Transcription
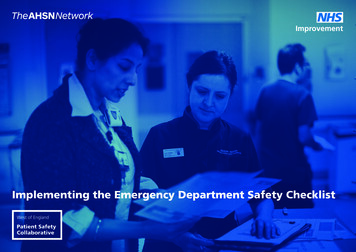
Implementing the Emergency Department Safety Checklist
IntroductionAcknowledgementsThis toolkit has been based on the ED Safety Checklistand Key Performance Indicators developed and tested byUniversity Hospitals Bristol NHS Foundation Trust (UH Bristol)and the West of England Patient Safety Collaborative.Adoption and spreadWe would like to thank the team at UH Bristol for theirwork in the development of this project. University Hospitals Bristol NHS Foundation Trust North Bristol NHS Trust Royal United Hospitals Bath NHS Foundation Trust Great Western Hospitals NHS Foundation Trust Gloucestershire Hospitals NHS Foundation Trust Weston Area Health NHS Trust South Western Ambulance Service NHS Foundation TrustThe UH Bristol pilot scheme was funded by the HealthFoundation SHINE Innovation programme.The safety checklist has been adopted by all six hospital trusts and the ambulance service in theWest of England, who comprise the Emergency Department Collaborative:Roll out to these other Emergency Departments was financially supported by the West of EnglandPatient Safety Collaborative.The ED Safety Checklist won Best Patient SafetyInitiative in A&E award at the 2017 PatientSafety Awards.NIHR CLAHRC West, now recommissioned as the NIHRApplied Research Collaboration West (ARC West), havecompleted an independent evaluation of the ED checklist.This toolkit has been updated in August 2019 to incorporateevidence-based recommendations from their evaluation.The judges felt that this entry had a significant impact onpatient safety in period of crowding in ED. It has alreadyspread across multiple organisations and using establishedtools has potential for wider spread across the UK.2
IntroductionAimThis toolkit supports the implementation of theED Safety Checklist and gives advice and guidanceon achieving a successful implementation in youremergency department.This toolkit also provides information and links toresources on change management methods.Supporting documents and resources are available atwww.weahsn.net/ed-checklistWho this document is forThis guide is for clinical teams in the emergencydepartment, consultants, nurses, quality andsafety leads and operational managers as wellas ambulance staff.LicenceTraining materials and supporting resources are West of England Academic Health Science Network2017, and provided under licence for use under the following terms: Attribution — You must give appropriate credit, provide a link to the licence, and indicate ifchanges were made. You may do so in any reasonable manner, but not in any way that suggeststhe licensor endorses you or your use. Non-commercial — You may not use the material for commercial purposes. Share alike — If you remix, transform, or build upon the material, you must distribute yourcontributions under the same licence as the original. No additional restrictions — You may not apply legal terms or technological measures thatlegally restrict others from doing anything the licence permits.This work is licensed under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0International Licence. To view a copy, visit http://creativecommons.org/licenses/by-nc/4.0/or send a letter to Creative Commons, PO Box 1866, Mountain View, CA 94042, USA.This document is version 5.1 September 20193
About the West of England Patient Safety CollaborativeEngland’s 15 Patient Safety Collaboratives play anessential role in identifying and spreading safercare initiatives from within the NHS and industry,ensuring these are shared and implementedthroughout the system.The Patient Safety Collaboratives are coordinatedby the 15 Academic Health Science Networks andthey are part of the national patient safety programme,with a mandate to create a culture of continuouslearning and improvement in the e West of England Academic Health Science Network(AHSN) is based in Bristol and is one of 15 AHSNs acrossEngland, established by NHS England in 2013 to spreadinnovation at pace and scale. As the only bodies thatconnect NHS and academic organisations, the thirdsector and industry, AHSNs are catalysts that createthe right conditions to facilitate change across wholehealth and social care economies, with a clear focuson improving outcomes for citizens.Find out about more about the work of the AHSNNetwork at www.ahsnnetwork.com.Find out more about the West of England AHSN atwww.weahsn.net and follow us on Twitter @WEAHSN.SwindonBathSalisburyWest of England Academic Health Science Network MapBristol, North Somerset and South Gloucestershire STP (Healthier Together)Bath and North East Somerset, Swindon and Wiltshire STPGloucestershire ICS ( One Gloucestershire)4
About the Emergency Department Safety ChecklistThe aims of the Emergency Department (ED) Safety Checklist are to standardise and improve the delivery of basic care in EDs, to improve resilience in EDs during periods of crowding,to improve the safety and clinical outcomes for patients accessing the emergency care system, and to improve ED performance against Best Practice Tariffs.What is the ED Safety Checklist?An ED Safety Checklist is a time based framework oftasks that is completed for every patient, other thanthose with minor complaints.The ED Checklist is a resource for all clinical staff inthe ED but will most likely be completed by nursingand nursing support staff, temporary/bank nursingstaff and nursing supervisors.Best Practice Tariffs and early triggers to specific carepathways such as sepsis are included.What is the evidence base for theintervention?At University Hospitals Bristol NHS FoundationTrust (UH Bristol) the mean proportions in KeyPerformance Indicators (KPI) taken before and afterthe introduction of the ED Safety Checklist improvedin 5%-25% in most cases.Quality improvements the checklistaims to achieve:Crowding has a profound impact on the ED’s abilityto deliver safe care. Delays in recognition and treatment of severe illnessare common, with associated poor outcomes. This isparticularly problematic for patients suffering fromstroke, heart attack and sepsis. What is the problem we are tryingto address?Improved baseline clinical careLess clinical incidentsMore efficient handoverMore efficient documentationImproved performance against best practice tariffDecrease avoidable harm by recognisingdeteriorationEnhanced safety region-wideImproved communicationImproved team moraleImproved patient and staff feedbackA scarcity of staff in the ED workforce has resultedin a reliance on agency and non ED-trained staff.Human factors - as staff become overwhelmed bythe tasks they need to complete in a timely fashionand with constant interruption.5
Case study - University Hospitals Bristol NHS Foundation TrustOvercrowding has an impact on the ability of staff inthe ED to deliver safe care. Delays in recognition andtreatment of severe illness are common, with associatedpoor outcomes. This is particularly problematic forpatients suffering from stroke, heart attack and sepsis.Staffing challenges in the ED workforce have resultedin a reliance on agency and non ED-trained staff. Asstaff become overwhelmed by the tasks they needto complete while faced with constant interruptionsthere is a risk of omissions in the delivery of basic careelements, which contributes to harm and difficulty inidentifying the deteriorating patient in a crowd.The impactUH Bristol’s performance was analysed against similarbaseline data. After the introduction of the ED safetychecklist, performance against baseline increased witha p-value of 0.0001 in most cases.Quantitative improvements Improved management of time-critical conditions,UH Bristol saw a mean increase of over 5% in CTscanning within one hour for suspected strokes.Earlier recognition and rescue of clinicallydeteriorating patients. UH Bristol saw a meanincrease of 25% in hourly observations and earlywarning score calculations.Ensuring patients are on the correct carepathways out of EDs. UH Bristol saw an 11%increase in patients treated on the strokepathway.Since the introduction of the ED Safety Checklist atUH Bristol there have been no clinical incidents relatedto failure to recognise deteriorating patients or delayin care delivery. This can be compared with the winterprior to implementation when there were five seriousincidents due to failure to recognise deterioration,three of which were in the ambulance queue.“International evidence, highlighted in the‘Keogh Review’ of Urgent and EmergencyCare clearly demonstrates the risks thatcrowded EDs pose to patient safety andoutcome.Safety checklists have been shown to improvestandardisation and demonstrate improvementsin patient safety and care. The team at UH Bristoldeveloped the ED Safety Checklist. Following a period of development and testing,including input from public and patient representatives,the ED Safety Checklist was introduced to the UHBristol adult ED in November 2014.Qualitative improvementsProfessor Jonathan Benger, National ClinicalDirector for Urgent Care, NHS England Key contactsAt UH Bristol the checklist is used for every ‘major end’patient coming into the adult ED - a footfall of almost14,000 patients every year. Reduced length of hospital stay.Better supported staff, including those lessfamiliar with the ED and ambulance crews.Improved quality of handover.Appropriate continuity of care.“This intervention is designed to directlyaddress these challenges, and hasalready been shown to be effective: it isentirely consistent with national policy inemergency care.”Dr Emma Redfern, Consultant in EmergencyMedicine, University Hospitals Bristol NHS FoundationTrust, emma.redfern@uhbristol.nhs.uk6
Case study - West of England Emergency Department CollaborativeUniversity Hospitals Bristol NHS Foundation Trust(UHB) was funded by the Health FoundationSHINE innovation programme in 2014 to introducea Safety Checklist in the Emergency Department(ED). Since April 2016, the West of EnglandAcademic Health Science Network (AHSN) hasworked to support all six Trusts across the Westof England region to introduce the ED SafetyChecklist across seven ED’s.The Checklist was piloted in UHB on November 2014and achieved demonstrable success in improvementin patient safety during periods of crowding. Thisincluded the support and cooperation from the SouthWestern Ambulance Service NHS Foundation Trust whoprovided a National Early Warning Score (NEWS) viatheir Electronic Patient Care Record System and initiatedthe ED Safety Checklist if managing patients in queueswaiting to transfer to ED.Following the Institute of Healthcare Improvementmodel, an implementation toolkit was developed usingthe lessons learnt from the pilot site to support Trustsintroduce the ED Safety Checklist in their department.An inaugural regional ED Collaborative meetingtook place in May 2016 with a primary focus ofimplementing the ED Safety Checklist. These were heldmonthly and were an opportunity to regularly sharelearning and discuss issues.Learning from implementation:Challenges:Benefits: Cost of colour printing or photocopying of theChecklist Continued departmental pressures, as well assometimes high use of agency staff and high staffturnover Initialling of the Checklist by staff (this was overcomeby explaining the importance of the Checklist andits ability to enable patient safety) Proven to be a useful tool in answering complaintsand providing a safety net for staff Increased regular contact with patients and familyleading to improved patient satisfaction Provides structure in times of overcrowding to alloweffective timely treatment Faster transitions for some patients through ED An objective tool to communicate concern using astandardised language Better recording of pain management andreassessment Improved recognition of sepsisCulture: Checklist is a tool to support patient care anddeterioration – it doesn’t take away decisionmaking or clinical judgement Continuous feedback to staff on progress and areasfor improvement Identify a Checklist champion to driveimplementation Feedback to champion with regards to staffmembers for additional trainingFor more information and resourcesto help support implementation, pleasego to www.weahsn.net/ED-ChecklistChecklist: More successful when included in observationbooklet/with original notes Clear guidance for escalation to doctors/othercolleagues/services Edit the Checklist as necessary to be in line withlatest hospital policies/guidance Standard of care and documentation is clearly set out Some of the Trusts are noting on the Checklist if thepatient is being monitored in the queue/corridorby adding a Q to the ChecklistAuditing: Data analyst role is key to the implementationof the Checklist and evidence its success by beingable to monitor it regularly Checklists need to be at least 50% completedto be audited Staff are to initial when completed, along withtime and ‘n/a’ if necessary Clear Key Performance Indicators (KPI) measured7
About the Emergency Department Safety ChecklistThe ED Safety Checklist is a simple time-based framework of nursing and medical tasks. The checklist systemises the observations, tests and treatments required by patients in a timebased sequence. This makes it clear what has been done and what needs to be done next. The checklist serves as an aide-memoire for busy staff. Any doctor, nurse, bank or agencystaff can join the department and provide the right care. By providing this structure, the checklist results in improved outcomes for patients and a reduction in system risk.The ED Safety Checklist is structured into two parts:Part 1 - Provision of basic safeclinical careA time-based framework for vital sign measurementand calculation of the National Early Warning Score(NEWS2), pain scoring, administration of drugs andfront-loading investigations.Part 2 - Value added tasksInclude referrals to drug and alcohol services, liaisonpsychiatry and occupational therapy.Commencement of pathways that demonstrablyimprove outcomes (e.g. fractured neck of femur,stroke and diabetic ketoacidosis).Our experience has shown that the Phase 2 valueadded tasks only improved after Phase 1 (basic clinicalcare) was well embedded.Best practiceThe ED Safety Checklist needs to work for your EDand be specifically structured to account for yourTrust specialisms, your local demographic and otherenvironmental factors. Each implementing ED willneed to assess what should be included in their EDSafety Checklist. It is suggested that a comprehensivereview of ED clinical incidents should be carried outto inform these decisions prior to PDSA testing of theED Safety Checklist.However, the recommendations for best practice fromthe Royal College of Emergency Medicine are: Vital signs taken and NEWS2 calculated regularly.Front loading of investigations i.e. imaging,bloods etc.Pain reliefTherefore, it is our strong recommendation that theseelements are included as mandatory fields. KPI datawill be driven by the fields in the checklist and will beunique to each ED.8
Implementing the ED Safety Checklist in your organisationThe processes we describe can be adapted to meet theneeds of your staff, service users and organisationalcontext. Our approach uses the methodology developedby the Institute of Health called the IHI Model ofImprovement.Plan, Do, Study, Act is an effective methodthat helps teams plan the actions for theirmodel, test it on a small scale, and review beforedeciding how to continue.Using PDSA cycles are a fantastic way of takingideas, trying them in practice, learning whatworks, and what doesn’t to help you achievesuccess.ANFor a fun way to introduce a team to qualityimprovement, check out this blog postwww.weahsn.net/2016/01/anyone-for-tennis/What changes can we make thatwill result in an improvement?PLYou can then broaden the scale of the test, oradjust your ideas through more than one PDSAcycle — it make take a few before the idea startsto work reliably.How will we know if a changeis an improvement?YUDFor an introduction to PDSA cycles watch this videohttps://youtu.be/xzAp6ZV5ml4These are then followed by rapid cycleimprovement using PDSA.STYou can find out more about the Model forimprovement through the MINDSet qualityimprovement toolkit. Although aimed at peopleinvolved in providing and commissioning services forpeople with mental health projects, it is an excellentresource for practical quality improvement guidance.Available at http://mindsetqi.net/ as a PDF to download.There are three questions to ask when developingimplementation projects shown to the right.What are we trying toaccomplish?DOQuality Improvement science is the application ofa systematic approach using specific methods andtechniques in order to deliver measurable improvementsin quality, care and safety.The IHI Model for ImprovementACTIn order to implement the ED Safety Checklist in asustainable way in your organisation, and to be able tomeasure the impact of this intervention, we recommenda structured Quality Improvement framework forimplementation.9
Project logic model in the West of England Patient Safety CollaborativeOvercrowding in emergency departments is widespread and is associated with clinically significant delays to diagnosis, recognising deterioration and treatment.Omissions in basic clinical care are common during crowding. Checklists have been shown to improve standardisation and reliability in the delivery of healthcare.InputsExisting UH Bristol SafetyChecklistChecklist implementationtoolkitLearning from West of EnglandCollaborativeSWAST (Ambulance Service)perspective and expertiseCentral clinical teamProgramme faculty supportWest of England Patient SafetyCollaborative supportNational Institute for HealthResearch Collaboration forLeadership in Applied HealthResearch and Care WestevaluationActivitiesDevelop and refine genericimplementation toolkit including educational material,data collection and dashboardRecruit local implementationteams.Implement ED Safety Checklistin all regional EDs andambulance service.Host masterclass for nationalinterested parties.Make toolkit and all resourcesavailable via West of EnglandAcademic Health ScienceNetwork website.OutputsOutcomesTeam dashboardsImproved baseline clinical careTeam risk and issues registersFewer clinical incidentsRegional dashboard (LifeSystem)More efficient handoverRegional risk and issues registerCommunication Strategy- including programmecommunication networks,tools, and Learning Set eventsMore efficient documentationImproved performance againstbest practice tariffImpactDecrease avoidable harm byrecognising deteriorationEnhanced safety in all adaptingEDsImproved communicationImproved team moraleImproved patient and stafffeedbackEvaluation data and analysesProject reports and publishedoutputsDisseminiation activitiesYou may find it helpful to adapt this logic modelto your local implementation of the ED checklist.Royal College of EmergencyMedicine support10
Role descriptionsEach ED will need to appoint individuals to specific roles within each Local Implementation Team. It is a strongly suggested that these roles are fulfilled by staff already in post workingin the EDs, not staff brought in for the specific functions/roles outlined in this Toolkit. In order to release people to complete the roles specified in this Toolkits, a commitment must begiven by the Trust to backfill the individuals undertaken them.Lead NurseLead ConsultantAudit Coordination Nurse / Data Analyst Providing day to day nursing leadership to theProjectAgree quality metrics for measurement (clinical andoperational) to assess impact of project with LeadConsultantEducating ED staff on the project aims,methodology and anticipated patient safety impact,by a full range of communication methods andbriefing sessions.Delivering appropriate training and staff briefingsessions.Champions of the project on the shop floorEnsuring regular feedback results to all staff groupsPresenting information in a variety of formatsCoordinate regular meetings with Project Teamto discuss project progression and action plan/delegation of responsibilitiesTarget specific staff groups according to theirinvolvement in the project (ED admin staff, clinicalsite managers)Liaise with trust data analysts to present dataeffectively and professionallyWrite and present reports as required Providing day to day medical leadership to theProjectAgree quality metrics for measurement (clinicaland operational) to assess impact of project withLead NurseProvide education support in all aspects of theproject, but with specific emphasis on medical staffat all levels and consultant colleagues.Champions of the project on the shop floorPresenting project information and results ina variety of formatsTarget specific staff groups according to theirinvolvement in the project (CSMs)Write and present reports as required Collecting and collating agreed metricsReview retrospective data to enable comparisonof current resultsManaging supporting staff involved in auditingLiaise with trust data analysts to present dataeffectively and professionallyContribute and present data results to project groupand wider audienceOther key stakeholdersSenior Medical & Nursing Team – need to entrustcommitment to project and be a champion on shopfloorData Analyst needs to be on board and prepared toassist project with data production and presentationReceptionist/Patient Flow Coordinators needs tobe on board and understand their contribution as perlocal procedures11
Form your local implementation teamWe recommend that each team makes time for fortnightly meetings to discuss the progress of the ED Safety Checklist implementation, to ensure the practicalities of the projectare being addressed, staff are being supported, messages are being appropriately disseminated and to review site data to track progress. We have provided a generic agenda,which you may find helpful to facilitate these fortnightly meetings. Please feel free to tailor this to your specific team.Project documentationTiming of implementationHousekeepingIt is recommended that each team maintain aRisk & Issue Log for the duration of the project.We recommend that you consider the timing of theimplementation of the ED Safety Checklist.Review of the practicalities required tointroduce the ED Safety Checklist, such asprinting etcOnce you have your aim agreed, as a team, considerwhat risks and issues may prevent you from achievingyour aim.DataAn issue is something that is happening. A riskis something that might happen. Please use yourown organisational risk management scoring forlikelihood and impact of risks occurring.In most EDs, winter crowding puts significantoperational pressures on staff at all levels. Therefore,it would be sensible to commence the implementationproject during periods when crowding is not asprevalent and staff have capacity to be releasedfrom their shop floor responsibilities.LIT fortnightly meeting agendaReview of current dataDashboardMeasurement strategyStaffThe status of a risk can be open (action required),accepted (all mitigation in place, no action required),closed (risk or issue has been closed).Nursing and medical staffPioneers and laggardsPeer supportRisk & issue logCommunications & education12
Organise your Emergency DepartmentConsider how you will print, store and restock the ED Safety Checklist. Each team will need to consider how this works for their local operational procedures.Photocopy the ED Safety ChecklistInterface with the ambulance trustIf printing in black and white, check the resolutionson all the fields.Patients queuing to offload from ambulance intoED is common. The risk of patients deterioratingin this queue is a significant patient safety issue.Consider what you will do with the ED SafetyChecklist once a patient has been dischargedout of ED.Sites in the West of England Patient SafetyCollaborative found that incorporating the ED SafetyChecklist into the ED notes ‘booklet’ saw an increasein reliability of use of the checklist for all patients.In some departments, this whole booklet getsscanned when the patient is discharged out of thedepartment prior to being filed and/or taken with thepatient to the ward, which helped with monitoringimplementation.Teams should consider engaging with theirAmbulance Trust to agree a Standard OperatingProcedure (SOP) for paramedics to commence theirED Safety Checklist in the queue and as a tool athandover of care.Each team needs to consider how they willincorporate the ED Safety Checklist into their EDnotes and what procedures will put in place forfiling and access for audit.13
Communication and trainingIt is recommended that teams ensure information about the checklist programme, ‘go live’ dates and the wider patient safety benefits of the checklist are communicated not only toED but across the Trust in order to encourage a culture of support and participation in the programme. Teams should consider a communications strategy in advance of ‘go live’ datesvia planned bulletins or within regular communications to both ED and Trust wide staff.ED Safety Checklist trainingReal-time feedbackNational Early Warning Score trainingThis Toolkit recognises that each team will have theirown training methods and structures for training theirstaff in the ED Safety Checklist.To ensure ongoing compliance with the checklistonce implemented and embedded, UH Bristol gavethe Nurse Shift Leaders the responsibility to checkand monitor that the ED Safety Checklist wasbeing completed for all (appropriate) patients andprovide ‘real-time’ feedback and support for thosestaff who were failing to consistently complete theED Safety Checklist.A suggested field of the ED Safety Checklist is that vitalsigns and the National Early Warning Scores (NEWS2)are regularly calculated.For the pilot implementation at UH Bristol the ED SafetyChecklist was introduced during the Bite size TeachingSessions that occur daily at 8am. The emphasis duringthese sessions was on: Culture – ensuring organisational buy-in, especiallysenior nursing and medical staff.Testing – Are the fields in the ED Safety Checklistright for your ED? Do additional fields need adding?Successes and challenges – review of thetesting cycles, the successes and challenges toimplementation.Staff feedback.It is our strong recommendation that each adopting EDidentify on-shift resource to fulfil this role and provideshop-floor support and feedback to staff.The NEWS2 is routinely used in inpatient wards butoften not calculated or tracked in ED or in ambulancequeues. The use of a track and trigger system in theUH Bristol pilot showed demonstrable improvementsto patient safety and quality of care. If teams do notroutinely use NEWS2 it may be worth considering anED training programme to familiarise staff with theaccurate calculation of the score.Feedback during testingDuring your testing of the ED Safety Checklist, you mayfind it helpful to carry out an anonymised staff surveyto see how well the checklist has been received and togather opinion on sections that work and those thatneed improvement. A SurveyMonkey questionnaire maybe good format for this during your study period of aPDSA cycle.14
Case study - evidence informed recommendationsNIHR CLAHRC West, now recommissioned as the NIHR Applied Research Collaboration West (ARC West), evaluated theimplementation and use of the ED Checklist during 2017. The full findings will be available soon in a journal paper buthere are some of their key recommendations for implementation. The evaluation used qualitative and quantitative data.The research interviews and observations conducted by NIHR CLAHRC West identified the value of emphasising theprimary purpose of the tool, involvement and endorsement from senior ED staff, dedicated training time and fullintegration with existing clinical documentation improved its implementation.1. Promoting the clinical purpose2. Obtaining senior staff supportThe research found that the checklist was sometimesseen as an administrative rather than a clinicaldocument which contributed to it being overlookedwhen busy.Obtaining senior ED management supportfrom doctors, managers and senior nursesis crucial to ensuring the ED Checklist becomesintegral to the department’s usual workflow.Promoting the ED Checklist to be clear about itspurpose and rationale for its introduction can help toimplement it effectively. Taking a clear approach toits purpose is better and it should be promoted as:Our research found there was better recognitionand ‘buy in’ to the checklist when it was associatedwith the Department and an implementation teamrather than an individual. A patient safety tool aimed at avoidingundetected patient deterioration A framework to support staff in monitoringpatient care and patient safety in busy anddemanding ED environments3. Training timePlanning dedicated staff training sessions andallowing staff time to train, ask questions andreflect on the checklist was more effectivefor implementation purposes that ad-hoc‘on the job’ training.This allowed a greater scope for communicatingthe purpose of the ED Checklist, how it cansupport patient safety and be integrated into thedepartment’s work processes more effectively.4. Tailoring & integrating theED checklistTo successfully integrate the ED checklist, twoadaptations are necessary:a) The ED Checklist needs to be tailored to yourdepartment’s specialisms/clinical priorities andb) the ED Checklist needs to be formatted andintegrated into the ED paperwork and not justclipped or stapled to itOur research indicates these adaptations will reducethe potential for the ED Checklist to be viewed as‘just another form’ and will encourage smootherimplementation.One trust who has implemented the ED Checklisttook several attempts and trial runs to get to thechecklist they wanted and to get it integrated intotheir c
The aims of the Emergency Department (ED) Safety Checklist are to standardise and improve the delivery of basic care in EDs, to improve resilience in EDs during periods of crowding, to improve the safety and clinical outcomes for patients accessing the emergency care system, and to improve ED performance against Best Practice Tariffs. 5