Surgical wounds After 24-48 hours if the wound is dry and there are no drains in situ in the wound then the dressingmay be removed and the wound left exposed or as instructed by the surgeon. The patient may shower or bathe ifdesired. If the patient would like the wound covered, a vapour permeable film dressing or non adherent dressing maybe used.Orthopaedic wounds Dressings changed as necessary until after removal of suture/clips, or until the wound iscompletely healed. Patient advised not to bathe or shower until the wound is fully healed, or as instructed by theorthopaedic surgeon.10
6Hand HygieneFor infection to spread there must be a source of infecting organism, a means or route of transmission and a susceptible host. Aclear idea of the route of transmission of organisms will allow simple and sensible precautions to be taken to prevent its spread.Direct contact via the hands of healthcare workers is the most common route of spread of organisms responsible forcross-infection in hospitals. This method will effectively transmit staphylococci and coliform organisms between patientsand may be responsible for transmitting some enteric or respiratory pathogens.Other modes of infection are indirect, i.e., airborne, inoculation, sexual route, vector borne, or food borne.W h e n t o Wa s h Yo u
College of Nursing databases and information from other organizations such as the European Pressure Ulcer Advisory Panel, the International Leg Ulcer Advisory Board and the National Institute for Clinical Excellence ( NICE) in the United Kingdom. The North Eastern Health Board "Regional Woundcare Management Committee" wishes to acknowledge the