Transcription
HEALTH SYSTEMS AND POLICY ANALYSISPOLICY BRIEF 25How can eHealth improve carefor people with multimorbidityin Europe?Francesco BarbabellaMaria Gabriella MelchiorreSabrina QuattriniRoberta PapaGiovanni LamuraOn behalf of the ICARE4EU consortium
Keywords:Chronic DiseaseComorbidityTelemedicineEurope NIVEL and TU Berlin 2016All rights reserved. NIVEL and TU Berlin have granted the EuropeanObservatory on Health Systems and Policies permission for thereproduction of this Policy Brief.Address requests about publications related to theICARE4EU project to:NIVELDr. Mieke RijkenP.O. Box 15683500 BN UtrechtThe NetherlandsEmail: m.rijken@nivel.nlThe content of this Policy Brief represents the views of the authorsonly and is their sole responsibility; it cannot be considered to reflectthe views of the European Commission and/or the Consumers,Health, Agriculture and Food Executive Agency or any other bodyof the European Union. The European Commission and the Agencydo not accept any responsibility for use that may be made of theinformation it contains.What is a Policy Brief?This policy brief is one of anew series to meet the needsof policy-makers and healthsystem managers. The aim isto develop key messages tosupport evidence-informedpolicy-making and the editorswill continue to strengthenthe series by working withauthors to improve theconsideration given to policyoptions and implementation.A policy brief is a short publication specifically designed to provide policy-makers withevidence on a policy question or priority. Policy briefs: Bring together existing evidence and present it in an accessible format Use systematic methods and make these transparent so that users can have confidencein the material Tailor the way evidence is identified and synthesised to reflect the nature of the policyquestion and the evidence available Are underpinned by a formal and rigorous open peer review process to ensure theindependence of the evidence presented.Each brief has a one page key messages section; a two page executive summary giving asuccinct overview of the findings; and a 20 page review setting out the evidence. The ideais to provide instant access to key information and additional detail for those involved indrafting, informing or advising on the policy issue.Policy briefs provide evidence for policy-makers not policy advice. They do not seek toexplain or advocate a policy position but to set out clearly what is known about it. Theymay outline the evidence on different prospective policy options and on implementationissues, but they do not promote a particular option or act as a manual for implementation.
How can eHealth improve care for people with multimorbidityin Europe?Contents pageKey terms / Key messages 7Executive summary 9Policy brief 11Introduction 11Findings 12Discussion 18Conclusions 19References 20Appendix 1 24Appendix 2 24EditorsErica Richardson Ewout van GinnekenSeries EditorErica RichardsonAssociate EditorsJosep Figueras Hans Kluge Suszy Lessof David McDaid Elias Mossialos Govin PermanandManaging EditorsJonathan North Caroline WhiteAuthorsFrancesco Barbabella, Research Fellow, Centrefor Socio-Economic Research on Ageing, NationalInstitute of Health and Science on Ageing (INRCA),Italy; Researcher, Department of Health and CaringSciences, Linnaeus University, SwedenMaria Gabriella Melchiorre, Senior Researcher,Centre for Socio-Economic Research on Ageing,National Institute of Health and Science on Ageing(INRCA), ItalySabrina Quattrini, Senior Researcher, Centre forSocio-Economic Research on Ageing, NationalInstitute of Health and Science on Ageing (INRCA),ItalyRoberta Papa, Statistician, Centre for SocioEconomic Research on Ageing, National Instituteof Health and Science on Ageing (INRCA), ItalyGiovanni Lamura, Director, Centre for SocioEconomic Research on Ageing, National Instituteof Health and Science on Ageing (INRCA), ItalyISSN 1997 – 8073This report arises from theInnovating care for people withmultiple chronic conditions inEurope (ICARE4EU) project,which has received fundingfrom the European Union, inthe framework of the HealthProgramme. The authorswish to thank all countryexpert organizations and theprogrammes which participatedin the ICARE4EU project. Theauthors are grateful to theprogramme managers forsharing information on theirprogrammes.The authors and editors are alsograteful to Julia Wadoux (AGEPlatform Europe), StephanieCarretero-Gomez (Joint ResearchCentre, Institute for ProspectiveTechnological Studies (IPTS)) andClayton Hamilton (WHO RegionalOffice for Europe) for reviewingthis publication and contributingtheir expertise.
Policy briefWhat is ICARE4EU?The Innovating care for people with multiple chronic conditionsin Europe (ICARE4EU) project aims to improve care for people withmultiple chronic conditions (multimorbidity) in European countries(www.icare4eu.org). An estimated 50 million people in Europe livewith multimorbidity. The complex health problems of these peopleand their need for continuous and multidisciplinary care pose agreat challenge to health systems and social services. From a patientperspective, improvements in, for example, the coordination ofcare and patients’ own involvement in the decision-making and thecare process are also important. ICARE4EU describes and analysesinnovative integrated care approaches for people with multiplechronic conditions in Europe. By disseminating knowledge aboutinnovative care programmes or practices, the ICARE4EU projectaims to contribute to the improved design, wider applicability2and more effective implementation of integrated care for peoplewith multimorbidity. Observations from the ICARE4EU project aredescribed in five policy briefs and key elements of multimorbiditycare are addressed from the following perspectives: patientcentredness [1], use of eHealth technology (this policy brief),integration [2] and financing systems [3]. A final policy brief[4] integrates all lessons learned from the ICARE4EU project onhow care in European countries could be improved for theircitizens with multiple chronic conditions.
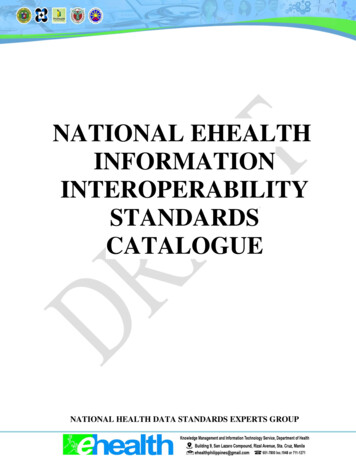
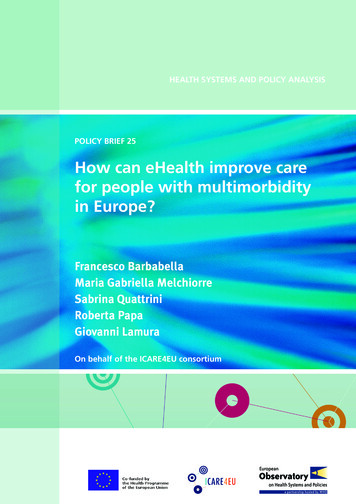
How can eHealth improve care for people with multimorbidity in Europe?How to strengthen patient-centredness in caring for people with multimorbidity in Europe?How do Policy Briefs bring the evidence together?How do Policy Briefs bring the evidence together?There is no one single way of collecting evidence to inform policyThereis noone singleway of collectingevidenceinform policymaking.Differentapproachesare e drawappropriateforofdifferentpolicyissues, soDifferentthe Observatorybriefson a mixmethodologiesissues,so thedraw on thea mixof methodologies(see FigureA)Observatoryand explainbriefstransparentlydifferentmethods used(seeA) andexplainthe allowsdifferentmethodsusedand Figurehow thesehavebeentransparentlycombined. Thisusersto understandandhow thesecombined.the natureand havelimitsbeenof theevidence.This allows users tounderstand the nature and limits of the evidence.There are two main ‘categories’ of briefs that can be distinguishedThereare twomain‘categories’of ofbriefsthatcancanbe bedistinguishedby methodandfurther‘sub-sets’briefsthatmapped anbemapped alonga spectrum:a spectrum: A rapid evidence assessment: This is a targeted review of the A rapid evidence assessment: This is a targeted review of theavailable literature and requires authors to define key terms, setavailable literature and requires authors to define key terms, setout explicit search strategies and be clear about what is excluded.out explicit search strategies and be clear about what is excluded. Comparative country mapping: These use a case study approachComparativecountry mapping:a casestudy withand combinedocument Thesereviewsuseandconsultationapproach icalandcountry reviewsexperts.andThesefall into twoappropriatetechnicalcountryexperts.Thesefall orintotwogroupsdependingon andwhethertheyprioritizedepthbreadth.groups depending on whether they prioritize depth or breadth. Introductory overview: These briefs have a different objective toIntroductoryoverview:These briefsdifferentobjective tothe rapid evidenceassessmentsbuthaveuse aa similarmethodologicalthe rapid evidencea sis targeted butandusereviewedwiththe aim ofapproach. aLiteratureis targetedand reviewed with the aim ofexplainingsubject to‘beginners’.explaining a subject to ‘beginners’.Most briefs, however, will draw on a mix of methods and it is forMostbriefs,thathowever,will drawa mix ofinmethodsand it is forthis reasona ‘methods’boxuponis includedthe introductionthisreasonthatsignallinga ‘methods’box is includedin the introductionto eachbrief,transparentlythat methodsare explicit,toeachbrief,methodsexplicit, robustrobustand signallingreplicable,transparentlyand showingthathowthey areareappropriatetoand replicable and showing how they are appropriate to the policythe policy question.question.Figure A: The policy brief spectrumRapidevidenceassessmentPOLICY g(depth)MultipleCase StudyInstrumentalCase : Erica Richardson33
Policy briefAcronyms4AALActive and Assisted LivingAIMAdvanced Informatics in MedicineCBeHISCross-Border eHealth Information ServicesCCMChronic Care ModelCEFConnecting Europe FacilityCIPCompetitiveness and Innovative Framework ProgrammeCOPDchronic obstructive pulmonary diseaseCVRMcardiovascular risk managementDESIDigital Economy and Society IndexDM2diabetes mellitus type 2DSMDigital Single MarketDSSdecision support systemeCCMeHealth Enhanced Chronic Care ModeleHDSIeHealth Digital Service InfrastructureeHGIeHealth Governance InitiativeEHRelectronic health recordeIDelectronic health identifierEIPAHAEuropean Innovation Partnership for Active and Healthy AgeingEUEuropean UnionGDPgross domestic productGPgeneral practitioner (physician providing general or family medicine)ICARE4EUInnovating care for people with multiple chronic conditions in EuropeICTinformation and communications technologyICUintensive care unitINCAIntegrated CareITinformation technologyOECDOrganisation for Economic Co-operation and DevelopmentPHRpatient health recordPOTKUPotilas Kuljettajan Paikalle (Putting the Patient in the Driver’s Seat) projectSMEsmall and medium-sized enterprisesWHOWorld Health Organization
How can eHealth improve care for people with multimorbidity in Europe?Boxes, figure and tablespageBoxes Box 1:What is eHealth? Box 2:Methods 13Box 3:Types of eHealth solutions for multimorbidity care 16Box 4:TeleRehabilitation (Nicosia General Hospital, Cyprus) 18Box 5:Chronic Care Strategy (Valencia Region, Spain) 18Box 6:INCA programme (Netherlands) 19Box 7:EU funding for research and innovation on eHealth 1913Figure Figure 1: Types of care and support provided by programmesfor multimorbidity care with at least one eHealth tool(%, multiple answers were possible) 15Tables Table 1: General characteristics of the programmes formultimorbidity care with at least one eHealth tool 14Table 2: Types of eHealth tools used in the programmes formultimorbidity care 16Table 3: Framework of eHealth solutions for multimorbidity care andenvisaged benefits 17Table 4: Current policies on eHealth at EU and national levels andrelated gaps 205
Policy brief6
How can eHealth improve care for people with multimorbidity in Europe?Key termsKey messages eHealth is an umbrella term that covers a wide range ofhealth and care services delivered through informationand communication technologies (ICTs), such aselectronic health records (EHRs), health informationsystems, remote monitoring and consultation services(e.g. telehealth, telemedicine, telecare), tools for selfmanagement, and health data analytics. eHealth has the potential to improve care and offer newservices for people with multimorbidity. It could allowproviders and policy-makers to: mHealth is a subset of eHealth that is linked to mobiletelephony and applications. Multimorbidity means having multiple chronicconditions at the same time and (typically) complex needsthat require the involvement of several care providers. Itis a significant and growing challenge to Europe’s healthsystems, with some 50 million people already affected. coordinate and integrate different elements of carebetter, by improving communication and the sharingof information between professionals and withpatients through message systems or electronic EHRs; support self-management through tools to providefeedback or check adherence to treatment; improve clinicians’ decision-making and the quality ofcare through decision support systems (DSSs), whichhelp share evidence on dealing with the complexitiesof multimorbidity; monitor and analyse risk to identify the most complexcases and allow proactive responses; improve access to health care services for people withmultimorbidity in rural and deprived areas throughtelehealth services or mHealth applications. eHealth is not yet a major component in most healthsystems. If it is to fulfil its potential, policy-makers need toaddress gaps in regulation and increase standardization inthe national and European contexts. This means: designing adequate legal and funding frameworks; defining standards for and regulation oninteroperability of eHealth solutions for remoteconsultation, monitoring and care; fostering standardization of DSSs by care providersat the national level; promoting new regulations and frameworks formobile health solutions for self-management,resolving the uncertain legal status; implementing personal health records that areaccessible to patients; refining and implementing a concrete road map forcompatibility and standardization of EHRs, e-referrals,ePrescriptions and health information systems withinand between EU Member States. Concrete initiatives to extend professional and patientuptake might usefully include personal health records,DSSs and information systems for risk stratification. Comprehensive training and educational campaigns willbe important in improving the digital health literacy ofpatients, informal carers and care professionals. Large-scale studies are needed to evaluate the impactof eHealth tools (rather than small-scale research, whichcannot evaluate effectively).7
Policy brief8
How can eHealth improve care for people with multimorbidity in Europe?Executive summaryThe policy issue: the added value of eHealth forpeople with multimorbidityCare for people with multiple chronic conditions(multimorbidity) requires integrated and patient-centredapproaches to adequately meet patient needs. Informationand communication technology (ICT) applied in the healthcare sector (eHealth) constitutes a recognized driver ofinnovation and improvement in providing tailored andinnovative care services to people with complex care needs.Despite the growing investment and interest in eHealth,there are challenges ahead for allowing a wider andmore systematic adoption of ICT in the health caresector. This policy brief synthesizes available evidence onthe implementation, benefits and policies related to theadoption of eHealth solutions for integrated care for peoplewith multimorbidity in Europe.ImplementationThe situation for the implementation of eHealth in termsof the availability of ICT infrastructure, services and skillsis still quite varied across Europe. For example, although27 out of 47 countries in the World Health Organization(WHO) European Region have a national electronic healthrecord (EHR) system in place, the majority of hospitals in theEuropean Union (EU) and Associate Countries (90%) do notpermit patients to access their own health data and only 9%provide any kind of telemonitoring service, with a similarpercentage of general practitioners (GPs) having access totelehealth services (10%).Of the 85 innovative programmes for multimorbidity careusing at least one eHealth tool selected by the ICARE4EUproject, almost half were already integrated into the healthcare system but the scale remained mostly local and/orregional (78%). The main types of eHealth solutions in theprogrammes were EHRs (71%), professionals’ databasesof patient data (64%) and ICT-based communicationbetween care providers (47%), whereas no more than onethird of the programmes has adopted the other types ofeHealth tools.BenefitseHealth solutions for multimorbidity care provide thefollowing benefits: Improving access to health care services: especially inrural and deprived areas with low (or no) availability ofhealth care services, eHealth tools can enable remoteconsultations, therapies and rehabilitation. Enhancing care coordination and integration: eHealthsolutions can help with collecting, storing and reportinghealth data to professionals and to patients via EHRsand patient health records (PHRs). eHealth tools can alsoimprove communication between these actors throughsystems for messaging and audio-visual communication. Enabling self-management: supporting people withmultimorbidity living at home includes tools that educateand empower them in self-care. Self-management toolscan provide feedback and support patients by checkingtheir coping behaviours and adherence to treatment. Supporting decision-making by clinicians: decisionsupport systems (DSSs) can link available clinical evidenceon appropriate treatments and best practice for thecomplex profile of people with multimorbidity, improvingthe quality of care provided. Enabling monitoring, risk analysis and proactiveintervention: an information system for risk stratificationcan monitor and predict health risks in a population, aswell as indicating recommended strategies for prevention,monitoring and treatment.PoliciesThe potential of eHealth for multimorbidity care is notyet sustained in a systematic and explicit way by currentpolicies. At the EU level, the issues of chronic care andmultimorbidity, together with personalized health careand intelligent environments within the eHealth sector,have become a policy priority only with the eHealth ActionPlan 2012 – 2020. Previously, the EU policy focus was onstimulating the general development and implementationof EHRs and health information networks to enable andimprove health data exchange between different careproviders and nations.At national level, there is increasing interest in dedicatingattention to eHealth in general, but there is a mixed impactat the operative level. There is the risk that, in some cases,policies are just symbolic and aimed at complying withcurrent international policy trends, but with marginaleffects in terms of the actual design, development andimplementation of eHealth services.Policy implicationsTo encourage the improvement of care for people withmultimorbidity through eHealth in European health systems,policies need: to refine and implement a concrete road map forachieving compatibility and standardization of EHRs,e-referrals, ePrescriptions and health information systemswithin and between EU Member States; to foster personalized medicine services throughenhanced EHRs and electronic health identifiers (eIDs)which can enable and realize PHRs for use by patientsthemselves; to identify key public health priorities for people withmultimorbidity nationally and support the scaling upof remote consultation, monitoring and care services; to define common public health objectives acrossEU Member States for different profiles of peoplewith complex care needs and regulate jointly oninteroperability and requirements of eHealth solutionsfor remote consultation, monitoring and care; to foster the awareness, standardization and adoptionof DSSs by care providers at national level;9
Policy brief to promote the awareness, standardization and adoptionof information systems for analysing the risk stratificationof populations at regional and national levels; to plan new promotion campaigns to encourage patients,informal carers and health professionals to improve theirdigital health literacy; to dedicate innovation, research and development funds,and design new regulations in the field of mHealthsolutions in order to increase their opportunities andmitigate their risks; to privilege the allocation of research funding tolarge-scale studies and trials aimed at verifying theeffectiveness, efficiency and impact of eHealth solutionsfor people with multimorbidity.10
How can eHealth improve care for people with multimorbidity in Europe?Policy briefIntroductionThe challenges related to the increasing number of peopleliving with multiple chronic conditions – multimorbidity – arewell-known. Over 50 million people in the EU have multiplechronic conditions [6] and around 60% of people aged 65years and over are estimated to live with multimorbidity [7],with major consequences such as functional impairment,lower quality of life and higher health care utilization andcosts [8,9].Multimorbidity is associated with a higher number ofprimary care consultations, hospital outpatient visits andhospital admissions, which increases the workload of healthcare staff [10,11]. However, national health care systemsin Europe are not designed to adequately meet the careneeds of people with multimorbidity, as care services arestill fragmented and oriented to managing single diseasesinstead of complex conditions [12]. There is a risk thatpeople with multimorbidity may receive inadequate care,which can then have a negative impact on their health andquality of life, as well as the health and quality of life of theirinformal carers.New opportunities enabled by the application andexploitation of ICTs in the health care sector couldsubstantially improve patient-centredness and careintegration, which are both fundamental aspects ofmultimorbidity care. As widely recognized [5,13–16],eHealth is a driver of innovation and leads to several benefitsfor people with chronic conditions and multimorbidity,care professionals, and the health and social care systems.It contributes to several key opportunities for Europeansocieties, including: a more personalized ‘citizen-centric’health care [5]; empowering patients to become moreindependent and able to self-manage their conditions,where possible; overall quality of life of patients and theirfamily carers; effectiveness and efficiency of care systemsthrough the optimization of resources and indirect benefitsfrom more appropriate care.Furthermore, in terms of social inclusion and equality,access to health care services can be harder for peoplewith lower socioeconomic status, for a variety of reasonsincluding unaffordability and residence in deprived areaswhich also have a lack of infrastructure, typically associatedwith the presence of multiple chronic conditions [17,18].ICTs can help improve accessibility through, for example,the implementation of telehealth services for remoteconsultations and monitoring [19–21]. In addition, severalsocial and economic benefits for health care systems andwelfare states have been noted. For instance, just thesystematic adoption of mobile Health (mHealth) solutionsin the EU would allow: saving 99 billion in total annualhealth care expenditure; extending the professional livesof more than 11 million people with chronic diseases; andincreasing the general domestic product (GDP) of the EUby 93 billion [22].Box 1: What is eHealth?eHealth has been defined by the European Commission as “theuse of ICT in health products, services and processes combinedwith organizational change in health care systems and new skills,in order to improve health of citizens, efficiency and productivityin health care delivery, and the economic and social value ofhealth” [5].Box 2: MethodsFor policy-making, insights from practice and from scientificliterature are useful and provide information on health carechanges, which can lead to more patient-centred, integratedcare. Therefore, this policy brief combines a rapid review of theresearch literature with results from a survey conducted within theICARE4EU project (see Appendices 1 and 2). The literature reviewfocused on identifying publications on the adoption of eHealthand ICT for chronic or multimorbidity care. Under the ICARE4EUproject, information was gathered on 101 innovative programmesin 24 European countries, eight of which were visited to obtain amore in-depth understanding of the particular characteristics ofthese programmes and to produce case study reports. Appendix 2provides detailed information on this research into innovative carepractices in European countries.eHealth is actually an umbrella term that includes a widerange of ICT solutions (see Box 1). Overall, it is estimatedthat the global eHealth market will be valued at around 280billion by 2022 [23], with a growing and consistent segmentin the EU. For mHealth solutions alone in Europe, this marketis projected to grow from 0.6 to 6.4 billion in the period2013–2018 [24]. eHealth is a key sector for the digitalizationprocess in the digital economy and society according to theEU Digital Single Market (DSM) Strategy [25,26], reinforcedalso by recent priorities in the New Skills Agenda [27] andDigitalising European Industry strategy [28].Despite the potential of eHealth, both in general and formultimorbidity care, there are challenges in allowing a widerand more systematic adoption of ICTs in the health caresector. Indeed, the progress of eHealth implementation, ingeneral but especially for multimorbidity care, is still quitelimited in the EU [16,29,30].Therefore, this policy brief aims to deepen and disseminatethe available knowledge about the implementation, benefitsand policies related to the adoption of eHealth solutions forintegrated care for people with multimorbidity in Europe.Policy-makers at EU, national and local levels can use thisbrief to promote eHealth for people with multimorbidityand to inform adequate development and implementationstrategies. Furthermore, care professionals, non-profitorganizations, companies and any other stakeholderworking with people with multiple chronic diseases andICTs can get new insights into the current state of eHealthin Europe.11
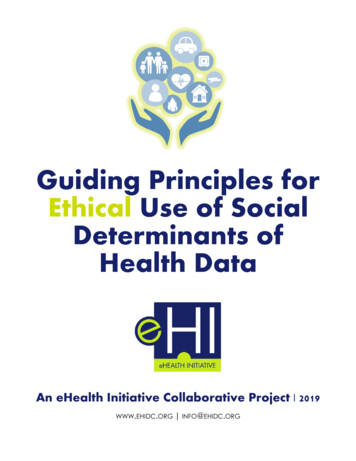
Policy briefPolicy questionsThis Brief focuses on the specific policy question: How caneHealth improve care for people with multimorbidityin Europe? It presents relevant findings in the field,including programmes with high potential, and highlightscurrent policies in the field. Three main sub-questionswere identified:1. Implementation: What eHealth solutions are availablefor people with multimorbidity?2. Benefits: What are the positive outcomes of eHealthsolutions for people with multimorbidity?3. Policies: What are the current policies concerning theadoption of eHealth for people with multimorbidity?Each sub-question is explored in the Findings through ananalysis of available evidence and information collectedfrom various sources (see Box 2).FindingsImplementation of eHealth solutions for peoplewith multimorbidityEven if access to and the use of digital technologies bycitizens is improving across the EU, national contexts are stillquite different in terms of availability of ICT infrastructure,services and skills among populations. The Digital Economyand Society Index (DESI) 2016 [31] shows that MemberStates are moving forward in the digitalization of publicservices (including eHealth), but the variation betweencountries is still wide (the index ranges from 0.331 inBulgaria to 0.866 in Estonia, where 1 would be a perfectscore) and EU countries are at very different stages of digitaldevelopment.This situation is well reflected in eHealth, where MemberStates have adopted different implementation strategies.Available data indicate that general eHealth services (notspecific to multimorbidity care) are not yet systematicallyemployed. According to data from a recent survey (2015)involving 47 countries in the European region [16], EHRswere the most widespread and well-established tools, with27 countries (59%) saying a national EHR system is in place,with around half of these working across both primary andsecondary care facility networks. Telehealth programmeswere implemented in the health care sector at nationalor international level in half of the countries, while therewas a growing interest in mHealth services sponsored bynational governments (22 countries), with most of theseservices already established at a national level (mainlyproviding access to emergency lines, health call centres,health information and EHRs). However, information systemsfor risk stratification, which analyse big data sets at thepopulation level, were not yet developed and could not bemapped, revealing that health data analytics is still in itsinfancy in Europe.Furthermore, in 2012–2013, 41% of hospitals in Europewere halfway between a fully paper-based non-digitizedenvironment and an electronic, paperless environment,12Table 1: General characteristics of the programmes formultimorbidity care with at least one eHealth toolAll programmesn 85Integration levelSmall-scale (pilot) programmeWell-established and comprehensive programmeFully integrated in the health care systemOperational levelOnly at level of daily patient careOnly at level of policy / managementBoth at policy / management and patient care levelImplementation levelLocalRegionalLocal / regional, as part of a national programmeNationalNational, as part of an international programmeInternationalGeographical coverageOnly ruralOnly urbanBoth rural and urban areas26%29%45%34%4%62%26%34%18%13%6%4%5%13%82%and over 80% had an EHR system [32,33]. Almost 80%of the hospitals surveyed were online, 57% had a formalstrategic information technology (IT) plan, and almost 50%had videoconferencing facilities. However, most of thehospitals (63%) alloca
systems, remote monitoring and consultation services (e.g. telehealth, telemedicine, telecare), tools for self-management, and health data analytics. mHealth is a subset of eHealth that is linked to mobile telephony and applications. Multimorbidity means having multiple chronic conditions at the same time and (typically) complex needs