Transcription
ETHIOPIA HEALTH SECTORDEVELOPMENT PROGRAMMEHSDP III2005/06 – 2010/11 (GC)(1998 – 2003 EFY)Mid-Term ReviewVOLUME ICOMPONENT REPORTBy the Independent Review Team05th May – 5th June 2008Final ReportAddis Ababa, 12th July 2008
ETHIOPIA HEALTH SECTOR DEVELOPMENT PROGRAMMEMID-TERM REVIEW OF HSDP III5TH MAY TO 5TH JUNE 2008Programme:Executing Agencies:Evaluation:Period reviewed:Date submission:Ethiopian Health Sector Development Programme (HSDP III)Federal Ministry of Health and Regional Health BureausMid-Term Review (MTR) HSDP III.July 2005-December 2007 (EFY July 1998 - Dec 2000)5th June 2008Members of the Joint Core Coordinating Committee (JCCC):Dr Nejmudin Kedir (FMOH, Chairperson JCCC), Dr Teferra Wonde (WHO), Dr Viviane vanSteirteghem and Dr Alemach Teklehaimanot (UNICEF), Dr Theo Pas (Royal NetherlandsEmbassy), Ato Eshete Yilma (USAID), Ms Hiwot Tadesse (Irish Aid), Dr Pasquale Farese(Italian Cooperation), Dr Muna Abdullah (UNFPA), Ato Luelseged Ageze (ESHE/USAID),and Dr Gebresellasie Equbagzi (World Bank).The total number of consultants / experts who participated in the MTR of HSDP III was 47,(16 females and 31 males). Their contribution to the various thematic areas was as follows:Members of the Independent Review Team of the MTR 2008Dr Jarl Chabot (Technical Team Leader)1. Service Delivery (23): Dr Abdi Maalim, Dr Aboubakar Kampo, Mr Andy O’Connell, MsAnna Herforth, Dr Asnake Tesfahun, Dr Degu Jerene, Dr Endale Engida, Dr ErmiasGetahun, Mr Eshetu Lemma, Mr Fekadu Beshah, Dr Fikir Melesse, Dr Tesfaye Bulto, DrIndra Pathmanathan, Dr Joanna Nikulin, Ms Laura Ngo-Fontaine, Dr Mengistu Asnake, W/oMihret Hiluf, Dr Muna Abdullah, Ms Patricia Schwerzel, W/rt Rahel Gizaw, Dr SelamawitNegash, Dr Thierry Comolet, W/o Zewdie Abegaz.2. Support Systems (12): Mr Abel Kuiper, Dr Carlo Resti, Dr Chet Chaulagai, Ato DanielTadesse, Dr Guy Clarisse, Mr Jan Debyser, W/o Mahlet Mairegu, Dr Kwadwo Mensah, MrRob Fielding, Dr Sukanta Sarker, Ato Yetim Geta and Dr Yayehyrad Kitaw.3. Finance and Governance (12): Ato Abebe Alebachew, Dr Teniin Gakuruh, Ms GemmaWilson-Clark, Mrs Jacqueline Mogeni, Ato Mekbib Tilahun, Ato Mulu Teka, Dr Palena Neale,Dr Petros Olango, Mr Roger Pearson, Ato Wendwosen Feleke, Ato Wolderufael Tesfu andAto Yilma Abdissa.All team members were selected on the basis of their professional expertise and participatedas individuals. There were 9 international and 38 national consultants. Some members onlyparticipated part-time. The following institutions provided staff/consultant support for thisevaluation: FMOH (12), UNICEF (13), UNFPA (3), WHO (5), Italian Cooperation (2), EHNRI(1), HAPCO (1), Tulane University (2), ABT Associates (1), JSI (1), Pathfinder (1), SC-UK(1), and freelance (3). The evaluation was partly funded through the Health Pooled Funds(Technical Assistance component).As an independent review team, the opinions andsuggestions mentioned in this report are solely the responsibility of the authors and do not inany way commit or imply the agreement of the FMOH or any of the other stakeholdersoperating in the Ethiopian health sector.Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009i
Table of ContentsTABLE OF CONTENTSIILIST OF TABLES, FIGURES AND BOXESIVABBREVIATIONS AND ACRONYMSVICALENDARSXNATIONAL LEVEL INDICATORS, JUNE 2008 (2000 EC)XIADMINISTRATIVE MAP OF ETHIOPIA: REGIONS AND ZONES, 2007XIIIEXECUTIVE SUMMARYXIV1. INTRODUCTION1.1. Background to the Assignment1.2. Methodology1.3. Limitations1.4. Acknowledgements112342. SERVICE DELIVERY DURING HSDP III2.1. Health Service Delivery and Quality of Care2.1.1. Health Extension Programme (HEP)2.1.2. Family Health2.1.3. Communicable Disease Prevention and Control2.1.4. Medical Services2.1.5. Hygiene and Environmental Health2.2. Information, Education and Communication/Behavioural Change Communication2.3. Cross-Cutting Issues2.3.1. Gender2.3.2. Nutrition2.3.3. Pastoralist Health Care2.3.4. Emergency Preparedness and Response (EPR)2.3.5. Population Issues55522384754576060626568703. SUPPORT SERVICES IN HSDP III3.1. Facility Construction and Rehabilitation3.2. Human Resource Development3.3. Pharmaceutical Supplies and Logistics3.4. HMIS, M&E and Operational Research7373798691Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009ii
4. FINANCE AND GOVERNANCE IN HSDP III4.1. Financing the Sector4.2. Health Care Financing Reforms4.3. Financial Management4.4. Governance and Sector Management4.5. Alignment and Harmonization4.6. Partnership with the NGOs/FBOs/CSOs4.7. The Right to Health Care96961061131161231261275. OVERALL HSDP III PERFORMANCE5.1. Policy Changes5.2. Equity5.3. Efficiency and Effectiveness5.4. Health Status Changes and the MDGs1291291301301316. STATUS OF RECOMMENDATIONS134ANNEXESAnnex 1AOverall Performance of HSDP III 1997 – 2000 (EC)Annex 1BOverall Performance of HSDP 1989 – 2000 (EC)Annex 2Regional and National Performance Indicators 1989 – 2000 (EC)Annex 3Terms of Reference of the HSDP III MTRAnnex 4Work Programme of the MTR TeamAnnex 5Matrix of MTR Team Members and Regional VisitsAnnex 6List of Persons MetAnnex 7List of DocumentsAnnex 8Status of Previous RecommendationsVOLUME II: REGIONAL REPORTS1. Federal Ministry of Health2. Addis Ababa3. Afar4. Amhara5. Benishangul Gumuz6. Dire Dawa7. Gambella8. Harari9. Oromiya10. Southern Nations Nationalities and Peoples Region (SNNPR)11. Somali12. TigrayEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009iii
List of Tables, Figures and BoxesTablesTable 1.1Table 2.1Table 2.2Table 2.3Table 2.4Table 2.5Table 2.6Table 2.7Table 2.8Table 2.9Table 2.10Table 2.11Table 2.12Table 2.13Table 2.14Table 2.15Table 2.16Table 2.17Table 2.18Table 2.19Table 2.20Table 2.21Table 2.22Table 2.23Table 2.24Table 2.25Table 2.26Table 3.1Table 3.2Table 3.3Table 3.4Table 3.5Table 3.6Table 3.7Table 3.8Table 3.9Table 4.1Table 4.2Table 4.3Table 4.4Table 4.5Table 4.6Table 4.7Table 4.8Table 4.9Table 4.10Table 4.11Table 4.12Table 4.13Table 5.1Gregorian and Ethiopian CalendarsProvision of EHSP Services at Community LevelOverview of the HEP Training PackagesCumulative Progress in Health Post Construction since 1996/7 (EFY)Overview of Health Posts in Selected RegionsDistribution of Health Post Kits (1998-2000 EC)Cumulative Total of HEWs Trained (1996/7-1999/00 EC)Summary of HEWs Capacity NeedsRecommendations for the Health Extension ProgrammeRecommendations for Maternal and Neonatal HealthResults EPI Programme 1997–2000 (EC)Recommendations for Family HealthRecommendations for Malaria InterventionsRecommendations for Tuberculosis and Leprosy ControlHIV Outputs 2005 to December 2007 (GC)Recommendations for HIV/AIDS InterventionsRecommendations for Blindness Prevention and Control InterventionsRecommendations for Integrated Disease Surveillance and ResponseEstimated Health Service Coverage and Utilization by Region, 1996-1999 EFYRecommendations for Medical ServicesRecommendations for Hygiene and Environmental HealthRecommendations for IEC/BCCRecommendations for Gender MainstreamingRecommendations for Nutrition InterventionsRecommendations for Pastoralist CareRecommendations for Emergency Preparedness and ResponseRecommendations for Population IssuesRecommendations for Facility Construction and MaintenancePublic Sector Physicians (Including Health Officers) per 100,000 pop. by RegionAvailable Human Resources 1989-1999 (EC)Output of Graduates from Various Training InstitutionsRecommendations to Strengthen Human Resources for HealthRecommendations for Pharmaceutical Supplies and LogisticsRecommendations for HMIS ImplementationRecommendations for Monitoring and EvaluationRecommendations for Operational ResearchEstimated Cost and Financing Plan of HSDP III (in ETB million)Budget Allocation and Expenditure (ETB) by Regions, 1997-2000 (EC)Resources Available for Use and Expenditure under Channel 2Total Regional Expenditure by Sector (in million USD)Total Health Budget and Expenditure from Known SourcesPer Capita Public Health Allocation and Spending in ETBRecommendations for Financing the Sector and Health Care Financing ReformsRecommendations for Financial ManagementRecommendations for Governance and Sector ManagementDevelopment Partners Responses to Alignment and Harmonization QuestionnaireRecommendations for Alignment and HarmonizationRecommendations for Partnerships with NGOs/FBOs/CSOsRecommendations for Right to Health CareHealth Related MDGs and Progress towards PASDEP 2009/2010 TargetsEthiopia MTR HSDP III Final, Executive Summary, 23125126127132iv
FiguresFigure 2.1Figure 2.2Figure 2.3planningFigure 3.1Figure 3.2Figure 3.3Figure 4.1Figure 4.2Figure 4.3Figure 4.4Figure 4.5Funding for Family Health24Ethiopia New Sputum Smear PTB Case Detection Trend 1998-2000 (EC)40Afar: A HEW helps increase EPI coverage rates and encourages uptake in family67New Pharmacies and Drugstores75Infrastructure Management Resources75Typical Layout for Safe Delivery and CEmONC76Per Capita Allocation and Expenditure by Regions, 1998-199998Financial Contributions by Development Partners, 1997-2000 (EC)99GOE, GHI and Development Partner’s Share of Public Health Expenditure (1999 EC)101Per Capita Cost, Budget and Expenditure in ETB102Proposed Sector Coordination Structure122BoxesBox 2.1Box 2.2Box 2.3Box 2.4Box 2.5Box 2.6Box 2.7Box 2.8Box 2.9Box 3.1Box 3.2Box 4.1Box 4.2HSDPIII Targets for 2002 (EC)Visit to a Health Post AnnexImportance of UpgradingWin-Win Situations: Collaboration between HEWs and TBAsKey Questions Regarding Skilled Birth AttendantsTwinning to Improve Clinical CompetenceTwo-Pronged Approach to Improve EmONCCritical Steps to Improve Production and Quality of Skilled Birth AttendantsContraceptive ChoicesHRH Retention Strategy in OromiyaReliability of HMIS Routine DataPiloting Fee Waivers: A SC-UK Best PracticeParis Declaration IndicatorsEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009510152627282930367993108124v
Abbreviations and FBOAccess to Clinical and Community Maternal, Neonatal and Women's HealthAccelerated Expansion of Primary Health Care CoverageAcquired Immune Deficiency SyndromeAcute Watery DiarrhoeaAdolescent Youth and Reproductive HealthAdolescent Youth and Reproductive Health StrategyAnnual Review MeetingAntenatal CareAnti-Retroviral TherapyArtemisin-Based Combination TherapyBasic Emergency Obstetric and Neonatal CareBehavioural Change CommunicationBureau of Finance and Economic Development (Regions)Case Detection RateCataract Surgical RateCentral Joint Steering CommitteeCentre for Disease ControlChristian Relief and Development AssociationCivil Service Reform ProgrammeCivil Society OrganizationCommunity Health PromoterCommunity Integrated Management of Childhood IllnessesCommunity-Based Health InsuranceCommunity-Based NutritionComprehensive Emergency Obstetric and Neonatal CareContraceptives Acceptors RateContraceptives Prevalence RateCouple of Years ProtectionDemographic Health SurveyDepartment for International Development (UK)Deutsche Gesellschaft für Technische ZusammenarbeitDevelopment Assistance GroupDevelopment Cooperation IrelandDiphtheria, Pertussis and Tetanus VaccineDirectly Observed Treatment Short CourseDisaster Prevention and Preparedness AgencyDisaster Prevention and Preparedness CommissionDrug Administration and Control AuthorityDrug and Therapeutic CommitteesEarly Warning SystemEmergency Obstetrics Neonatal CareEnhanced Outreach StrategyEssential Health Service PackageEssential Nutrition ActionsEssential Services for Health in EthiopiaEthiopian BirrEthiopian CalendarEthiopian Demographic and Health SurveyEthiopian Fiscal YearEthiopian Health and Nutrition Research InstituteExpanded Programme of ImmunizationExternal Quality ControlFaith Based OrganizationEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009vi
EMTRFamily Health InternationalFederal Ministry of EducationFederal Ministry of HealthFemale Genital MutilationFinancial Management Information SystemFirst Expired-First OutGeneral PractitionerGlobal Alliance for Vaccines and ImmunizationGlobal Fund against AIDS, Tuberculosis and MalariaGlobal Health InitiativesGood Hygienic PracticesGovernment of EthiopiaGregorian CalendarHealth and Health Related IndicatorsHealth Care FinancingHealth Commodity Supply SystemHealth Education CentreHealth Emergency Preparedness and ResponseHealth Extension and Education CentreHealth Extension ProgrammeHealth Extension WorkersHealth Management Information SystemHealth Pooled FundHealth Population and NutritionHealth Sector Development ProgrammeHIV Counselling and TestingHIV/AIDS Prevention and Control OfficeHSDP Harmonization ManualHuman Immunodeficiency VirusHuman Resource Management Information SystemHuman Resources DevelopmentHuman Resources for HealthInformation Communication TechnologyInformation, Education and CommunicationInsecticide Treated NetIntegrated Disease Surveillance and ResponseIntegrated Management of Childhood IllnessesIntegrated Management of Newborn and Childhood IllnessesIntegrated Refresher TrainingInternational Development Association (World Bank)International Health PartnershipIntra-Uterine DeviceIron/Folic AcidJapan International Cooperation AgencyJohn Snow IncorporatedJoint Core Coordinating CommitteeJoint Review MissionJoint United Nations Programme on HIV/AIDSLogistics Management Information SystemMaking Pregnancy SaferManual Vacuum AspirationMaternal and Neonatal Mortality and MorbidityMaternal Mortality RatioMaternal Neonatal Child HealthMaternal Neonatal HealthMédecins Sans Frontières (Doctors without Borders)Medical Association of Physicians in Private PracticeMid-Term ReviewEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009vii
SDPRPSIDASSSCMillennium Development GoalMinistry of Capacity BuildingMinistry of EducationMinistry of Finance and Economic DevelopmentMonitoring and EvaluationMultiple Drug ResistanceNational Drug PolicyNational Health AccountsNational Health Communication StrategyNational Nutrition PolicyNational Nutrition StrategyNon Governmental OrganizationNorwegian Agency for International DevelopmentNucleus Health CentreOral Contraceptive PillOral Rehydration SaltsOut Patient DepartmentParticipatory Hygiene and Sanitation TransformationPeople Living With HIV/AIDSPerformance Package FundPharmaceutical Fund and Supply AgencyPharmaceutical Logistics Master PlanPharmaceutical Supply and Logistic DepartmentPharmaceuticals and Medical Supplies Import and DistributionPhysical Assets Management Information SystemPlan for Accelerated and Sustained Development to End PovertyPlanning and Programming DepartmentPopulation Services InternationalPostnatal CarePoverty Reduction Strategy PaperPresident's Emergency Plan for Aids ReliefPrevention of Mother to Child TransmissionPrimary Health CarePrimary Health Care UnitProcurement and Logistics Management SystemProgramme Action PlanProtection of Basic ServicesPublic Expenditure ReviewPublic Finance ManagementPublic Private PartnershipRapid Diagnostic TestRational Drug UseRegional Health BureauRegional Joint Steering CommitteeRegional Training CentreReproductive HealthRevolving Drug FundRoyal Netherlands EmbassySave the Children UKSexually Transmitted InfectionSocial Health InsuranceSouthern Nations Nationalities and Peoples RegionSpecial PharmacySupply Chain Management SystemSurgery, Antibiotic, Face washing and Environmental ImprovementSustainable Development and Poverty Reduction ProgrammeSwedish International Development AgencySupport Systems Steering CommitteeEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009viii
EDTechnical and Vocational Education Training SchoolTerms of ReferenceTetanus ToxoidTherapeutic Feeding ProgrammeTotal Fertility RateTraditional Birth AttendantTraining of TrainerTuberculosisUnder Five Mortality RateUnited NationsUnited Nations Children’s FundUnited Nations Development ProgrammeUnited Nations Fund for Population ActivitiesUnited Nations High Commission for RefugeesUnited States Agency for International DevelopmentUnited States DollarUniversal Salt IodizationVoluntary Counselling and TestingVolunteer Community Health WorkerWater Sanitation and HygieneWereda Health OfficeWereda Joint Steering CommitteeWereda Office of Finance and Economic DevelopmentWomen of Reproductive AgeWorld Food ProgrammeWorld Health OrganizationZonal Health DepartmentZonal Office of Finance and Economic DevelopmentConversion Rate:1 USD 9, 56 Birr (May/June EFY 2001, GC 2008)1 Euro 14, 96 Birr (May/June EFY 2001, GC 2008)Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009ix
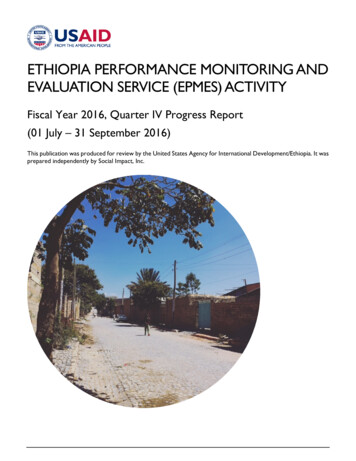
CalendarsThe Ethiopian Fiscal Year / EFY (or Ethiopian Calendar / EC) refers to the Ethiopian FiscalYear, starting on 7th July in the European calendar. Currently, June 2008 corresponds with theend of EFY 2000. The overall correspondence between Ethiopian and European fiscal years isgiven in the table below, based on the Gregorian and Ethiopian Calendars:Table 1.1Gregorian and Ethiopian 01/022002/032003/042004/052005/062006/072007/08EFY 1985EFY 1986EFY 1987EFY 1988EFY 1989EFY 1990EFY 1991EFY 1992EFY 1993EFY 1994EFY 1995EFY 1996EFY 1997EFY 1998EFY /14EFY 2000EFY 2001EFY 2002EFY 2003EFY2004EFY 2005EFY 2006EFY 2007HEALTH DEVTHSDP YEARSNAT DEVTPLANSHEALTHPOLICY1993BASELINEi-PRSPHSDP IPRSPHEALTHSDPRPPOLICY OF THEHSDP IITRANSITIONALHSDP IIIPASDEPGOVERNMENTEFY Ethiopian Fiscal Year; GC Gregorian Calendar; EC Ethiopian CalendarEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009x
National Level Indicators, June 2008 (2000 EC)SerialNo.CategoryBaselineHSDP IIIEFY 1997TargetHSDP IIIEFY 2003CurrentStatus MTREFY 1999Comments1,643 million3,250 million3,920 million(in EFY 2000)Birr 19.10(USD 2,0)Birr 91.70(USD 9,60)Birr 28.00(USD 3)Ratio of budget allocation toutilization/expenditure85%NA78%4Essential drug stock-out rateEssential Drug AvailabilityNANA0%100%Improving5HMIS completeness andtimeliness reporting rateNA80%6Level of HSDP IIIharmonization with the “oneplan, one report and onebudget” principleThis policywas not yetdefined in1997NAImplementationinitiated7Primary health servicecoverage72%100%109%8Health service utilization rateOPD / pp / yr0.300.660.32The HSDP III target is to double the share of health as a proportion of totalGovernment budget (domestic spending and direct budget support), the baseline isgiven as an absolute amount rather than a percentage.The HSDP III target is to increase total per capita health expenditure from USD 5.6 toUSD 9.6. This can only be determined through a National Health Account. Per capitapublic health expenditure is estimated at ETB 28 (USD 3)No target was set for this indicator in HSDP III but an increase in utilization isdesirable. There is a high level of utilization in the recurrent budget but less in thecapital budget, mainly due to the multi-year nature and delays in capital expenditure.HSDP III sets a target for essential drug availability to increase from 75% to 100%.During health centre and hospital visits, periodic shortages of essential drugs are stillreported, but the situation is improving due to the special pharmacies. However, thereis no routine information system to monitor this indicator.Currently it is difficult to estimate the performance of this indicator as not all healthfacilities are using a common HMIS reporting format due to implementation of thepilot HMIS.FMOH and Development Partners have signed a Code of Conduct, and are workingthrough joint steering committees. All partner plans are aligned with HSDP III andFMOH policy, however, there are still many reporting formats for the different sourcesof funding. Although figures are available for budgeting purposes, expenditure is notcaptured.Funding through channel 3 remains off-budget.There is little progress in alignment with government systems.Although it appears that the target has been reached by over 9%, this figure is likelyinflated, due likely errors in the nominators/denominators. However, as a result of theaccelerated expansion of the primary health service coverage plan in Ethiopia, manyregions will reach the 100 % target.The HSDP III target is to increase per capita health service utilization rate from 0.30to 0.66. Currently OPD utilization rate is used and is at 0.32. In most hospitals visited,1Input23ProcessIndicatorsGovernment budgetallocation to the healthsector: ETBTotal per capita healthexpenditure (GOE):Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009xi
SerialNo.CategoryIndicatorsBaselineHSDP IIIEFY 1997TargetHSDP IIIEFY 2003CurrentStatus MTREFY 1999CommentsAdmission / 100 persons / yr1.6NA0.2Contraceptive Acceptor Rate(CAR) / ContraceptivePrevalence Rate (CPR)Proportion of births attendedby skilled health personnel21%45%28%12%32%16%11Pentavalent coverage(DPT3)70%80%73%12ART coverageNA150,00073,00013NANASee comments14Performance and coverageof community conversationsat different levelPMTCT servicesNAHosp 100%HC 70%See comments15ITNs coverage rateNA20 millionSee comments1617Inpatient case fatality ratesTB: Case Detection RateTB: Treatment success RateImprovement of sanitationaccess rateInstitutions staffed as normsDr / Pop RatioNurse / Pop RatioMidwives / WRA RatioHEW / Pop RatioNA34%81%20%NA50%NA80%1: 67,8211 : 6,0821 : 13,6821 : 26,6871 : 14,000NA1 : 6,7591 : 2,500NA32%85%50%See commentsSee comments1 : 79,2671 : 5,9281 : 19,7341 : 8,608this rate has not increased in recent years. A underreporting is identified as one ofthe reasons, it seems necessary to explore further for possible reasons.The HSDPIII plans to expand family planning service coverage from 21% to 45%.There is a problem to use this coverage figure to monitor progress of CPR, the latteris only being collected through EDHS.The HSDP III target is to increase deliveries attended by skilled birth attendants from12% to 32%. Data from the regions suggest that the great majority of women do notdeliver in a health facility in the presence of skilled health personnel.The original HSPD III target was to increase DPT3 coverage from 61% to 90%.Findings from the regions show that this is on target. Various problems were reportedwith staffing, supervision and maintenance of the cold chain but if these areaddressed then coverage can be achieved.The HSDP III target was to provide ART to 150,000 people. Current estimates arethat over 73,000 are on ART and numbers are increasing.Though no target was set for this objective the review found plenty of evidence thatcommunity conversations are well established and that the health sector is increasingusing this forum to mobilize communities.The HSDP III target is to have PMTCT services available in 100% of hospitals and70% of health centres. Currently many regions have reached the target for hospitalsand through the accelerated expansion plan will soon reach health centre target also.Over 20 million ITNs have been distributed throughout malaria endemic parts. Astudy is underway to assess ITN utilization but it was unavailable at the time of theMTR.Not availableTreatment success rates are improving in most regions but low detection rates arestill a major concern and require follow-up.The HSDP III target is to increase latrine coverage from 20% to 80%. In manyregions coverage had reached over 50% and plans for expansion are in place.There is a need to revise staffing standards as per designation of health facilities.HSDP III sets some norms, such as 1 HEW to 2,500 people, increase ratio ofmidwives to WRA from 1:13,682 to 1:6,759. Results in EFY 1999 show the Dr/PopRatio and the Midwives/WRA Ratio both decreasing, while Nurse/Pop Ratio andHEW/Pop Ratio are improving.9Output101819OutputEthiopia MTR HSDP III Final, Executive Summary, 4-5-2009xii
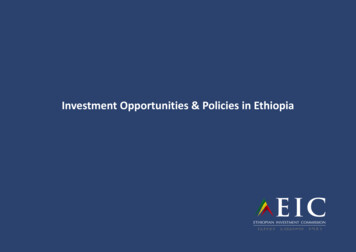
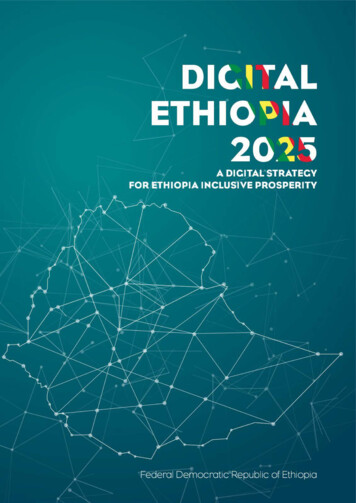
Administrative Map of Ethiopia: Regions and Zones, 2007Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009xiii
Executive Summary1. OVERALL HSDP III PERFORMANCEIntroductionBetween the 5th May and 7th June 2008 (EFY 2000), the year of the Ethiopian Millennium, amultidisciplinary team of 38 national and nine international consultants studied the mid-termperformance of the HSDP III (1998-2003). The team worked on the basis of a Terms ofReference (TOR), endorsed by the Joint Core Coordinating Committee (JCCC) and theCentral Joint Steering Committee (CJSC). In the first week, the team reviewed a multitude ofdocuments and prepared (with relevant inputs from JCCC) an exhaustive questionnaire (bylevel and by component).In the second and third week, six teams with experts in service delivery, support systems andfinance/governance visited and interviewed responsible staff in all the regions and in the twocity administrations. They also visited training institutions, regional Bureaus of Finance andEconomic Development (BOFED) and other relevant authorities. In all regions, care wastaken to visit at least two Weredas (a strong versus a weak one). Interviews were conductedwith health managers at all levels, Health Extension Workers (HEW), trainers of HEWs andmidwives. Feedback was provided on findings, challenges, conclusions andrecommendations to all Heads and their staff in the 11 regional health bureaus (RHB).During the visits, all teams drafted their regional reports, using a pre-established format. Thesame format was used during their debriefings with the RHB staff.Back in Addis Ababa (week four), the teams debriefed each other in the presence ofrepresentatives of the Federal Ministry of Health (FMOH), Development Partners and CivilSociety Organizations. The regional reports were circulated among all team members(Annex II). This formed the basis for the zero draft of the main report. The main report wasinternally discussed and validated by all team members in week five. Finally, the key findingsof the main report’s first draft were presented to the FMOH Management Team and theJCCC.Limitations of the MTRReviewing a complete sector that provides health care and support to more than 80 millionpeople in a period of five weeks is by definition limited in scope and depth. Other limitationsrelate to the lack of information on the functioning of the private and NGO sectors, the highturnover of health staff, and the inability to travel to the more remote and poorer areas of thecountry. Finally, in some instances, the reliability of national and regional data appearedquestionable. Nevertheless these are the only sources available, along with the Ethiopianand Demographic Health Survey (EDHS). For these reasons, gaps or incomplete informationmay be found in various parts of the report.AcknowledgementsThe MTR team would like to express its gratitude to the Minister of Health, His Excellency DrTedros Adhanom G/yesus for his dedicated leadership and stimulating support to the reviewprocess. Gratitude goes also to the two State Ministers, His Excellency Dr Kebede Workuand His Excellency Dr Shiferaw Teklemariam for their time and their vision on theperformance and future of HSDP. Warm thanks goes to all staff of the Ministry, the RHBs,the zonal health departments (ZHD), the Wereda health offices (WORHO) and the HEWsworking at kebele level for taking the time to respond to the multitude of questions. We havetried to bring their views and concerns as much as possible into this report.Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009xiv
Leadership and VisionIn reviewing the HSDP III performance over the last 2½ years, the MTR team found thathealth staff at all levels, demonstrated a strong commitment and vision to achieve itsobjectives. The FMOH, under the inspiring leadership of His Excellency, the Health Minister,his two State Ministers and his team of senior managers, has shown dedicated leadershipand an impressive dynamism. With its concerted energy, the FMOH has set in motion a widevariety of innovations that are now in the process of being implemented. These innovationsinclude: the Business Process Re-engineering (BPR) of some of the most importantdepartments, the Civil Service Reform Programme (CSRP), the accelerated expansion of thehealth infrastructure (health posts and health centres), the massive training and deploymentof HEWs, the start of an impressive bottom-up planning exercise by the WORHOs (the ‘CorePlan’) and the development of a community health insurance strategy for the country. Inaddition, important management initiatives have been put in place, such as the weekly,senior, management meetings, the bi-monthly meetings with all the heads of the RHBs andthe improvements in hospital management. Together, these initiatives have led to the settingof very ambitious targets, summarized by His Excellency, the Health Minister as follows: “Inthis initial phase we aim for High Speed, Big Volume and Minimal Quality”.From a bird’s eye view of the health sector, the MTR team concludes that the FMOH hasinitiated bold and courageous steps, aimed at achieving the HSDP III targets. FMOH hasshown committed leadership and impressive management practice over the last three years.Many examples of these initiatives will be discussed in the following sections of this report,but first the question, asked by His Excellency
Ethiopia MTR HSDP III Final, Executive Summary, 4-5-2009 v Figures Figure 2.1 Funding for Family Health 24 Figure 2.2 Ethiopia New Sputum Smear PTB Case Detection Trend 1998-2000 (EC) 40