Transcription
Transitional care management (TCM)Subject to disclaimer on Salient University.
Hospital costsexceed 24 billionfor Medicarepatients readmittedwithin 30 days ofdischargePreventing hospitalreadmissions canlead to betterpatient outcomesand lower costs26.9% ofreadmissions arepotentiallypreventableSubject to disclaimer on Salient al-readmissions-by-addressing-the-causes/
The Transitions of Care visit aims to prevent readmissionsby improving care coordination and closing gaps in carefor patients as they transition from hospital or post-acutecare to homeSubject to disclaimer on Salient University.
TCM BenefitsDoctors, Patients, and ACOs Practice Strengthen the provider/patient partnership Create a sustainable revenue stream for the practice Patients Close care gaps during transitions Keep patients out of the hospital Enhance provider/patient relationshipGoodfor theACOGood forPatients ACO GoodforPracticeReduce readmissionsSubject to disclaimer on Salient University.
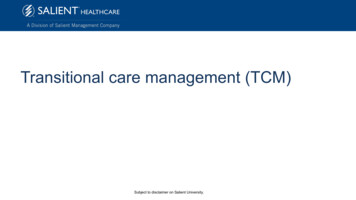
TCMs ProvideIncreased FFS ReimbursementComparison of Reimbursement between Level 5 E/M Visit and 7-day TCMVisit 250 200 150 100 50 0E/M Office Visit (99215)Subject to disclaimer on Salient University.7-day TCM Visit (99496)Reimbursement Ranges Based on the 2020 Physician Fee ScheduleNon-Facility Price and Non-Facility Limiting Charge99496: 226.05- 346.1099215: 136.12- ule/search/searchresults.aspx?Y 0&T 0&HT 0&CT 3&H1 99215&M 1
TCM Sample Workflow: Team Based actNon-face-to-face ServicesFace-to-Face ServicesAfter the VisitPractice receives anotification that a patienthas been discharged froman inpatient settingRN/MA calls the patient to determinewhether the patient needs a TCM visitand completes non face-to-faceinteraction. Schedules visit asappropriate (or transfers to scheduler).RN completes initial portion of the visit and identifies“red flags” for the PCP.RN/MA follows up with thepatient regarding anyidentified gaps andreferrals.RN/MA meet with the patient after the PCP face-toface and enrolls patient in care management orother community resources.Document encounter in EHR template.Document encounter in EHR template.PCPPCP completes face-to-face services for the patient,addressing issues that will help to prevent thereadmission. PCP identifies if the patient may benefitfrom care management and provides referrals to otherservices.Document encourage in EHR template.Bill for TCM visitBillerSubject to disclaimer on Salient University.
What patients are eligible for TCMs?TCM services are furnished following the beneficiary’s discharge from one of these inpatienthospital settings: Inpatient Acute Care HospitalInpatient Psychiatric HospitalLong Term Care HospitalSkilled Nursing FacilityInpatient Rehabilitation FacilityHospital outpatient observation or partial hospitalizationPartial hospitalization at a Community Mental Health CenterFollowing discharge from one of the above settings, the beneficiary must be returned to his or hercommunity setting, such as: HomeDomiciliaryRest homeAssisted CN908628.pdfSubject to disclaimer on Salient University.
Components of the TCMInteractive contact within 2 business days The contact may be via telephone, e-mail, or face-to-face.Certain non-face-to-face services Review need for or follow-up on pending diagnostic tests and treatments Interact with other health care professionals who will assume or reassume care of thebeneficiary’s system-specific problems Provide education to the beneficiary, family, guardian, and/or caregiver Establish or re-establish referrals and arrange for needed community resources Assist in scheduling required follow-up with community providers and servicesFace-to-face N908628.pdfSubject to disclaimer on Salient University.
There are two types of TCMs99495TCM with moderate medical decisioncomplexity with a face-to-face visit within14 calendar days of discharge99496TCM with high medical decisioncomplexity with a face-to-face visit withinseven calendar days of t-ICN908628.pdfSubject to disclaimer on Salient University.
Patient identification for TCMsThe key to the success of the TCM initiative is for a practice to be able to identifypatients immediately after they have been discharged, so that the practice canperform outreach within 2 business days.This can be accomplished through: Connection with a Health Information Exchange or vendor that provides these notifications Discharge planners providing fax/phone/secure email notifications to the practice Access to hospital EHR by the practiceSubject to disclaimer on Salient University.
Using Data to Assess the Salient Trickle-DownEffectSubject to disclaimer on Salient University.
Using Data to Assess the Salient Trickle-DownEffectSubject to disclaimer on Salient University.
Transitional care management (TCM) Subject to disclaimer on Salient University. Hospital costs exceed 24 billion for Medicare patients readmitted within 30 days of discharge 26.9% of readmissions are potentially preventable Preventing hospital readmissions can lead to better patient outcomes and lower costs