Transcription
Workforce Development Plan2018Prepared by the Workforce Development Committee: February 1, 2018Approved by the Department Director: February 9, 2018Original Plan Implemented: April 16, 2014 2018 Denver Public Health
Workforce Development Plan - 2018Table of ContentsPurpose and Introduction. 4Introduction . 4Questions . 4Agency Profile. 5Denver Public Health Vision, Mission, and Values . 5Location and population served . 5Governance . 6Organizational structure . 6Funding . 7Workforce policies . 7Communication plan . 7Workforce Profile. 8Current workforce demographics . 8Future workforce . 8Continuing education requirements by discipline . 9Core Competencies for Public Health Professionals . 10Introduction . 10Job classifications and competency selection . 10Competency language and tiers . 11Self-assessment . 11Creating a Learning Culture . 12Training needs assessment results . 13Mandatory and recommended training . 13Training resources . 14Professional development funding. 14Professional development goal setting . 15Travel to conferences . 16Mentorship. 17Evaluation & Tracking . 18Workforce Development Committee. 19Introduction . 19Goals . 19Objectives . 192
Workforce Development Plan - 2018Roles and responsibilities . 20Implementation plan . 21Conclusion/Other Considerations . 21Other agency documents and plans . 21Review of plan . 21Approval of plan . 21Appendix A – DPH Organizational Chart. 22Appendix B – DPH’s 2017 Core Competency Survey . 23Appendix C – Example of Individual Staff Core Competency Results . 41Appendix D – Manager Core Competency Coaching Guide. 46Appendix E – Example of Core Competency Program Data . 51Appendix F – DPH 2017 Core Competency Results (Department Competencies) . 52Appendix G – DPH New Employee Orientation Checklist . 53Appendix H – Workforce Development Committee Charter . 56Appendix I – Professional Development Implementation Plan . 58Appendix J – Health Equity Training Plan . 613
Workforce Development Plan - 2018Purpose and IntroductionIntroductionIn an effort to meet the changing health needs of the community, it will be necessary toexpand our workforce capacity to offer both direct service delivery and population-basedpublic health practice. Denver Public Health (DPH) is fortunate to employ skilled, dedicatedand diverse staff. These individuals, who personify our values, will need to learn new skillsto help us bridge our present with our future. When existing staff feel they are learning andgrowing personally and professionally and performing well they are more likely to staywith an organization and provide continuity by teaching and training others to becomegreat employees. DPH has identified gaps in knowledge, skills, and abilities through theassessment of both organizational and individual needs, and addresses these gaps throughtargeted training and development activities. Workforce development opportunitiesidentified in this plan align with DPH strategies in the DPH Strategic Plan.This document provides a comprehensive workforce development plan for DPH. It alsomeets the documentation requirement for Accreditation Standard 8.2.1: Maintain,implement, and assess the health department workforce development plan that addresses thetraining needs of the staff and the development of core competencies.QuestionsThe Workforce Development Plan is maintained by the Workforce DevelopmentCommittee. The Workforce Development Committee strives for representation from allDPH program areas. Members include:Art DavidsonCali ZimmermanCarol McDonaldChristie MettenbrinkElizabeth Rumbel, ChairErin BrunerKari EhmannKathy RootKristen RossLaura WeinbergMaggie McCleanNancy WittmerPeggy SarcomoFor any questions regarding the DPH Workforce Development plan, contact:Elizabeth Rumbel, Workforce Development Specialistelizabeth.rumbel@dhha.org(303) 602-35504
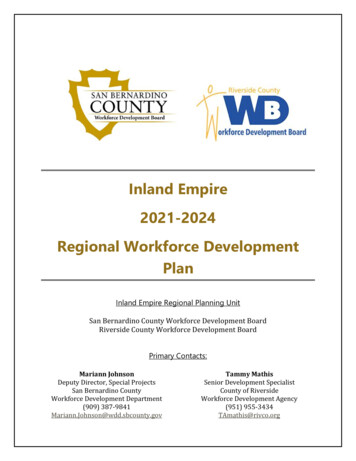
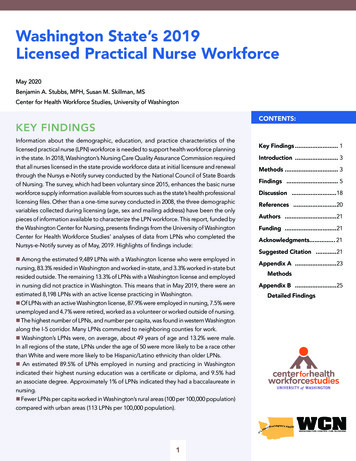
Workforce Development Plan - 2018Agency ProfileDenver Public Health Vision, Mission, and ValuesVision: Denver is a healthy community for all people.Mission: Improving health with our community.Core Values: Continuous Improvement and Innovation Excellence Collaboration EquityLocation and population servedThe City and County of Denver is the capital of Colorado with a total 2016 estimatedpopulation of 693,060. Denver ranks as the 19th most populous U.S. city. Located in theSouth Platte River Valley on the western edge of the High Plains, it lies just east of the FrontRange of the Rocky Mountains. Nicknamed the Mile-High City, its official elevation isexactly one mile or 5,280 feet above sea level. The 10-county Denver-Aurora-Lakewood, COMetropolitan Statistical Area (MSA) had an estimated 2015 population of 2,812,732 andranked as the 19th most populous U.S. MSA.The following figures describe the population served:Population by Age/Sex: Denver 201685 years and older80 to 84 years75 to 79 years70 to 74 years65 to 69 years60 to 64 years55 to 59 years50 to 54 years45-49 years40-44 years35-39 years30 to 34 years25 to 29 years20 to 24 years15 to 19 years10 to 14 years5 to 9 yearsUnder 5 yearsFemalesMales8.00% 6.00% 4.00% 2.00% 0.00% 2.00% 4.00% 6.00% 8.00%Source: 2016 US Census5
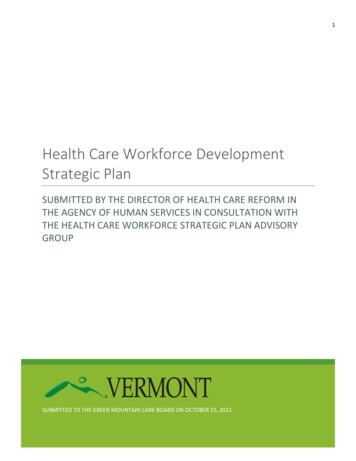
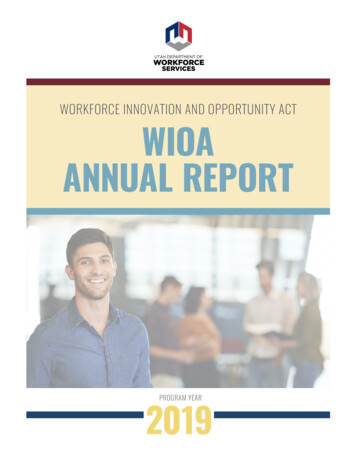
Workforce Development Plan - 2018Race/Ethnicity: Denver 2016White, not of HispanicOriginBlack, not of HispanicOrigin30.00%54.0%4.1%1.9%American Idian or AlaskanNativeAsian or Pacific Islander10.0%Hispanic or LatinoSource: 2016 US CensusGovernanceDPH provides a wide range of services that promote, improve, and protect the health andwell-being of the residents of Denver and beyond. We partner with the Denver Departmentof Public Health and Environment (formerly Denver Environmental Health), a departmentof the Denver City and County government, to provide the 10 Essential Public HealthServices. Much of the work we do is in partnership with community organizations locatedthroughout Denver’s diverse communities.Our services include the following: Birth and Death Records Clinical Care Community Health Data Educational Opportunities Community Health Promotion Activities Outbreak Detection and Investigation Services Public Health Emergency PreparednessDenver Public Health is a department of Denver Health and Hospital Authority (DenverHealth), an integrated health system whose mission is to provide care for all Denverresidents, regardless of ability to pay. Denver Health includes an acute care hospital(Denver Health Medical Center), emergency response system, community-based clinics inDenver’s low-income areas, medical and surgical specialty clinics, behavioral healthservices (including the city’s detoxification unit), school-based health centers, and theRocky Mountain Poison and Drug Center.Organizational structureAs a department of Denver Health, the Director of DPH reports to the Denver Health CEO.The DPH Director shares leadership with the Associate Director and the DPHAdministrative Director. The leadership structure of DPH includes multiple divisions6
Workforce Development Plan - 2018headed by Directors who report to the DPH Director. Program areas are managed by teamsof Program Managers/Supervisors. (See Appendix A for the DPH Organizational Chart.)FundingDPH is funded through a diverse stream of funding, which can vary across categories each year.In 2016, funding for DPH came from the following sources: 41% Federal 26% State 30% City and County 3% OtherWorkforce policiesDPH, as a department of Denver Health, is included as a part of the enterprise-wideintranet. Found in this site are Denver Health Principles and Practices (P&Ps), whichinclude P&Ps on Employee Competence. Additionally, a Public Health SharePoint sitewithin this intranet includes the DPH Workforce Development Plan. All of these internalsites are accessible to all public health employees.Communication planFeedback from DPH’s Core Leadership Team, Program Directors and Managers, and otherstaff will be sought to ensure the process of implementing the workforce goals andstrategies are done in a systematic and clear method. DPH staff will be notified via emailannually when this plan is reviewed and updated. The Workforce Development Plan will belocated, along with supporting materials, on the Workforce Development page on thePublic Health SharePoint site. Workforce development will also be the focus of adepartment town hall meeting each year to ensure all staff have the opportunity to hearabout the plan and provide feedback.7
Workforce Development Plan - 2018Workforce ProfileThis section provides a description of the current and anticipated future workforce needs.The table below summarizes the demographics of the department’s current workforce as ofJanuary 18, 2018.Current workforce demographicsCategory# or %182Total Number of icity:African American:Asian/Pacific 24% 1%3.4%3.4%29.3%62%1.7%Age:20-29:30-39:40-49:50-59: 60:14%33%27%14%12%Professional Disciplines/Credentials*:Medical nformatics:Epidemiology/Preparedness:Community Health Promotion:Trainers:DIS/Linkage to Care/Patient Navigators/Social Workers:Health Care Partners:Support Staff:Dental Clinic:Pharmacy:Employees 5 Years from Retirement:173727791361311402712%*Does not total 182 due to a number of staff being included in multiple categories.Future workforceThe changing public health landscape of the 21st century provides new opportunities andchallenges for those working in the field. Today’s public health challenges are muchbroader than in the past and require a workforce that is prepared and competent toaddress these challenges.8
Workforce Development Plan - 2018Some of the key challenges to health in the 21st century are those related to chronicdisease prevention and emergency preparedness. For over 100 years communicabledisease has been the focus of public health and continues to be a robust activity. To addressthe new challenges, we must retool our approaches and strategies. New tools for chronicdisease prevention and emergency preparedness focus on systems, policy, andenvironmental change. In chronic disease we face challenges of health inequities, socialdeterminates of health, and food deserts. In emergency preparedness we are challenged toprotect the population from biological weapons and mass casualty events. All three focicreate the opportunity to train our workforce to meet tomorrow’s challenges.In addition, we desire for every person in Denver to attain his or her full health potential,regardless of socially determined circumstances. As a result, we will strive to focus onhealth equity and broader population-based approaches and work on upstream factorssuch as the built environment, racism, poverty, educational attainment, and environmentalcauses of disease. To be effective in this work, the workforce will need support, training,and effective partnerships.Public health professionals of the future will need to understand and be able to use the newinformation systems that provide the data upon which public health research and practiceis based. They will need to be able to communicate with diverse populations, to understandthe issues, concerns, and needs of these groups in order to work collaboratively to improvepopulation health. Public health professionals must have the skills and competenciesnecessary to engage in public health practice at many levels: leadership, management, andsupervisory.Continuing education requirements by disciplineMultiple public health-related disciplines require continuing education (CE) for ongoinglicense to practice. Licensures held by staff, and their associated CE requirements, areshown in the table below. The Department encourages and supports employees pursuinglicensure and those licensed or certified as part of their assigned roles and responsibilities.ProfessionAdvanced Practice NursePhysician AssistantHealth Educator (CHES/MCHES)Nursing (RN/LPN)PharmacistPhysicianSocial Worker (LSW, LCSW, etc.)CE RequirementsVaries by specialty and certifying body*100 hours every 2 years (50 in Category 1)75 hours every 5 years10 hours annually (not required butencouraged)24 hours every 2 yearsCME based on area of discipline40 hours each renewal cycle*Advanced Practice Nursing Specialties recognized by the State Board of Nursing are nurse practitioner (NP),certified registered nurse anesthetist (CRNA), certified nurse midwife (CNM), and clinical nurse specialist(CNS), which may have a population focus (including but not limited to: Neonatal, Child, Women, Adults,Family, Mental Health). State licensure requires national certification in the individual’s specialty. As a part ofcertification, the individual commonly shows evidence of continuing education credits determined by thecertifying body for that specialty/population.9
Workforce Development Plan - 2018Core Competencies for Public Health ProfessionalsIntroductionIn 2016, DPH fully adopted the Core Competencies for Public Health Professionals (CoreCompetencies) developed by the Council on Linkages Between Academia and Public HealthPractices (Council on Linkages) by launching its first annual Core Competency Survey.The Core Competencies are a standard set of skills public health workers use to serve thecommunity in clinical and non-clinical ways. Some skills are important for all public health staffto have (such as cultural competency skills); others are specific to individuals based on their jobfunction (such financial planning and management skills).The Core Competencies are divided into the following area of public health practice: Analytical/Assessment Policy Development/Program Planning Communication Cultural Competency Community Dimensions of Practice Public Health Sciences Financial Planning and Management Leadership and Systems ThinkingDPH’s Workforce Development Committee began the process of creating an annual,department-wide Core Competency Survey in 2014. The committee decided that by conductingthe survey in a coordinated effort, the survey results could provide a framework for futuretraining and professional growth opportunities for all staff.Job classifications and competency selectionTo ensure that the survey was meaningful to all staff, the Workforce Development Committeecategorized all DPH staff into one of six job classifications: Data Drivers (Epidemiologists, Informaticians, and Researchers) Directors (Clinic Directors, Administrative Directors, and Program Directors) Healthcare Providers (Licensed RNs, NPs, PAs, and Non-Director MDs) Patient Support (Patient Clerks, Health Care Partners, Care Coordinators, ClinicAdministrators, and Social Workers) Program Support (Program Assistants, Non-Patient Clerks, Office of the Director andDPH Administrative Staff) Public Health Specialists (Program-Specific Planners, Trainers, Coordinators, Specialists,and other population-focused staff)The Workforce Development Committee worked with representatives from each of these sixjob classifications to identify between six and ten competencies that were most relevant to thatclassification’s job function. A total of 59 employees from the entire department helped in this10
Workforce Development Plan - 2018selection process, choosing competencies that best matched their role in public health ratherthan their individual job performance.In addition to these competencies specific to job classification, the Workforce DevelopmentCommittee selected 15 competencies to be surveyed of the entire department (regardless oftheir title, job classification, length of employment, or managerial status). The committee feltthat these competencies should include a focus on: evidence-based decision making, writtenand oral communication, workforce diversity, cultural influences on policies, programs, andservices, community engagement, team building, ethics, professional development, andcontinuous improvement.Competency language and tiersRather than using the Council on Linkages’ tiered language for each of the competencies (withTier 1 applying to clerks and assistants, Tier 2 applying to managers, supervisors, and thoserequiring a license or degree, and Tier 3 applying to senior management), the WorkforceDevelopment Committee met to reconcile the language from all three tiers and create newwording. The competencies were reworded, when necessary, to condense broad themes thatwould be applicable to all staff regardless of their title, job classification, length of employment,or managerial status. The new language was vetted through representatives of eachclassification to ensure that it was easy to comprehend without losing the competency’soriginal intention.Self-assessmentDPH’s Workforce Development Committee also created a self-assessment scale forindividuals to consider when taking the Core Competency Survey. All staff were asked tohonestly rate their knowledge and/or ability to apply the competency using one of fivechoices: None: I have no knowledge or don’t understand this topic Aware: I have limited knowledge of this topic Informed: I understand and can explain this topic Experienced: I can apply knowledge and skills related to this topic Expert: I am highly skilled in this topic and could teach this to othersThe Core Competency Survey was administered through a Survey Monkey link and wasopen to all staff from June 1, 2017—June 30, 2017. Staff were required to provide theirname when taking the assessment (as well as their primary area of work) so that theirresults could be shared with their managers, both in individual and aggregate form. (TheCore Competency Survey and DPH’s 2017 results can be viewed in their entirety inAppendix B.)The results of the Core Competency Survey were used in three ways:1) Every employee received personalized results that listed their highest self-assessedcompetencies to their lowest self-assessed competencies, with a reference to thecompetency’s original domain. These results were emailed to the employee and totheir manager. The intention in creating personalized results was not for11
Workforce Development Plan - 2018performance management; rather, at monthly check-in sessions with theiremployees, managers were encouraged to review the results to help employeesbrainstorm new professional development goals either based on the broad domainsof the Core Competencies or in a specific competency that they felt the employeecould improve. To help facilitate this process, managers were given a coaching guidethat included how to start the conversation and think through questions that mightarise in the one-on-one meetings. (An example of an individual’s personalizedresults, as well as the manager’s coaching guide, are available in Appendix C and D.)2) Managers received aggregate data for their program/clinic areas. This data helpedmanagers make an informed decision about program-specific trainings that theywould like to offer to increase their organizational competence. (An example of theaggregate data given to managers is available in Appendix E.)3) The Workforce Development Committee reviewed the aggregate data for the 15competencies that were surveyed of the entire department (regardless of jobclassification). From these 15 competencies, the committee selected twocompetencies to uplift at a department-level. These two competencies would be thefocus of the Workforce Development Committee’s work in 2017 and 2018, as well asa roadmap to this Workforce Development Plan. The two selected competencies are:a. Recognize the ways that diversity (e.g., food deserts, cultural views, healthequity) influences policies, programs, and services that impact the health of acommunity.b. Describe and/or provide professional development opportunities.(A graph of all of DPH’s department-level competency results is available inAppendix F.)These two competencies were selected to align to DPH’s Strategic Plan (which, in2017, adopted a focus on health equity) and to clarify information aboutprofessional development for all staff (including guidelines, funding availability, andopportunities). A full training schedule for the professional developmentcompetency is available in Appendix I; the 2017 training schedule for health equityis available in Appendix J.Creating a Learning CultureThe talents and skills of staff are a primary focus for DPH. Our patients and clients deservepublic health staff that are current, proficient, and challenged to perform at the highestlevel of their abilities. The range of activities and services that public health workersprovide requires an experienced, motivated, and well-trained workforce. Attention topublic health workforce development is essential to ensure we have a sufficient number oftrained professionals and that continuing education for these professionals is accessible,encouraged, relevant, and linked to core public health competencies.12
Workforce Development Plan - 2018The intended result is greater customer satisfaction, better public health outcomes, andmore effective use of resources. DPH invests in our employees and their continued growth.Workforce engagement is a pillar of the Denver Health Strategic Plan.Training needs assessment resultsTraining needs will be identified through various methods. Supervisors and the WorkforceDevelopment Committee will review the list of Core Competency Survey Results todetermine the training needs identified by staff and supervisors. The committee will workwith supervisors and leadership to help provide training opportunities matched to theneeds of staff. As competency checklists are developed and used within the department,additional gaps and training needs will become evident by supervisors. Additionalinformation, such as that gained from the annual Quality Improvement Assessment, will beutilized to determine training needs, if applicable.Mandatory and recommended trainingTo maintain a standard level of organizational competency, DPH ensures that all staffparticipate in mandatory training. Some training, such as Denver Health’s “Standards ofBehavior,” or eLearning Annual Curriculum are conducted on a yearly basis. Othertrainings are expected to be completed at least once, with the option to review the trainingas needed. Appendix G highlights DPH’s New Employee Orientation Checklist, whichfeatures mandatory and suggested trainings (as of January 2018).Denver Health uses the Cornerstone system to provide and track the Denver Health AnnualCurriculum for all employees. At hire and annually, each employee is required to take a setof mandatory online trainings. In addition to an annual review of the online courses, staffmust pass the associated tests with a satisfactory score to receive credit for the training. Asassigned by Human Resources, all staff are expected to log into Cornerstone to completethe training and supervisors monitor progress and completion at each annual review.Denver Health’s Annual Curriculum includes: Code of Conduct Diversity and Inclusion Drug-Free Workplace Environment of Care Infection Prevention Language Services Perfecting the Patient Experience Protected Health Information (PHI) Privacy Understanding Sexual Harassment Workplace ViolenceIn addition to mandatory all staff training, managers are required to take additional classesoffered by Denver Health’s Organizational Development Department. Appendix Gsummarizes trainings available for staff (including the annual mandatory trainings).13
Workforce Development Plan - 2018Training resourcesDPH defines Professional Development as any activities, trainings, or opportunities thatenhance and maintain skills, build competency, or prepare the staff member for theircurrent or anticipated work. Staff are encouraged to seek out meaningful professionaldevelopment experiences. For some staff, professional development might mean attendinga conference (either as a presenter or a participant); for others it could be registering foran instructor-led class or taking part in a self-guided learning activity. While someprofessional development goals are uniquely specialized to an individual’s programmaticneeds, others can be met through a variety of free training opportunities available to allDPH staff.To search for professional development and training opportunities, DPH staff areencouraged to start with three resources: Cornerstone: Cornerstone is a centralized educational system for Denver Healthand DPH employees that lets
Denver Public Health is a department of Denver Health and Hospital Authority (Denver Health), an integrated health system whose mission is to provide care for all Denver residents, regardless of ability to pay. Denver Health includes an acute care hospital (Denver Health Medical Center), emergency response system, community-based clinics in .