Transcription
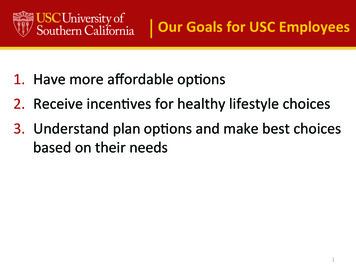
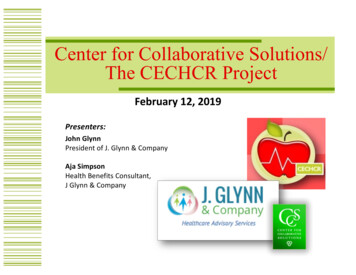
U NIO N2020 Comparing Your Health Plan OptionsUSC TROJANCARE EPOPAG EUSC PPOANTHEM HMOANTHEMMYCHOICE HMOBENEFITEPO NetworkTier 1: Keck MedicineTier 2: Anthem Prudent Buyer Tier 3: Out-of-NetworkAnthem CaliforniaCareNetworkAnthem CaliforniaCareNetworkIs a referral requiredto see a specialist?NoNoNoNoYesYesIndividual 100 100 250 600 0 0Family (3 members) 300 300 750 1,800 0 0MEDICAL DEDUC TIBLESTier 1–2 deductibles cross accumulate(count toward one another)M E D I C A L O U T- O F - P O C K E T M A X I M U MEmployee only 1,000* 1,500* 2,500* 12,500** 1,500* 3,000*Employee plus adult 2,000* 3,000* 5,000* 25,500** 3,000* 6,000*Employee plus children 3,000* 4,500* 7,500* 37,500** 4,500* 9,000*Employee plus family 3,000* 4,500* 7,500* 37,500** 4,500* 9,000*Employee plus childP R E S C R I P T I O N O U T- O F - P O C K E T M A X I M U MEmployee only 2,000* 4,850*No out-of-pocket maxCombined with medicalCombined with medicalEmployee plus adult/Child(ren) family 4,000* 7,200* (two or more people)No out-of-pocket maxCombined with medicalCombined with medical* 100% thereafter.** 100% of UCR thereafter. Usual and customary rate. Refers to the rate generally charged for a specific service by doctors or other providers in the same geographic area.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.1
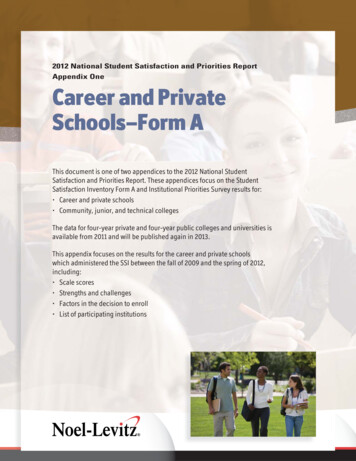
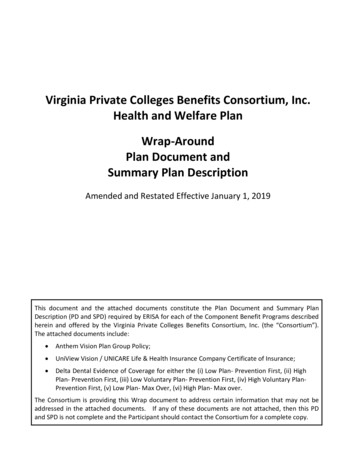
U NIO N2020 Comparing Your Health Plan OptionsUSC TROJANCARE EPOBENEFITPAG EANTHEM HMOANTHEMMYCHOICE HMOAnthem CaliforniaCareNetworkAnthem CaliforniaCareNetworkPlan pays 50% of UCR* afterdeductible/member paysdeductible plus balanceof chargesPlan pays 100% after memberpays 20Plan pays 100% after memberpays 30Plan pays 100% after memberpays 20Plan pays 100% after memberpays 40USC PPOEPO NetworkTier 1: Keck MedicineTier 2: Anthem Prudent Buyer Tier 3: Out-of-NetworkPCP office visit(including maternity)Plan pays 100% after memberpays 20 copay ( 10 copay withdesignated PCP)Plan pays 100% aftermember pays 20 ( 10 copaywith designated PCP)Plan pays 100% aftermember pays 30 ( 20 copaywith designated PCP)SCP office visitPlan pays 100% after memberpays 20Plan pays 100% aftermember pays 20Plan pays 100% aftermember pays 30Preventive carePlan pays 100%Plan pays 100%Plan pays 100%Plan pays 50% of UCR* afterdeductible/member paysdeductible plus balanceof chargesPlan pays 100%Plan pays 100%Urgent care centersMember pays 35Not availableMember pays 35Plan pays 50% of UCR* afterdeductible/member paysdeductible plus balanceof chargesMember pays 30Member pays 30Emergency care(waived if admitted)Member pays 150 copayMember pays 200copay (only available at USCVerdugo Hills Hospital)Member pays 200 copayMember pays 200 copay andany charges above 100% ofUCR*; plan pays 100% of UCRMember pays 150 copayMember pays 100 copay plus10% of cost 10 copay 10 copay after 25 deductibleBrand/formulary: 20% of cost,with a minimum 30 copay; 125 max copay 25 copay after 25 deductibleBrand/non-formulary: 45% ofcost (min 50, max 250) 40 copay after 25 deductibleSame as above, except selfadministered injectable drugs 200 (does not apply to insulin)20% of cost (maximum 100)after 25 deductibleMEDICAL BENEFITSPRESCRIPTION COST SHARINGGeneric 5 copay 5 copayBrand(no generic available) 25 copay 25 copayBrand(generic available) 70 copay 70 copaySpecialty drug 125 copay 125 copayIf filled at a non-Networkpharmacy, the plan willreimburse you 50% of theplan’s network contractedrate (not of cost);reimbursement requestmust be received within60 days of fill* Usual and customary rate. Refers to the rate generally charged for a specific service by doctors or other providers in the same geographic area.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.2
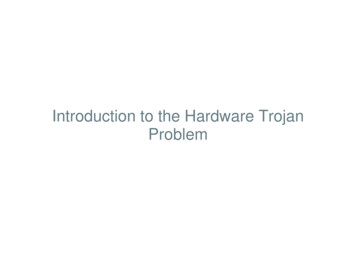
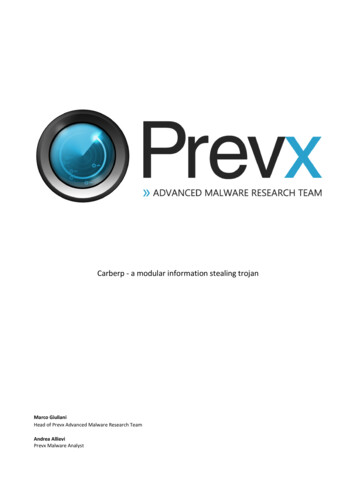
U NIO N2020 Comparing Your Health Plan OptionsUSC TROJANCARE EPOBENEFITPAG EANTHEM HMOANTHEMMYCHOICE HMOAnthem CaliforniaCareNetworkAnthem CaliforniaCareNetworkPlan pays 100%Plan pays 100%Plan pays 50% of UCR* aftermember pays 600 copay/admission. Member pays 600copay/admission plus balanceof chargesPlan pays 100% after memberpays 250 copay/admissionPlan pays 80%USC PPOEPO NetworkTier 1: Keck MedicineTier 2: Anthem Prudent Buyer Tier 3: Out-of-NetworkPlan pays 100%Not availablePlan pays 80% afterdeductible; member pays 20%after deductibleAMBULANCEEmergency groundtransportation(non-emergency transportrequires prior authorization)Plan pays 80% of UCR* afterdeductible; member paysdeductible plus balanceof chargesI N PAT I E N T H O S P I TA L S E R V I C E S ( A L L H O S P I TA L A D M I S S I O N S A R E S U B J E C T T O P R I O R AU T H O R I Z AT I O N)FacilityPlan pays 100% (not subject todeductible)Plan pays 100% after memberpays 300 copay/admissionMaternity delivery onlyavailable at USC Verdugo HillsHospitalMaternity delivery: 100copay/admission only at GoodSamaritan Hospital whendelivery is done by a USC CareMedical Group ObstetricianPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 80% afterdeductible; member paysdeductible and 20% ofallowed amountPlan pays 50% of UCR* afterdeductible; member paysdeductible plus balance ofcharges 50% of UCRPlan pays 100%Plan pays 100%FacilityPlan pays 100% after member 200 copay/admissionPlan pays 100%Plan pays 100% after memberpays 200 copay/admissionPlan pays 50% of UCR* not toexceed 2700 after memberpays 600 copay/admissionplus remainder of chargesPlan pays 100% after member 250 copay/admissionPlan pays 80%PhysicianPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 80% afterdeductible; member paysdeductible and 20% ofallowed amountPlan pays 50% of UCR* afterdeductible; member paysdeductible and balanceof chargesPlan pays 100%Plan pays 100%Surgery/doctor visitsPlan pays 100% after memberpays 100 copay/admissionA M B U L AT O RY S U R G E RY* Usual and customary rate. Refers to the rate generally charged for a specific service by doctors or other providers in the same geographic area.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.3
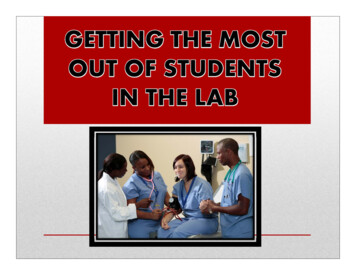
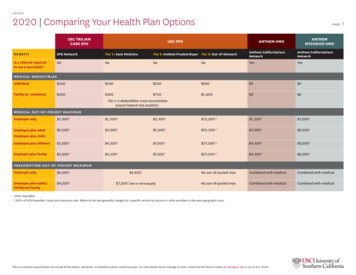
U NIO N2020 Comparing Your Health Plan OptionsUSC TROJANCARE EPOBENEFITEPO NetworkPAG EUSC PPOTier 1: Keck MedicineTier 2: Anthem Prudent Buyer Tier 3: Out-of-NetworkANTHEM HMOANTHEMMYCHOICE HMOAnthem CaliforniaCareNetworkAnthem CaliforniaCareNetwork4B E H AV I O R A L H E A LT H A N D S U B S TA N C E U S E D I S O R D E R S E R V I C E SAuthorizationInpatient, partial hospitalization,residential treatment center, andIntensive outpatient visits requireprior authorizationInpatient services, partial hospitalization, residential treatment center, and intensive outpatientvisits require prior authorizationInpatient, partial hospitalizationand residential treatmentrequire prior authorizationInpatient, partial hospitalizationand residential treatmentrequire prior authorizationInpatient - facilityPlan pays 100% after memberpays 100 copay/admissionPlan pays 100%Plan pays 100% after memberpays 300 copay/admissionPlan pays 50% of UCR.*Member pays 600 copay/admission plus balanceof chargesPlan pays 100% after member 250 copay/admissionPlan pays 80%Inpatient - physicianPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 90% afterdeductible; member paysdeductible and 10% of allowedamountPlan pays 80% afterdeductible; member paysdeductible and 20% ofallowed amountPlan pays 50% of UCR* afterdeductible; member paysdeductible and balanceof chargesPlan pays 100%Plan pays 100%Partial hospitalizationPlan pays 90% afterdeductible; member paysdeductible and 10% ofallowed amountPlan pays 90% afterdeductible; memberpays deductible and10% of allowed amountPlan pays 80% afterdeductible; member paysdeductible and 20% ofallowed amountPlan pays 50% of UCR* afterdeductible; member paysdeductible and balanceof chargesPlan pays 100%Plan pays 80%Residential treatmentPlan pays 100% after memberpays 100 copay/admissionPlan pays 100%Plan pays 100% after memberpays 300 copay/admissionPlan pays 50% of UCR.*Member pays 600 copay/admission plus balanceof chargesPlan pays 100% after member 250 copay/admissionPlan pays 80%Outpatient - facilityPlan pays 100% after memberpays 200 copay/admissionPlan pays 100%Plan pays 100% after memberpays 200 copay/visitPlan pays 50% of UCR* not toexceed 2,700 after memberpays 600 copay/admissionplus remainder of all chargesPlan pays 100%Plan pays 80%Plan pays 100% aftermember pays 20 copay/visitPlan pays 100% aftermember pays 30 copay/visitPlan pays 50% of UCR* afterdeductible; member paysdeductible and balanceof chargesPlan pays 100% after memberpays 20 copay/visitPlan pays 100% aftermember pays 30 copay/visitNoYesYesEmergency onlyEmergency onlyOutpatient - professional Plan pays 100% after memberpays 20 copay ( 10 copay withdesignated PCP)O T H E R H E A LT H S E R V I C E SCoverage in foreigncountriesEmergency only* Usual and customary rate. Refers to the rate generally charged for a specific service by doctors or other providers in the same geographic area.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.
U NIO N2020 Financial Incentives/Surcharges to Medical PlansPAG EEMPLOYEE COST IMPACTSURCHARGE/INCENTIVE DESCRIPTIONAFFEC TED PL ANM O N T H LYA N N UA LHealth assessment creditAll plans except Anthem MyChoice HMOSubtract 40Subtract 480Tobacco-free creditAll plans except Anthem MyChoice HMOSubtract 25Subtract 300PCP selection discountUSC Trojan Care EPO and USC PPO plans only 10 off PCP copaysNot applicableWorking spouse surchargeAll plans except Anthem MyChoice HMOAdd 100Add 1,2002020 Vision2020 VSP CHOICE PLANBENEFITIN-NET WORK USCR O S K I P R OV I D E RIN-NET WORKV S P P R OV I D E RO U T- O F - N E T W O R KP R OV I D E RWell vision exam (one exam/year) 0 copay 15 copay 15 copay up to 45Frames 25 copay* up to 170(every other calendar year) 25 copay* up to 170(every other calendar year) 25 copay* up to 55(every other calendar year)Single vision, lined bifocal, lined trifocal, lenticular 25 copay*(every calendar year) 25 copay*(every calendar year) 25 copay* up to 45- 125(every calendar year)Progressive 55– 175 copay(every calendar year) 55– 175 copay(every calendar year) 25 copay up to 85 allowance(every calendar year)Contacts (in lieu of glasses)Up to 150 allowance(every calendar year)Up to 150 allowance(every calendar year)Up to 150 allowance(every calendar year)LENSES* Only one copay applies when lenses and frames are purchased.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.5
U NIO N2020 DentalPAG EDELTA DENTAL PPO PLAN6UNITED CONCORDIA DHMO PLANServices at the USC Schoolof DentistryIn-NetworkOut-of-NetworkPrimary Dental Office (PDO) 1,500/person 1,500/person 1,500/personNot applicableIndividual 50 50 75 0Per family 150 150 225 0100%, no deductible90%, no deductible80%, after deductible 0 copay100%, after deductible80%, after deductible70%, after deductible 0– 140 copay100%, after deductible60%, after deductible50%, after deductibleCrowns: 25– 75 copay*Bridges: 70– 90 copay*Dentures: 100– 120 copayComprehensive orthodontic treatment50%50%50% 1,500– 2,000 copayLifetime maximum 1,500 1,500 1,500Not applicable. Orthodontic benefits areavailable once per lifetime per member.Eligibility for orthodontiaCovers both children and adultsCovers both children and adultsCovers both children and adultsCovers both children and adultsImplant rider50%50%50%Not coveredImplants lifetime maximum 1,500 1,500 1,500Not applicableBENEFITO U T- O F - P O C K E T M A X I M U MOut-of-pocket maximum (combined)DEDUC TIBLEP R E V E N T I V E A N D D I AG N O S T I CCleaning, exams, x-rayBASIC SERVICESRoutine extractions, fillings, root canal therapy, osseous surgery, oral surgeryMA JOR SERVICESCrowns, bridges, denturesORTHODONTIAIMPL ANTS* Charges for the use of precious (high noble) or semiprecious (noble) metal are not included in the copayment for crowns, bridges, pontics, inlays and onlays. The decision to use these materials is a cooperative effort between the provider and the patient, based onthe professional advice of the provider. Providers are expected to charge no more than an additional 125 for these materials.This is a summary only and does not include all the details, exclusions, or limitations about covered services. For more details about coverage or costs, contact the HR Service Center at uschr@usc.edu or (213) 821-8100.
available at USC Verdugo Hills Hospital Plan pays 100% after member pays 300 copay/admission Maternity delivery: 100 copay/admission only at Good Samaritan Hospital when delivery is done by a USC Care Medical Group Obstetrician Plan pays 50% of UCR* after member pays 600 copay/ admission. Member pays 600 copay/admission plus balance of charges