Transcription
ISSN 2691-7475Health Policy BriefJuly 2020Despite Insurance, the Poorest AdultsHave the Worst Access to Dental CareNadereh Pourat and Maria DitterSUMMARY: Oral health is critical for overallhealth and well-being, yet it is not consideredan essential health benefit for adults underthe Patient Protection and Affordable CareAct. Long-standing income disparities inoral health have been documented and arelinked to lower rates of dental insurance andsubsequent limited access to oral health care.We examined pooled data from the 2017 and2018 California Health Interview Surveys toassess whether there were income and dentalinsurance disparities among California adults,and, if so, whether such disparities included‘‘Dental servicesare not anessential healthbenefit under theACA and arenot covered bypublic programssuch as Medicare.’’Oral health is an integral componentof overall health.1 Evidenceindicates that oral health depends on timelycare that includes oral health education,preventive services, and early detection andtreatment of dental problems.1 However,evidence also indicates that low-incomeadults have poorer oral health, whichis potentially linked to lack of dentalinsurance.2Like health insurance, dental insurancepromotes access to care by reducing financialbarriers to access.3 However, dental insuranceis different from health insurance in severalrespects. For one thing, private dentalinsurance is offered less frequently than healthinsurance by employers. Without premiumsharing from employers, dental insurancepremiums are less affordable to lower-incomepopulations. In addition, dental services arenot considered an essential health benefitaccess to timely dental care. We found that lowincome California adults were less likely to havehad timely dental visits, more likely to have hadvisits for dental problems, and less likely to havehad private dental insurance than their higherincome counterparts. We also found that dentalinsurance alleviated some, but not all, incomedisparities in access. These findings highlightthe importance of considering dental healthas an essential health benefit and of ensuringparity in dental benefits, among other potentialpolicy solutions for reducing disparities indental coverage and access.under the Patient Protection and AffordableCare Act and are not covered by publicprograms such as Medicare. Adult dentalbenefits are optional for Medicaid (Medi-Calin California), and California is one of 35states that include this benefit.4 Most dentalinsurance policies have an annual cap onbenefit amounts, as well as restrictions oncoverage of some services.5,6 Medi-Cal haslower provider reimbursement levels anda lower rate of provider participation thanprivate dental insurance.7 Private insurancemay also have high levels of cost sharing onspecific services, which may contribute toreduced dental visits.8Access to dental care is measured by visits todental providers to receive preventive care anddental treatment. Healthy People 2020 set thetarget for this access indicator as at least onedental visit per year for 49% of the populationby 2020.9 The frequency of visits varies by
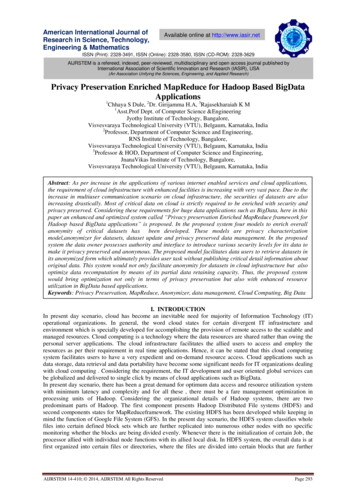
UCLA CENTER FOR HEALTH POLICY RESEARCH2Exhibit 1Timeliness of Dental Visits by Federal Poverty Level (FPL), Adults Ages 18 and Older,California, 2017–201817%24%18%13%6%14%23%13%More than 5 years agoor neverMore than 1 year andup to 5 years ago6 to 12 months ago17%Up to 6 months ago67%41%0%–138% FPL(6.97 million)47%139%–249% FPL(5.11 million)At or Above 250% FPL(17.49 million)Sources: 2017 and 2018 California Health Interview Surveys‘‘Our aimwas to assesswhether incomedisparities inaccess to dentalcare exist, andwhat potentialrole dentalinsurancemight have inaddressing thesedisparities.’’dentist recommendations, which are basedon the oral health of individuals. Most dentalinsurance policies and Medi-Cal cover up totwo preventive visits per year.This policy brief examines timeliness of andreasons for dental visits among Californiaadults by income and insurance coverage.We pooled data from the 2017 and 2018California Health Interview Surveys (CHIS)to obtain the most recent available data onoral health access for California adults. Ouraim was to assess whether income disparitiesin access to dental care exist among Californiaadults, and, if such disparities exist, whatpotential role dental insurance might have inaddressing these disparities.We used the federal poverty level (FPL)to measure income, identifying Californiaadults with incomes at or below 138% FPL( 17,237 for a single person and 35,535 fora household of four) as those whose incomeswere lowest and were consistent with MediCal eligibility criteria.Low-Income Californians Have LessTimely Dental Visits Than Higher-IncomeIndividualsThere is no single requirement for frequencyof dental visits, as the need for care is highlydependent on individual risk factors. However,the American Dental Association recommendsa minimum of one annual visit, and mostsurvey data examine this frequency.10 CHISrespondents reported on how long it hadbeen since they had had a dental visit, whichallowed us to examine both variations inannual visits and the time intervals betweenvisits. We found that these indicators variedby income (Exhibit 1). Among low-incomeadults (0%–138% FPL), we found that 41%had had a dental visit less than six months ago,and 18% had had a visit 6–12 months ago.Combined, 59% of low-income adults (datanot shown) had visited a dentist in the lastyear. In contrast, 67% of those with incomesabove 250% FPL ( 31,225 for a single personand 64,375 for a household of four) had hada visit less than six months ago, and 13% had
UCLA CENTER FOR HEALTH POLICY RESEARCHhad a visit 6–12 months ago. Combined, 80%of adults with the highest incomes had had adental visit last year.Low-Income Californians Visit DentistsMore Frequently Than Higher-IncomeAdults for Dental ProblemsCHIS respondents were asked whether theirlast dental visit was for preventive care, aspecific problem, or both. We examinedwhether low-income adults (0%–138% FPL)had visited dentists for specific problems(including those who had visited for bothpreventive and specific problems) at adifferent rate than that of higher-incomeadults. We found that 41% of low-incomeadults had visited a dentist for specificproblems, compared to 23% of adults withincomes at or above 250% FPL (Exhibit 2).Medi-Cal Is the Dominant Form of DentalCoverage Among Low-Income AdultsWe identified adults with private dentalinsurance, Medi-Cal, and no dental insuranceand examined types of coverage reportedby income. Sixteen percent of low-incomeadults (0%–138% FPL) had private dentalinsurance, and 64% had Medi-Cal (Exhibit 3).In contrast, 69% of those with incomesLast Dental Visit for Specific Problem byFederal Poverty Level (FPL), Adults Ages 18and Older, California, 2017–201830%35%23%0%–138% FPL(6.59 million)139%–249% FPL(4.95 million)At or Above250% FPL(17.28 million)Sources: 2017 and 2018 California Health Interview Surveysat or above 250% FPL had private dentalinsurance, and 8% had Medi-Cal (a smallshare of higher-income populations receivedMedi-Cal under specific circumstances,including high medical expenses). Data alsoshowed that a smaller proportion of lowincome adults (20%) had no dental insurancecompared to those with incomes at or above250% FPL (24%).24%8%64%36%69%Private16%139%–249% FPL(5.11 million)Sources: 2017 and 2018 California Health Interview SurveysNote: Private dental insurance may include a small proportionwith military or other publicly funded coverage.UninsuredMedi-Cal34%0%–138% FPL(6.97 million)Exhibit 241%Type of Dental Insurance by Federal Poverty Level (FPL), Adults Ages 18 and Older,California, 2017–201820%3At or Above 250% FPL(17.49 million)Exhibit 3
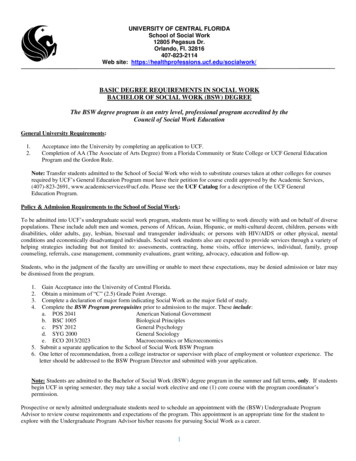
UCLA CENTER FOR HEALTH POLICY RESEARCH4Exhibit 4Timeliness of Dental Visits by Dental Insurance and Federal Poverty Level (FPL), Adults Ages18 and Older, California, 43%41%36%28%PrivateMedi-Cal Uninsured0%–138% FPL(4.14 million)PrivateMedi-Cal Uninsured139%–249% FPL(3.23 million)6 to 12 months ago57%PrivateMedi-Cal UninsuredAt or Above 250% FPL(14.05 million)Up to 6 months agoSources: 2017 and 2018 California Health Interview SurveysNote: Private dental insurance may include a small proportionwith military or other publicly funded coverage.‘‘Having a higherincome wassignificantlyassociated withmore visits . forboth privatelyinsured anduninsuredadults.’’Dental Insurance Improves Timelinessof Dental Visits, but Income DisparitiesRemainWhen we examined the joint relationship oftype of insurance coverage with timelinessof visits by income, we found that having ahigher income was significantly associatedwith more visits within the past six monthsfor both privately insured and uninsured adults(Exhibit 4). Among privately insured adults,56% of low-income adults (0%–138% FPL)had had a visit within the past six months,compared to 73% of those with incomes at orabove 250% FPL. Among uninsured adults,28% of low-income adults had had a dentalvisit within the past six months, compared to57% of those with incomes at or above 250%FPL. Among adults with Medi-Cal coverage,however, the timeliness of dental visits didnot significantly increase by income.
UCLA CENTER FOR HEALTH POLICY RESEARCH5Last Dental Visit for Specific Problem by Federal Poverty Level (FPL) and Dental Insurance,Adults Ages 18 and Older, California, 2017–2018Exhibit 543%43%39%38%32%31%28%27%20%PrivateMedi-Cal Uninsured0%–138% FPL(6.59 million)PrivateMedi-Cal Uninsured139%–249% FPL(4.95 million)PrivateMedi-Cal UninsuredAt or Above 250% FPL(17.28 million)Sources: 2017 and 2018 California Health Interview SurveysNote: Private dental insurance may include a small proportionwith military or other publicly funded coverage.Dental Visits for Specific Problems AreLeast Common Among Privately InsuredAdults, but Income Disparities PersistWe analyzed the data to determine whetherrates of dental visits for a specific problemvaried by type of dental insurance and income(Exhibit 5). Overall rates for visits due to aspecific problem declined significantly forhigh-income individuals, irrespective of typeof insurance. However, results also indicatedthat privately insured adults in all incomegroups visited dentists for a specific problemsignificantly less often than adults who hadMedi-Cal or who were uninsured. These ratesalso varied by income. Among low-incomeadults (0%–138% FPL), 31% of those whowere privately insured reported having visiteda dentist for a specific problem, compared to43% of the Medi-Cal and uninsured groups.Among those with incomes at or above 250%FPL, these rates were lower for those withprivate insurance (20%) or Medi-Cal (32%)and those who were uninsured (28%).Implications and Policy RecommendationsWe found that a higher percentage ofCalifornia adults had had a dental visit inthe last year than the Healthy People 2020target of 49%. However, we found incomedisparities in timeliness of visits, withlow-income adults more likely than highincome adults to have had a visit for a dentalproblem. Furthermore, we found that amongthose who were uninsured, low-incomeadults (0%–138% FPL) had the lowest ratesof dental visits compared to their higher-‘‘Low-incomeadults are morelikely to havehad a visitfor a dentalproblem.’’
UCLA CENTER FOR HEALTH POLICY RESEARCH6‘‘Low-incomeadults haveless access todental servicesfor preventivecare and earlydiagnosis ofproblems.’’income counterparts. Also, we found thatalthough most low-income adults had dentalinsurance because of enrollment in Medi-Cal,this advantage did not translate into betteror more timely access to dental visits forthis group compared to those with incomesat or above 250% FPL. Similarly, Medi-Calcoverage did not reduce the likelihood ofdental visits for specific problems for lowincome adults. Our findings were consistentwith other studies that found more publicdental coverage, infrequent dental checkups, fewer dental visits, and higher unmetneed for dental treatment among lowincome adults compared to higher-incomepopulations.11, 12Collectively, our findings imply that lowincome adults (0%–138% FPL) have lessaccess to dental services for preventive careand early diagnosis of problems, whichin turn leads to missed opportunities topromote better oral health among thispopulation. Policies are needed that promotethe availability of affordable dental insurancefor adults. Such policies should involveinclusion of dental services as an essentialhealth benefit, regulation of premiums,standardization of dental benefits and costsharing, and parity between dental andmedical benefits.Policies are also needed to address thelimited role of Medi-Cal in reducing incomedisparities in access to dental services. Inaddition, policies should be establishedthat promote higher reimbursement ratesfor dental services, along with financialand nonfinancial incentives to encouragebetter participation of dentists in MediCal. Financial incentives have been usedsuccessfully by Medi-Cal to promote accessto dental care of children.13 CaliforniaProposition 56 provided supplementalpayments for several dental services underMedi-Cal during fiscal years 2017–18 and2018–19. However, the continuation of thesepayments is in question due to the financialimpact of COVID-19 on the state budget.The data in this brief were unlikely to havecaptured the impact of these paymentson access to dental care among Medi-Calbeneficiaries.The impact of COVID-19 is likely to includesignificant changes in dental coverageassociated with loss of employment-basedinsurance. The economic recession associatedwith the virus is also likely to lead tocutbacks in coverage of adult dental care,which is an optional Medi-Cal benefit. Thesechanges are likely to exacerbate the incomedisparities highlighted in this brief.
UCLA CENTER FOR HEALTH POLICY RESEARCHData Source and MethodsWe pooled 2017 and 2018 California HealthInterview Survey (CHIS) data for these analyses.Income was measured based on the total annualincome of a household divided by the number ofindividuals in the household and reported as apercentage of the federal poverty level. We consideredthose who had had Medi-Cal insurance at any timeduring the past year to have had dental insurance,regardless of their response to the question onhaving dental insurance. Among the remainder ofrespondents, we identified those who had had dentalinsurance and those who had lacked any dentalinsurance. Some Medi-Cal beneficiaries—particularlythose whose income was above 138% FPL—mayhave had limited-scope Medi-Cal, although this datamay be underreported.Endnotes12345Author InformationNadereh Pourat, PhD, is associate director of theUCLA Center for Health Policy Research anddirector of the center’s Health Economics andEvaluation Research Program, a professor of healthpolicy and management at the UCLA FieldingSchool of Public Health, and a professor at theUCLA School of Dentistry. Maria Ditter, Dr.med,MPH, is a research analyst at the UCLA Center forHealth Policy Research.Funder InformationThis policy brief was supported by a generous grantfrom the California Wellness Foundation (contractnumber 2018-230).AcknowledgmentsThe authors would like to thank Julian Aviles andAndrew Juhnke for their assistance with statisticalanalysis, and Tiffany Lopes and Venetia Lai fortheir editing and production support. The authorsalso thank Jayanth Kumar, DDS, MPH; ShannonConroy, Phd, MPH; Earl Lui; and Todd Hughes fortheir helpful comments on this brief.Suggested CitationPourat N, Ditter M. 2020. Despite Insurance, thePoorest Adults Have the Worst Access to Dental Care.Los Angeles, Calif.: UCLA Center for Health PolicyResearch.7678910111213U.S. Department of Health and Human Services. 2000.Oral Health in America: A Report of the Surgeon General.Rockville, Md.: U.S. Department of Health and HumanServices, National Institute of Dental and CraniofacialResearch, National Institutes of Health. -10/hck1ocv.%40www.surgeon.fullrpt.pdfSanders B. 2012. Dental Crisis in America—The Need toExpand Access. Washington, D.C.: U.S. Senate Committeeon Health, Education, Labor, & Pensions. LCRISIS.REPORT.pdfManski RJ, Schimmel Hyde J, Chen H. 2016.Differences Among Older Adults in the Types of DentalServices Used in the United States. Inquiry: The Journalof Health Care Organization, Provision, and Financing(Sage Journals). Vol. 53. 958016652523DHCS. 2019. Restoration of Adult Dental Services.Sacramento, Calif.: California Department of Health CareServices. Adult Dental.aspxCohens K. 2017. Denti-Cal for Adults. Fact Sheet.Justice in Aging. 2017/02/Denti-Cal-for-Adults.pdfVujicic M, Buchmüller T, Klein R. 2016. DentalCare Presents the Highest Level of Financial Barriers,Compared to Other Types of Health Care Services. HealthAffairs 35(12): 2176-2182. haff.2016.0800Ku L. 2009. Medical and Dental Care Utilization andExpenditures Under Medicaid and Private HealthInsurance. Medical Care Research and Review (SageJournals) 66(4):456-471. 9334896ADA. 2012. Breaking Down Barriers to Oral Health for AllAmericans: The Role of Finance. Chicago, Ill.: AmericanDental Association. https://www.ada.org/ /media/ADA/Publications/ADA%20News/Files/7170 Breaking DownBarriers Role of Finance.pdf?la enHealthy People 2020. Data table: “Children, adolescents,and adults who visited the dentist in the past year bytotal.” Rockville, Md.: Office of Disease Preventionand Health Promotion, U.S. Department of Health andHuman Services. ?category 1&by Total&fips -1ADA. 2013. American Dental Association Statement onRegular Dental Visits. Chicago, Ill.: American DentalAssociation. t-on-regular-dental-visitsBerchick ER, Barnett JC, Upton RD. 2019. HealthInsurance Coverage in the United States: 2018. CurrentPopulation Reports. Washington, D.C.: U.S. CensusBureau. publications/2019/demo/p60-267.pdfKramarow EA. 2019. Dental Care Among Adults Aged 65and Over, 2017. NCHS Data Brief. Centers for DiseaseControl and Prevention. .htmHarrington M, Felland L, Peebles V, et al. 2019.Evaluation of the Dental Transformation Initiative: InterimEvaluation Report. Ann Arbor, Mich.: he California HealthInterview Survey (CHIS)covers a wide array ofhealth-related topics,including health insurancecoverage, health statusand behaviors, and accessto health care. It is basedon interviews conductedcontinuously throughoutthe year with respondentsfrom more than 20,000California households.CHIS is a collaborationbetween the UCLA Centerfor Health Policy Research,California Department ofPublic Health, CaliforniaDepartment of Health CareServices, and the PublicHealth Institute. For moreinformation about CHIS,please visit chis.ucla.edu.
UCLA CENTER FOR HEALTH POLICY RESEARCH10960 Wilshire Blvd., Suite 1550Los Angeles, California 90024The UCLA Centerfor Health Policy Researchis part of theUCLA Fielding School of Public Health.The analyses, interpretations, conclusions,and views expressed in this policy brief arethose of the authors and do not necessarilyrepresent the UCLA Center for Health PolicyResearch, the Regents of the Universityof California, or collaboratingorganizations or funders.PB2020-5Copyright 2020 by the Regents of theUniversity of California. All Rights Reserved.Editor-in-Chief: Ninez A. Ponce, PhDPhone: 310-794-0909Fax: 310-794-2686Email: chpr@ucla.eduhealthpolicy.ucla.eduRead this publication online
private dental insurance.7 Private insurance may also have high levels of cost sharing on specific services, which may contribute to reduced dental visits.8 Access to dental care is measured by visits to dental providers to receive preventive care and dental treatment. Healthy People 2020 set the target for this access indicator as at least one