Transcription
Pain, Prejudice and Opioids: EmergingPolicy and Integrative PracticeIntegrative Healthcare SymposiumFebruary 23, 2016John WeeksJane Ballantyne, MDHeather Tick, MD
Objectives: Participants Will Be Able To. Discuss the level of inclusion of nonpharmacologic approaches in emerging painpolicyEvaluate the role of interprofessionalismand being at the table on the creation ofpolicy directionsDiscuss the level of risk with nonpharmacologic approaches to pain.Explore the necessity for policy andpractice changes regarding the role ofopioids in the management of chronic painDisclosure: I have no conflicts of interest. I do have multiple alignments of interest, volunteer roles and limitedconsulting with not-for-profit organizations on pain related issues.
Opioid/Pain PolicyThe Awakening to Non-Pharmacologicand Integrative Approaches
Early Opioid Guidance 2011Center withsignificant CAMresearch – butno reference toCAMin guideline.Why?Dan Cherkin, PhD
Is it possible that acharacteristic of areductive mindis that it can’taccess commonsense?
Relieving Pain in America 2011 - IOM IOM Committee on Advancing PainResearch, Education and Care–– ND, LAc pain expert MarinelliUCLA Integrative pediatrician Zelzer“CAM” included in 15 relevantsegments–Re cost-effective, education, under barriers,self-management, interdisciplinary teams, Rick Marinelli, ND, LAcreimbursement, etc.http://theintegratorblog.com/index.php?option com content&task view&id 759&Itemid 93 Antecedent to the National PainStrategyPain focus in NCCAM Strategic PlanHighlighted in Strategic Objective #1Lonnie Zelzer, MD
Joint Commission - November 2014
CDC’s OpioidGuidance
DRAFT CDC Guideline: Were Integrative Healthand CAM Professionals on the Team? Stakeholder Review Group had norepresentatives National Center for InjuryPrevention and Control’s Boardof Scientific Counselors had noapparent representation
DRAFT Guideline: CDC “Non-Pharmacologic”MethodsDecember 2015“Nonpharmacologic therapy andnonopioid pharmacologic therapy arepreferred for chronic pain.DRAFT: explicitly included as nonpharma:“ complementary and alternativetherapies (e.g., manipulation, massage,and acupuncture ) “What happened with the draft?
CDC Comment PeriodMultiple integrative healthorganizations respondPublicized and promoted response
FINAL CDC Description of “Non-Pharmacologic”Methods“Nonpharmacologic therapy and nonopioidpharmacologic therapy are preferred forchronic pain.”FINAL: Explicit Options for Non-Pharma:“Exercise, aquatic, aerobic, psychological,cognitive behavioral therapy, andbio-psycho-social interventions”RECALL DRAFT: Also explicitly included:“ complementary and alternative therapies (e.g., manipulation,massage, and acupuncture ) “What happened with the draft?
Integrative Health and Medicine Representatives on Teams? Oversight Panel: No experts fromIHM/CAM 6 Working Groups (80 total members) Working Group on Prevention and Care: None Working Group on Disparities: None Working Group on Service Delivery and Payment:None Working Group on Professional Educationand Training:one, Brian Berman, MD Working Group Public Education &Communication: NoneBrian Berman,MD
CAM/IHM Inclusionas “Collaborators”Vision Statement: 8th of 14 bullets, under education, at the end of list of prioritized areas:“the role of complementary and integrative medicine.”Listed among “Collaborators”-Service Delivery & Payment Objective #1: “Define and evaluate integrated, multimodaland interdisciplinary care .” urged inclusion of “licensed integrative health practitioners.”-Same section, Objective #3,: “Tailor payment to promote and incentivize high-quality,coordinated pain care .” reaches out to “licensed integrative health care providers.”-Disparities, Objective #1: “Reduce bias (implicit, conscious, and unconscious) and itsimpact on pain treatment by improving understanding .” calls out to include “socialservice providers (including licensed practitioners who provide integrative andcomplementary health approaches).”-Prevention and Care, Objective #2: “Develop nationwide pain self-managementprograms.” invites collaboration with “licensed complementary and integrative healthfields.”
Obama and Congressional Opioid Plans(2016) Obama strategy: IHM absent Congressional plan: IHM absentThe Uneven Entrance of Non-Pharma Approachesas Tools in the Opioid ols-in-the-opioidcrisis
Leadership: Get into the Opioid Conversation! American Public Health Associationresolution– Nursing section backed– Support from Chiropractic Section andIntegrative, Complementary andTraditional Health Practices Section Foundation for ChiropracticProgress(F4CP) white paper AANP reaches out to AMA as resource IHPC Task Force – planning 2017 actionMichele Maiers, DC, PhDAPHA Chiropractic SectionBeth Sommers, PhD, MPH, LAcAPHA Integrative, Complementary andTraditional Medicine SectionSteve Welsh, DCIHPC Task Force Chair
Leadership: Will States - and Lobbying byState Professional Associations - Take theLead? Oregon Inclusion in Coordinated CareOrganizations (Medicaid)– “The following integrative treatments are amongthe recommended therapies: acupuncture,chiropractic manipulation, cognitive behavioraltherapy, osteopathic manipulation.”– “In addition, yoga, intensive rehabilitation,massage, and/or supervised exercise therapy arerecommended to be included in thecomprehensive treatment plans.”– Naturopathic doctors already allowed to runCoordinated Care Organizations Vermont – S. 243, Sec. 15A An act relatingto combatting opioid abuse– 463,000 for acupuncture pilotJohn Singer, LacVermont Acupuncture AssociationLaura Ocker, LAcOregon Acupuncture Assn.Kimberly Tippens, ND, MSAOM, MPHNational Univresity of NaturalMedicine
NCCIH/Mayo Scientific Guidancefor PCPsTeam led by Richard Nahin, PhD-Acupuncture and yoga for back pain-Acupuncture and tai chi for osteoarthritis of the knee-Massage therapy for neck pain with adequate dosesand for short term benefit-Relaxation techniques for severe headaches andmigraineSeptember 2016
Convergence: Integrative PainCareLast Week!New Back Pain Guideline“Noninvasive Treatments forAcute, Subacute, andChronic Low Back Pain: AClinical Practice GuidelineFrom the American Collegeof Physicians”February 2017Proposed StandardsRevisions Related to PainAssessment andManagement."The hospital promotesaccess to non-pharmacologicpain treatment (this mayinclude alternative modalities,such as chiropractic,relaxation therapy, musictherapy).”February 20, 2017 commentperiod closed
From “Never Only Opioids” to“Never only (drug name here)”
Thank You!
Managing chronic pain:the age before and afteropioidsJANE C BALLANTYNEUNIVERSITY OF WASHINGTON, SEAT TLE
Before Descartes“Make me fully understand that the ills ofthe body are nothing else than thepunishment and the encompassing symbolfor the ills of the soul . the greatestsickness is insensibility Let me feel thispain sharply so that I can make whatever isleft of my life a continual penance to washaway the offenses I have committed.”Blaise Pascal “Priere pour demander a dieu le bon usage desmaladies” prayer circa 1659
Pain carried in a line labelled system Early reductionist view First to describe pain as aperception, existing in the brain Distinguished from sensorytransductionL'homme de Rene Descartes. Paris: 1664
“Many investigators seem grimly determined to establish .that for a given stimulus there must be a given response;that is, for so much stimulation of nerve endings, so muchpain will be experienced, and so on.This fundamental error had led to enormous waste. It isevident . that there is no simple relationship betweenstimulus and subjective response.It is also made evident that the reason for this is theinterposition of conditioning, of the processing component,of the psychic reaction.”Beecher HK Increased stress and effectiveness of placebosand “activity” drugs Science 132;91-2 July 1960
Wibert Evans “Bill” Fordyce 1923-2009Developed approaches to dealing with pain that were groundbreaking atthe time (1960s)Used behavioral principles to encourage chronic pain patients to becomeactive again and cut back on pain medicationLed the way to the integration of psychological principles and psychologistsinto the care of chronic painDeveloped the idea of operant conditioningThe idea of multidisciplinary pain management:Pain doesn’t just producepain behaviors, attitudes,movements and postures,but is produced by them. PT to improve conditioning and body awareness Learn CBT strategies for managing pain and developinghealthy habits Learn injury avoidance and unlearn fear avoidance Use drugs and interventions as indicated but do not focus onthem
We were in a very good place .And then along came opioids
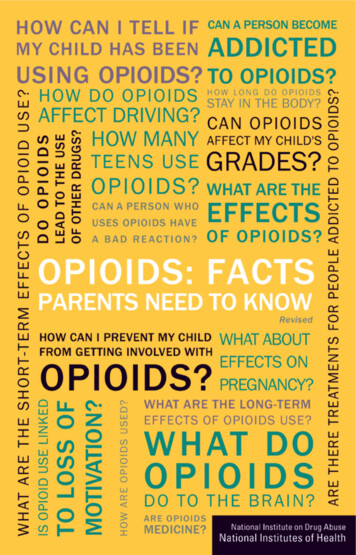
Rates of Opioid Sales, OD Deaths, and Treatment, 1999–2010Opioid Sales KG/10,00087Rate65432101999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010YearCDC. MMWR 2011
Primary non-heroin opiates/synthetics admission rates, by State(per 100,000 population aged 12 and over)
Public health impact of opioid pain reliever useFor every opioid overdose death in 2009 there were:Abuse treatmentadmissionsED visits for misuse orabusePeople withabuse/dependencePast Year Nonmedicalusers930118795Based on 15,597 OPR overdose deaths in 2009.Treatment admissions are for primary use of opioids from Treatment Exposure Data set for 2009.Emergency department (ED) visits are from DAWN (Drug Abuse Warning Network) for dependence and nonmedical use in the past year are from the 2009 National Survey on Drug Use and Health
Mortality by cause, white non-Hispanics ages 45–54Case A, Deaton A. Rising morbidity and mortality in midlife among white non-Hispanic Americans inthe 21st century. Proceedings of the National Academy of Sciences. November 2, 201532
Why did it happen?1. Palliative care physicians promoted opioids for chronic pain2. Pharmaceutical industry promoted opioids for chronic pain3. US healthcare system factors4. US cultural factorsVentafridda et al Int J Tiss React 1985Scholten & Henningfield J Pain Palliat Care Pharmacother 2016WHO Persisting Pain in Children 2012Ballantyne et al BMJ 2016
Industry-funded “educational” messages Physicians are allowing patients to suffer needlessly because of “opiophobia.” Opioid addiction is rare in pain patients. Opioids can be easily discontinued.Porter & Jick NEJM 1080Portenoy & Foley PAIN 1986Sullivan & Ballantyne Arch Int Med 2012Ballantyne & Sullivan NEJM 2015 Opioids are safe and effective for chronic pain. Palliative care principles such as titration-to-effect apply equally to chronic pain.34
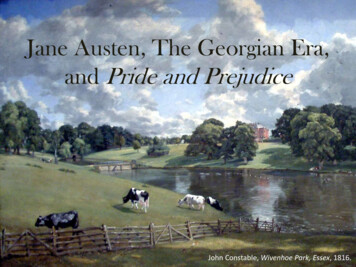
Dollars Spent Marketing OxyContin (1996-2001)JCAHO Pain Management Standards 2001Zgierska et al JAMA 2012Source: United States General Accounting Office: Dec. 2003, “OxyContin Abuse and Diversion andEfforts to Address the Problem.”
What’s wrong with using opioids long-term and continuously?1.Misunderstands chronic pain: suffering is related less to intensity than tomeaning, disability, role function, attitude and expectation, all of which can bechanged2.Commandeers the endogenous opioid system: a system that is important fordefining who we are and how we react to the world – destroys natural defenses3.Causes neuroadaptations: tolerance and dependence are linked adaptationsthat account for opioid failure4.Susceptible individuals will become addicted at a fairly constant rate (between12 and 20%): the more that is prescribed, the more addiction will occur5.Activity and exercise are therapeutic for many pain conditions, especiallymusculoskeletal pain: opioids are deactivating
Current theories about the purposes ofthe endogenous opioid system suggesttwo important categories: to provide stress-related pain relief and painenhancement (injury-related “physical pain”) to facilitate maternal-infant and otherattachments The pain and opioid systems evolved throughevolutionary processes over millions of years Giving exogenous opioids overwhelms these naturalsystems and prevents the protective, defensivemechanisms from taking place Central control (top down) contributes as much asnociception to the experience of pain and is a powerfulmeans of controlling pain Opioid systems are intimately involved in the groupprocesses, the top down effects Isolation, withdrawal, distress, family, job, culture allinfluence the development of chronic pain and areindicators of derangement in natural (opioid) systems
The overuse of opioids for chronic pain is a distinctlyUS problem .What is the US going to do about it?
Systems map for obesity
Employing self management programs to improve patientquality of life as an important component of acute andchronic pain prevention and management Use of integrated, multimodal and interdisciplinarytreatment approaches Reducing incentives for treatments with little absolutebenefit or a limited benefits relative to risks Increasing incentives and reimbursement strategies topromote high-quality coordinated pain care through anintegrated biopsychosocial approach “Safe use campaign” for opioidsDraft National Pain Strategy A comprehensive population health-level strategy for pain nStrategy.pdf
Let us go back to what Beecher and Fordyce recognized a long time ago Suffering may be expressed as physical pain, but its rootsoften lie much deeper These roots are created by past experiences and presentfears, not found in the body or explained by pathology Modern imaging enables us to see most pathological causesof pain Thus, we understand that two individuals with the samepathology on an image may experience this condition verydifferently For one person the physical pain becomes the focus for a lifeof suffering, while for another, the physical pain issublimated, or even disappears.
Cultural transformation needed is demedicalization of the most common pain conditionsOLD PATHWAYNEW PATHWAY
2016 The CDC GuidelineWhat’s new? Offers different patient selection criteria (1.)Discourages use of long-acting opioids (4.)Suggests dose limitations (5.)Recognizes ‘legacy patients’ as a different category (5.)Considers acute use as a pathway to chronic use (6.)Dowell D, Haegerich TM, Chou R. CDC Guideline for PrescribingOpioids for Chronic Pain - United States, 2016wwwcdcgov/mmwr/volumes/65/rr/rr6501e1htm 2016.
New teaching based on new evidenceCompare with old teaching Opioids are a reasonable option if allother treatments have failed People who have failed all other treatments tend to have a high-riskprofile thus opioids are often a bad choice if used for the reason that allother treatments have failed Opioids cause problematic use in up to 30%, and addiction in up to 20% Opioids rarely cause addiction if usedto treat pain (5% incidence) Risk mitigation strategies have not been shown to reduce adverseoutcome, 80% do not get good long-term efficacy Provided cautions are used, most COTis safe and effective Copious evidence now links adverse outcomes to high dose There is no ceiling dose Long acting opioids are more likely to produce tolerance leading to loss ofefficacy and dose escalation without protecting from addictionSullivan et al Arch Intern Med 2006;166:2087Vowles et al Pain 2015;156:569Chou et al Ann Intern Med 2015;162:276Le Marec et al Psychopharmacology 2011;216:297Yu et al J Pscyhiatr Res 2014;59:161 Long acting opioids provideconsistent analgesia with less riskof addiction
Is the patient a suitable candidate for opioids?BENEFITRISKSubstance abuse Hx, including smokingIntractable pain-producing diseaseFamily Hx sub abuseChildhood sexual abuseGoal is comfortPTSDAnxiety1.Sullivan MD, Ballantyne JC. Arch Int Med. 2012;172(5):433-434.2.Martin BC, Fan MY, Edlund MJ et al J Gen Intern Med. Dec2011;26(12):1450-1457.3.Schwartz AC, Bradley R, Penza KM, et al. Psychosomatics. Mar-Apr2006;47(2):136-142.4.Seal KH, Shi Y, Cohen G et al JAMA. 2012;307(9):940-947.DepressionOther MHDYoung age
The 90% of chronic pain for which opioids have not proven helpfulFibromyalgiaAxial low back pain without apathoanatomic diagnosisFranklin GM. Neurology2014;83:1277-84.Headache
CONCLUSIONS The over-prescribing of opioids in the 1990s and 2000s produced theworst iatrogenic catastrophe ever Opioids have a very limited role in the treatment of chronic painbecause they carry enormous risk and have not been shown to bebeneficial if used continuously long-term Use of opioids for chronic pain misunderstands chronic pain If we can teach people to live well with chronic pain and providethem with the right tools, that is the best we can do
INTEGRATIVE PAIN MEDICINETransformational Care
Heather Tick MA, MDClinical Associate Professorof Family Medicineand Anesthesia & Pain MedicineUW MedicineDIVISION OF PAIN MEDICINE
DISCLOSURE Author of Holistic Pain Relief Heathertickmd.com
Seven Habits of Successful ConventionalPhysicians We are well intentionedRushedWe are buried in electronic “paperwork”We rely on testsWe focus on getting a diagnosis54% in primary care suffer “burn out”We are part of the system that is the thirdleading cause of death (Makary MD,BMJ 2016;353:i2139)
A lot of trust in Validity of tests Their applicability to the unique patient weare treating The latest trend: how did we label/treatpatients before this trend, how certain werewe that it was the right approach. Drug solutions-and more drug solutions to theside effects
Less trust in The laying on of hands (Skinner, kangaroo care, nursing literature,increased vagal activity-Early Hum Dev. 2014 Mar;90(3):137-40. doi:10.1016/j.earlhumdev.2014.01.009. Epub 2014 Jan 27; ) Micronutrient deficiencies (Ames B, PNAS 2006 103 (47)17589-17594;Agarwal S, J Am Coll Nutr. 2015;34(2):126-34. doi:10.1080/07315724.2014.901196. Epub 2015 Jan 7.) The ability of the body to heal The interconnectedness of all systems (Langevain e-Chronic-Pain-andCancer-30714. Vagus nerve stimulation inhibits cytokine production andattenuates disease severity in rheumatoid arthritis PNAS 2016 113 (29) 82848289. Tracey K, TNFa reduction with vagal stim )
Less experience with The offer an intervention whose side effectsinclude better health instead of renal failure How good it feels to refocus the conversationon the pursuit of health How a focus on health as a positive attributehelps our patients and ourselves. With respect to neuroplasticity: Which circuitsdo we want to reinforce.
Less trust in Marcia Angel, NEJM, The Truth About DrugCompanies Richard Horton The Lancet, “much of the scientificliterature, perhaps half, may simply be untrue”,blaming, among other things, studies with smallsample sizes, researchers’ conflicts of interest and“an obsession” among scientists for pursuingfashionable trends of dubious importance”. Harvey Markovitch, (2010) “Editors, Publishers,Impact Factors, and Reprint Income”. PLoS Med7(10): e1000355.doi:10.1371/journal.pmed.1000355
Trust?
Risk of Standard of Care Prescription opioid inadvertent ODs kill morepeople than heroin and cocaine combined (46/d) Escalating drug use and procedures and noimprovement in outcomes Overtreating chronic backpain: Time to back off? Deyo RA, Mirza SK, Turner JA, Martin BI. J amboard Fam Med 2009;22(1):62–8. The Spine Journal. nchikanti L, Pampati V, Falco FJE, Hirsch JA. Growth of spinalInterventional pain management techniques. Spine. 2013;38(2):157–168. doi:10.1097/brs.0b013e318267f463.Manchikanti L, Pampati V, Falco FJE, Hirsch JA. Growth of spinalInterventional pain management techniques. Spine. 2013;38(2):157–168. doi:10.1097/brs.0b013e318267f463.
HOW DID WE GET THIS SO WRONG? The pressures of modern practice havepushed us to accept simple solutions tocomplex problems. We also have a story telling problem: We are abit too quick to come up with explanationsfor things we really don’t have an explanation for.(Malcolm Gladwell)
“Medical care is a public health hazard.”(Don Berwick IHI)
THE MORAL ERA YouTube: Address to the 27th annual meetingof Institute for Healthcare Improvement https://www.youtube.com/watch?v DKKyFn7e 0 Difference between QI, and transformation
Our health care model is adisease management model Personalized, individualizedcareHEALTHCREATION Time, attention Silver Bullet model- does notORwork for chronic conditionsHEALTHCARE “healing is always possible”
HEALTHCREATIONORHEALTHCARE Our health care modelproduces life longcustomers for manydifferent types ofservices Was this our intention?
Diagnosis:WHATDISTINGUISHESIM/IPM?an agreed upon labelfor a set of symptoms Benefits?It helps in urgent,acute situationsBilling, codingEntitlements Disadvantages?
What distinguishes IM/IPM?Medicine is like a game of connect the dotsWhat about the connectors?
PREVENTABLE WITH LIFESTYLE CHANGES
EPIC: European ProspectiveInvestigation into Cancer and Nutrition23,000 people for 7.8 years– Not smoking– Exercise 3.5 hr/week– Healthy diet: veg, fruit, beans, whole grains,nuts, seeds, low meat consumption– BMI 30E. S. Ford et al., “Healthy Living Is the Best Revenge: Findings from the EuropeanProspective Investigation into Cancer and Nutrition — Potsdam Study,” Archives ofInternal Medicine 169, no. 15 (2009): 1355–62.
THE KEY TO HEALTH
SUGAR Average US person consumes 150 pounds ofsugar per year ½ pound each day
Metchnikoff Nobel Prize in 1908 for work in immunity He discovered macrophages, phagocytosisand cell mediated immunity (co-recipient PaulErlich established the principles of humeralimmunity) He also developed the concept of good andbad bacteria in the gut and their associationwith health and prolonged life.
THE GUT 70-80% of the immune systemlines the gut 80% of serotonin is in the gut Enough neurons in the gutfor a small mammals brain Has a profound effect oninflammation, the immunesystem and our mood
THE MICROBIOME 10x as many cells as human cells 200x more DNA Affects digestion and nutrientabsorption Affects weight, inflammatorybiomarkers, abdominal pain,intestinal permeability,autoimmunity, mood,temperament, epigenetics,circadian rhythm .MICROBIOME
MICROBIOME
MICROBIOME EFFECTSAbdominal painO’ Mahony SM, Dinan TG, Cryan JF. The gutMicrobiota as a key regulator of visceral pain.PAIN. November 2016:1.doi:10.1097/j.pain.0000000000000779.
MICROBIOME EFFECTS van den Eisen LW, Poyntz HC et al"Embracing the Gut Microbiota: The New Frontierfor Inflammatory and Infectious Diseases." 6, no. 1,2017, Vol.6(1).“As such, beneficial modulation of the gutmicrobiota is a promising clinical target for manyprevalent diseases including inflammatory boweldisease, metabolic abnormalities such as obesity,reduced insulin sensitivity and low-gradeinflammation, allergy and protective immunityagainst infections.
MICROBIOME EFFECTS Christian LM, Galley JD, Hade EM, SchoppeSullivan S, Kamp Dush C, Bailey MT. Gutmicrobiome composition is associated withtemperament during early childhood. Brain,Behavior, and Immunity. 2015;45:118–127.doi:10.1016/j.bbi.2014.10.018.
MICROBIOME EFFECTS Voigt R, Forsyth c, Green S, Engen P,Keshavarzian A. Circadian Rhythm and the GutMicrobiome. International Review ofNeurobiology. 2016;(131):193–205.
EPIGENETICSEpigenetic gene regulation comprises the heritablechanges in gene expression that occur in the absenceof changes to the DNA sequence itself . acetylation,methylation, phosphorylation . potential fornutritional and environmental factors to influencefetal, adult, and transgenerational epigenetic generegulation, resulting in numerous phenotypicconsequencesDolinoy DC, The agouti mouse model: an epigenetic biosensor for nutritional andenvironmental alterations on the fetal epigenom, Nutr Rev. 2008 Aug; 66(Suppl 1):S7–11.
The agouti mouse model: an epigenetic biosensor fornutritional and environmental alterations on the fetalepigenomeDolinoy DC, Nutr Rev. 2008 Aug; 66(Suppl 1): S7–11. doi10.1111/j.1753-4887.2008.00056.x
Stress, VAGUS NERVE AND GUTPrenatal stress causing epigenetic changesin the fetusBonaz B, Anti-inflammatory properties of thevagus nerve:potential therapeutic implicationsof vagus nerve stimulation. Physiol. 2016 Apr 5.doi: 10.1113/JP271539
HEARTBURN AND GI HEALTH Acid stimulates– Unfolding of proteins– Gastric emptying– Pancreatic enzymes– Sterilizes food– Optimizes microbiome– nutrient absorptioninflammation
Omega 3: DHAand EPA Omega 3’s anti-inflammatoryprostaglandin pathways 3 gm DHA EPA/day reducedpainMaroon et al, SurgNeurol.2006;65:326-331
Omega 3: side effectsEffective for: Lowering TGLikely:Reduced risk of dying of heartdiseasePossibly:Reduced risk for HT, RA,Dysmenorrhea, ADHD, Raynauds,Stroke, OsteoporosisIgA nephropathy ural/993.html
Essential Fatty Acids: Inflammation R. J. Goldberg and J. Katz, “A Meta-analysis of theAnalgesic Effects of Omega-3 PolyunsaturatedFatty Acid Supplementation for InflammatoryJoint Pain,” Pain 129 (2007): 210–23. A. P. Simopoulos, A. Leaf, and N. Salem Jr.“Workshop Statement on the Essentiality of andRecommended Dietary Intakes for Omega-6 andOmega-3 FattyAcids,” Prostaglandins,Leukotrienes and Essential Fatty Acids 63, no. 3(2000):119–21
Vitamin D for pain Low vit D levels correlated to higher opioiduse (2x) and longer duration of use (2x) “vitamin D inadequacy may represent anunder-recognized source of nociception andimpaired neuromuscular functioning amongpatients with chronic pain”Turner et al, Mayo Clinic Pain Med. 2008 Nov;9(8):979-84
VITAMIN D Decreased inflammation Increased bone density Less susceptibility toinfections such as flu Less diabetes Less auto-immune disorders Possible role in cardiac andbrain health Overdose extremely rare(over 150ng/ml)Holick MF , MD PhD, Vitamin DDeficiency, N Engl J Med 2007;357:266-281July 19, 2007DOI:10.1056/NEJMra070553
Mg inhibits release of Achfrom motor end plates muscle relaxation (FM,MFPS, cramps) MAGNESIUM Magnesium depletionfacilitates neuromuscularexcitability, producingtremor, cramps, and tetany Cohen S et al,Anesthesiology2004;101:495-526
Recent rat studies onmechanisms NMDAreceptors and nerve pain MAGNESIUM Improves constipationand irritable bowel, Sleep disorders Bone health, Collagenformation
Hypomagnesemia isprobably the mostunderdiagnosed electrolytedeficiency in currentmedical practice.hypomagnesemia is notnecessarily present in amagnesium-deficient state MAGNESIUM Am J Med 1987Mar 20;82(3A)24-9.Magnesium deficiency:pathogenesis, prevalence, andclinical implications. Whang R.
Prospective study of4,497 Americans no DM Mg favorably affectsinflammation, insulinresistance and reducesonset of DM Mg intake inverselyassociated withinflammatory markers(hsCRP, IL6,fibrinogen)and fasting insulin NIH FUNDEDCARDIASTUDY Kim DJ et al. Diabetes Care 2010;33(12):2604-10
REFERENCES-MAGNESIUM Jane Higdon, “Magnesium,” Linus Pauling Institute, Oregon StateUniversity website, last updated August s/magnesium/ D. J. Kim et al., “Magnesium Intake in Relation to SystemicInflammation, Insulin Resistance, and the Incidence of Diabetes,”Diabetes Care 33, no. 12 (December 2010): 2604–10. Alexander Mauskop and Jasmine Varughese, “Why All MigrainePatients Should Be Treated with Magnesium,” Journal of NeuralTransmission 119, no. 5 (2012): 575–79. F. H. Nielsen, L. K. Johnson, and H. Zeng, “MagnesiumSupplementation Improves Indicators of Low Magnesium Statusand Inflammatory Stress in Adults Older Than 51 Years with PoorQuality Sleep,” Magnesium Research 23, no. 4 (2010): 158–68; S. Brill et al., “Efficacy of Intravenous Magnesium in NeuropathicPain,” British Journal of Anaesthesia 89, no. 5 (2002): 711–14.
VITAMIN B12 Vitamin B12 in low back pain: a randomised,double-blind, placebo-controlled crossoverstudy daily injections of 1000mcg Reduction of pain in both active arms of thecrossoverMauro GL, Eur Rev Med Pharmacol Sci - 01-MAY-2000; 4(3):53-8
VITAMIN B12 Powerful methylator (mitochondria and detox) Co factor for methionine synthase: lowershomocysteine Possibly helpful: Diabetic neuropathyFatigueFractures(Mayo Clinic)
TURMERIC(Curcuma Longa)
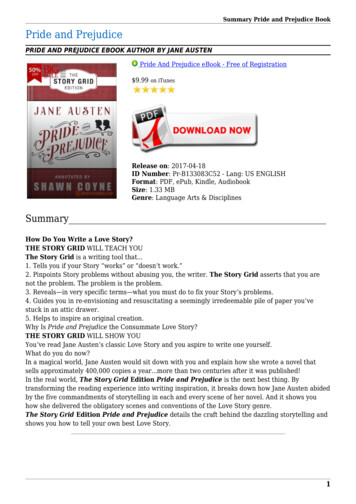
107 knee OApatients: 800 mg/dibuprofen 2g/dcurcumin for pain Kuptniratsaikul V etal, J AlternComplement Med2009; 15(8):891-7
Laparascopiccholecystectomy: Lesspain and fatigue andanalgesic use incurcumin group vsplacebo (500mg q6h)DBPC RCT Agarwal KA et al.,Surg Endosc(2011) 25:3805–3810 DOI10.1007/s00464-011-1793-z
Neuroprotective- animalmodelsTURMERIC SIDEEFFECTS New neurons in thehippocampus Studied in Alzheimersprevention and improvedfunction in Alzheimerspatients
FASCIA Langvain -Chronic-Pain-andCancer-30714. Myers, T. Fascia is more of a connector than atissue demarcation
Ultrasonographic elastography allowing us toimage fascial thickening and decreasedmovement of the fascial planes in LBP patientsvs controls which correlated with pain andfunctional limitations Langevin et al. BMC Musculoskeletal Disorders2011, 12:203http://www.biomedcentral.com/14712474/12/203
MYOFASCIAL PAIN Travell and Simons, Myofascial Pain andDysfunction: The Trigger Point Manual, vol 1, 2 C Chan Gunn “The Gunn Approach to theTreatment of Chronic Pain: IntramuscularStimulation for Myofascial Pain of RadiculopathicOrigin” Canno
as Tools in the Opioid Crisis . Foundation for Chiropractic Progress(F4CP) white paper . Dollars Spent Marketing OxyContin (1996-2001) JCAHO Pain Management Standards 2001 Zgierska et al JAMA 2012 . What's wrong with using opioids long-term and continuously? 1. Misunderstands chronic pain: suffering is related less to intensity than to