Transcription
ADULT PALLIATIVE CARE SERVICESMODEL OF CARE FOR IRELANDThe National Clinical Programme for Palliative Care1
INTRODUCTIONACKNOWLEDGEMENTSEXEC. SUMMARYACKNOWLEDGEMENTSREADER INFORMATIONPatients, carers, advocacy organisations, managers, academics, health andTITLE:Adult Palliative Care Services, Model of Care for Irelandsocial care professionals have worked together to produce a documentAUTHOR:National Clinical Programme for Palliative Carethat describes best practice and communicates a compelling and inspiringVERSION:1.0vision of care. The programme is truly grateful to them all for theirAPPROVAL: CSPD005/2018tremendous contributions. We would like to also thank all members of theAPPROVED: 23.04.2018Working Group and Clinical Advisory Group who have worked so tirelesslyPUBLISHED: 25.04.2019and given so generously of their time.REVISION:Collaboration with our partners in the Department of Health, RoyalCollege of Physicians of Ireland and the HSE, the Office of the Chief Clinical25.04.2024WEB ACCESS: /CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYSGUIDELINESOfficer, Clinical Strategy and Programmes, Strategy and Planning for OlderPeople and Palliative Care and National Primary Care Operations has alsobeen hugely valued and key to the success of the programme to date.A final word of thanks goes to Kellie Myers, Programme Manager andMary Marsden, Nurse Lead and their predecessors without whom theModel of Care would not be NOTHER MOCs2IMPLEMENTATION
INTRODUCTIONTABLE OF CONTENTSEXEC. SUMMARYFOREWORD7The Eight Foundations20MEMBERS OF THE WORKING GROUP8The Overview Pathway21MEMBERS OF THE CLINICAL ADVISORY GROUP8ABBREVIATIONS9CASE FOR CHANGELIST OF FIGURES10Drivers of Change23Gaps In Palliative Care Provision25Estimation Of Need26INTRODUCTION12Current Level of Service Provision27What Is A Model Of Care?13Potential Benefits Of Palliative Care27How Was This Model Of Care Developed?13Key Points28The Let’s Talk About Survey13References29What Is The Purpose Of This Model Of Care?14Who Should Use This Model Of Care?14POLICY TO DATETerminology14Background32When Will The Model Of Care Be Reviewed?15Children’s Palliative Care33Key Points16Three Year Development Framework 2017- 201933References17National Cancer Strategy 2017 - 202633The Oireachtas Committee on the Future of Healthcare34World Health Assembly Resolution34Key Points34References35The Aim Of The Palliative Care Model3POLICY TO DATEPalliative CareEXECUTIVE SUMMARY19CASE FOR CHANGEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONTABLE OF CONTENTSEXEC. SUMMARYMODEL OF CAREPATHWAYSThe Aim Of The Palliative Care Programme Model37Overview Patient Pathway80Model Of Care Overview Pathway38Specialist Palliative Care Referral Pathway81Foundation 1: Identification And Assessment Of Need39Rapid Discharge Pathway85Foundation 2: Family and Carer Support45Loss, Grief And Bereavement Pathway87Foundation 3: Palliative Care Approach Service Provision48Night Nursing Pathways91Foundation 4: Specialist Palliative Care51Key Points95Foundation 5: Integrated Networks Of Care56References95Foundation 6: Information flow59Foundation 7: Quality Improvement61GUIDELINESFoundation 8: Research & Innovation63NCEC Pharmacological Management Of Cancer Pain, No. 997Key Points66Scope Of Guideline Number 9, Cancer Pain97References72Supporting Resources98NCEC Management Of Constipation In98Adults Receiving Palliative Care, No.10NEEDS ASSESSMENT4Scope Of Guideline Number 10, Constipation In Palliative Care99Background75Supporting Resources99Palliative Care Needs Assessment Guidance76Prevalence Studies100Additional Resources77Other NCEC Guidelines100Key Points78Care Of The Dying Adult Guideline100References78Palliative Care For People With Parkinson’s Disease100CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONTABLE OF CONTENTSEXEC. SUMMARYWORKFORCE, continuedGUIDELINES, continuedOther National Policies, Guidelines and Standards101Nursing114Key Points102Health Care Assistant115References102HSCPs, Pharmacy & Pastoral Care115Creative & Complimentary Arts118Administrative, Secretarial and General Support Staff118QUALITY IMPROVEMENTNational standards for Safer, Better Healthcare104Workforce planning – Volunteers119Specialist Palliative Care quality Assessment & Improvement105Interfacing with other specialties – Psychiatry & Psychology119Specialist Palliative Care Quality Improvement106Interfacing with other specialties – Radiology122National standards for residential care settings for olderpeople106Key Points123References128Key Points107References107WORKFORCE5Developing and supporting staff109Example of support and development in action109Palliative care Competence Framework110Education, Training & Continuing Professional Development110Workforce planning111Medicine112CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYSGUIDELINESQIINFORMATION AND COMMMUNICATION TECHNOLOGYBackground130eHealth Ireland130The electronic healthcare record and palliative care131Electronic referrals132Healthmail132Healthlink132National Medical Laboratory Information System (MedLIS)133National Integrated Medical Imaging System (NIMS)133Key THER MOCsIMPLEMENTATION
INTRODUCTIONTABLE OF CONTENTSEXEC. SUMMARYIMPLEMENTATIONMETRICSCASE FOR CHANGEHow will we know if we are improving?136NOTE ON COMPLETION OF IMPLEMENTATION SECTION149Key Points139Implementation to date - learning from lessons of pastexperience150POLICY TO DATEImplementation Logic Model – Foundation 1152MODEL OF CAREImplementation Logic Model – Foundation 2155FUNDINGPalliative care and universal healthcare141Implementation Logic Model – Foundation 3157Revenue funding for palliative care141Implementation Logic Model – Foundation 4160Current funding mechanisms for specialist palliative care142Implementation Logic Model – Foundation 5163Key Points143Implementation Logic Model – Foundation 6165Implementation Logic Model – Foundation 7167Implementation Logic Model – Foundation 8169OTHER MODELS OF CAREPalliative Care and published Models of Care144Implementation – Indicative costings171Models of Care in draft that have consulted with the NationalClinical Programme for Palliative Care146Key Points175References175Key Points147References147NEEDS UNDINGIMPLEMENTATIONOTHER MOCs6IMPLEMENTATION
INTRODUCTIONFOREWORDEXEC. SUMMARYPROF KAREN RYAN, CLINICAL LEADDR DAVID HANLON, NCAGL PRIMARY CAREThere is scarcely a conversation about healthcare in Ireland that does not reference theThe aim of the Palliative Care model of care is that:challenges of ageing demographics, constrained resources and constant change. Increasing“Every person with a life-limiting condition can easily access a level of palliative caredemands, combined with a sense of urgency, produce an environment that is oftenappropriate to their needs regardless of care setting or diagnosis in order tocomplex and pressured. With so many forces at work, it can be difficult to move from aoptimise quality of life.”focus on immediate problem-solving to a broader perspective that asks how the healthcaresystem can be redesigned without damaging its foundations. Nevertheless, National ClinicalProgrammes aim to do exactly that in its development of Models of Care that optimisehealth, care and value.Berger wrote in 1972: “We only see what we look at. To look is an act of choice.” Thisdocument is reflective of the priority placed in Ireland on palliative care provision. Ourcountry has a long and proud tradition of caring for those with life-limiting conditions, andthe publication of the Report of the National Advisory Committee on Palliative Care was aseminal moment that marked government commitment to growing and sustaining servicesbegun by communities and voluntary organisations. That commitment was echoed andexpanded in 2017 when the ‘Houses of the Oireachtas Committee on the Future ofHealthcare “Sláintecare” report’, recommended that universal palliative care should beprovided within five years of report implementation.This is an aim which has wide support not only in the Health Services but across Irishsociety. I believe that this document makes an important contribution by guidingthose who commission, plan and deliver services for people with life-limitingconditions.The National Clinical Programme for Palliative Care has been particularly successfuland productive. It has contributed hugely to broadening the scope of palliative carebeyond malignant disease alone, and highlighted the importance of a palliative careapproach in all service delivery.developed using a robust and inclusive process, and its scope extends from technicalquestions of funding and ICT to the clinical domains of needs assessment, guidelinesand patient pathways. It also takes a broad view of workforce, identifying thecompetency needs of healthcare professionals, but also recognising the contributionsof volunteers, creative arts and complementary therapies to the wellbeing of thelife-threatening condition can easily access a level of palliative care appropriate to theirpeople we all care for. This content is presented in a way which makes it easy toneeds, regardless of care setting or diagnosis, in order to optimise quality of life”.access and navigate.do. We are fortunate that Dr Brian Creedon, Consultant Physician in Palliative Medicine,has taken up the role as Clinical Lead and will guide the National Clinical Programme forPalliative Care into the next phase of action. Brian’s experience and skills ideally placePOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYSGUIDELINESI wish to thank the many people who contributed to this excellent document. It wasThe aim of the Palliative Care Model of Care is that: “Every person with a life-limiting orImplementation of the Model of Care has already started, but there remains much yet toCASE FOR CHANGEI wish to acknowledge in particular the leadership, expertise and vision of Prof KarenQIWORKFORCEICTMETRICSRyan in the development of this document. Our next step must be to make use of thisresource to guide us in delivering our common aim.FUNDINGhim to support cross-organisational and professional change, and I wish him everysuccess in this important role.7IMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONMEMBERS8EXEC. SUMMARYWORKING GROUPROLECLINICAL ADVISORY GROUPProf. Karen RyanClinical LeadDr. Aisling O’GormanProf. Karen RyanDr. Sarah McLeanMs. Mary MarsdenNurse LeadDr. Anne CleminsonDr. Kathleen CroninDr. Sarah DohertyMs. Kellie MyersProgramme ManagerDr. Brian CreedonDr. Liam O’SiorainProf. Tony O’BrienDr. Aisling O’GormanConsultant representativeDr. Camila MurtaghDr. Lucy BaldingDr. Val O'ReillyMs. Anne MolloyPublic Involvement representativeDr. Cathryn Bogan (Chair)Dr. Maeve O’ReillyDr. WilhelmMs. Deirdre RoweTherapy representativeDr. Clare McAleerDr. Marie MurphyVonHornsteinDr. Faith CranfieldConsultant representativeDr. Deirdre FinnertyDr. Marie TwomeyDr. Feargal TwomeyConsultant representativeProf. Dominic O’BrannagainDr. Mike LuceyMs. Geraldine TreacyNursing representativeDr. Dympna WaldronDr. Michael CushenMs. Gráinne TippingPharmacy representativeDr. Emmett WallsDr. Miriam ColleranDr. Lucy BaldingConsultant representativeDr. Eoin TiernanDr. Marian ConroyDr. Marie MurphyConsultant representativeDr. Eileen MannionDr. Mary DevinsMs. Marie WrightPharmacy representativeDr. Elaine WallaceDr. Mary O’LearyDr. Mary DevinsPaediatric Palliative CareDr. Faith CranfieldDr. Norma O’LearyMs. Michelle ComerfordSocial Work representativeDr. Feargal TwomeyDr. Patricia SheahanMs. Sarah McCloskeyHospice CEO group Ms.Dr. Fiona KielyDr. Paul GreganSheilagh Reaper – ReynoldsPalliative Care Lead, HSEDr. Ita HarnettDr. Pauline KaneMs. Shirley RealeTherapy representativeDr. Jane FlemingDr. Regina McQuillanDr. Stephen HigginsConsultant representativeDr. Joan CunninghamDr. Stephen HigginsCASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONABBREVIATIONSEXEC. SUMMARYABBREVIATIONSAHPsAllied Health ProfessionalsAIIHPCAll Ireland Institute for Hospice and Palliative CareCHOsCommunity Health OrganisationsNCECNational Clinical Effectiveness CommitteeCIOChief Information OfficerNCHDsNon-Consultant Hospital DoctorsCITCommunity Intervention TeamNCPPCNational Clinical Programme for Palliative CareCVADCentral Venous Access DeviceNDTPNational Doctors Training and PlanningDONDirector of NursingOOHOut of HoursECHOExtension for Community Healthcare OutcomesPAL.M.EDPalliative Medicine in the Emergency DepartmentEHRElectronic Health RecordPCNAPalliative Care Needs AssessmentEoLEnd of LifePCRNPalliative Care Research NetworkEPaCCSElectronic Palliative Care Coordination SystemsPCSBsPalliative Care Support BedsGPsGeneral PractitionersPHNPublic Health NurseHFHHospice Friendly Hospitals NetworkQA&IQuality Assurance & ImprovementHGsHospital GroupsQIQuality ImprovementHIQAHealth Information and Quality AuthoritySPCSpecialist Palliative CareHSCPHealth and Social Care ProfessionalsWHAWorld Health AssemblyHSEHealth Service Executive of IrelandWTEWhole Time EquivalentICSIrish Cancer SocietyICTInformation & Communication TechnologyIHFIrish Hospice FoundationMDTMultidisciplinary TeamNACPCReport of the National Advisory Committee onPalliative Care 2001CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCs9IMPLEMENTATION
INTRODUCTIONLIST OF FIGURESEXEC. SUMMARYLIST OF FIGURESPageFigure 1The Eight Foundations20 / 37Figure 2Overview Pathway21 / 38 / 80Figure 3Gap Analysis Palliative Care provision25Figure 4Referral to Specialist Palliative Care Pathway84Figure 5Rapid Discharge Pathway86Figure 6Loss, Grief and Bereavement Pathway90Figure 7Night Nursing, Patients with a Malignantdiagnosis Pathway92Figure 8Night Nursing, Patients with a NonMalignant diagnosis Pathway93GUIDELINESFigure 9Booking a Night Nurse during Out of Hoursperiods94QIFigure 10Proposed Model of Hospital-CommunityPsycho-oncology and Psycho-social Care121WORKFORCEFigure 11Metrics138ICTFigure 12Stages of Implementation150CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS R MOCs10IMPLEMENTATION
INTRODUCTIONINTRODUCTIONEXEC. SUMMARYCASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCs11IMPLEMENTATION
INTRODUCTIONINTRODUCTIONEXEC. SUMMARYPALLIATIVE CAREmodel of care and in the links below, describe what palliative care meansPalliative care is care that improves the quality of life of patients and theirto them and their families:families who are facing the problems associated with life-limiting or lifethreatening illness. Palliative care prevents and relieves suffering bypain and other physical, psychosocial and spiritual problems.POLICY TO DATEMODEL OF CAREmeans of early identification, impeccable assessment and treatment of1CASE FOR CHANGEPalliativeNEEDS ASSESSMENTcare is best understood as both a set of principles that underpin anapproach to care, and as a type of service that is provided. In Ireland,PATHWAYSpalliative care services are organised into specialist and non-specialistservices that operate in partnership as part of an integrated network ofGUIDELINESproviders.Many people still think of palliative care as care provided at the very lastQIstage of life, around the time of death. However, in the last twenty years,the scope of palliative care has broadened to providing palliative care atWORKFORCEan earlier stage in the disease trajectory. In this model of integratedpalliative care provision, palliative care is not dependent on prognosis andICTcan be delivered at the same time as curative treatment. While thebroader definition is far from the original idea of ‘terminal’ or ‘end of life’METRICScare, it does still include it. As Cicely Saunders stated ‘You matter becauseyou are you, and you matter to the end of your life. We will do all we canFUNDINGnot only to help you die peacefully, but also to live until you die’.2A number of patients and carers have generously lent their voices to this12These and videos of other personal experiences can be viewed atwww.adultpalliativehub.comIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONINTRODUCTIONEXEC. SUMMARYTHE LET’S TALK ABOUT SURVEYA Model of Care broadly describes a framework that brings togetherThe All Ireland Institute of Hospice and Palliative Care ‘Let’s Talk About’regulatory, organisational, financial, and clinical aspects of servicepalliative care survey had input from 528 people across the island ofprovision to outline best practice in patient care delivery. A ‘model ofIreland who were either living with a life-limiting condition or who hadcare’ is a multifaceted concept but one that is important because of theexperience of providing care to someone in this situation. Theirlink between adoption of best practices (as outlined in the Model of Care)responses provide a picture of what matters to people when they areand the delivery of improved patient outcomes.living with a progressive medical condition which is unlikely to be cured.NEEDS ASSESSMENTIn developing the Palliative Care Model of Care, the National ClinicalWhen we know what matters, services and support can be designed,PATHWAYSProgramme for Palliative Care:delivered and improved to address these issues and help people to haveHOW WAS THIS MODEL OF CARE DEVELOPED? Built on the work of the National Advisory Committee for PalliativeCare,3the HSE Three Year Development Framework (2017-2019)Future of Healthcare (Sláintecare) 6 and other relevant national policyand strategy documents, Reviewed national and international models of care, Took cognisance of other clinical programmes' Models of Care, Took cognisance of the national 'Let's Talk About' survey, 7 Involved stakeholders (patients, carers, clinical and non-clinical staff,managers and commissioners) in its co-design. Engaged in a consultation process (51 submissions received, summarydocument available from clinicalprogrammeadmin@rcpi.ie)POLICY TO DATEMODEL OF CAREas good a quality of life as possible.GUIDELINESKey messages from the survey were that:QI4Cancer Strategy (2017-2027) 5, the Oireachtas Committee on the13CASE FOR CHANGEWHAT IS A MODEL OF CARE? People need help to plan for the future, People experience too little autonomy, People value clear and sensitive communication, People value timely and appropriate information, There are emotional and psychological needs that are not met,WORKFORCEICT People would like their family and friends more involved.METRICSMore information on Let's Talk About can be found at the following links:FUNDINGvideoscribe; infographic; Executive Summary or Full ReportIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONINTRODUCTIONEXEC. SUMMARYWHAT IS THE PURPOSE OF THIS MODEL OF CARE?future. Overall, the document should be used to encourage and supportThe purpose of the palliative care model of care is to provide a frameworkdialogue between commissioners, service providers and service usersfor the organisation of care for people with life-limiting or life-threateningabout what is required to provide the best possible care to patients andconditions. Essentially, it is a tool to help commissioners and providerstheir families. It provides a platform for all to play active parts in nationalensure that people get the right care, at the right time, by the right teamand local co-design of services.CASE FOR CHANGEPOLICY TO DATEMODEL OF CAREand in the right place. A model of care defines ‘what good looks like’ andoffers actionable steps to help commissioners and services provide suchTERMINOLOGYcare. Without a model of care to guide decision-making, decisions may beA specific word on the terminology used when referring to staff providingbased on the opinions of a small number of stakeholderspalliative care services in the Model of Care. The Report of the Nationalor beconstrained by local availability of resources.WHO SHOULD USE THIS MODEL OF CARE?Commissioners, managers, clinical and non-clinical staff should all usedifferent parts of this model of care to guide their work. Commissioners and managers should use the model of care as aAdvisory Committee on Palliative Care recommended that palliative careservices should be structured in three levels of ascending specialisation.These levels refer to the expertise of the health professionals deliveringthe palliative care services: practical guide for the provision of specialist palliative care servicesbe practiced by all health care professionals. The palliative careand for the integration of the palliative care approach into hospital,approach should be a core skill of every clinician at hospital andcommunity and primary care services.community level. Many patients with progressive and advancedClinical staff should use the model of care as a reference for bestdisease will have their care needs met comprehensively andpractice.satisfactorily without referral to specialist palliative care units orPatients, carers and advocates may be interested in using the model ofcare to understand how services are being provided, what they can expectfrom service providers and how care will be further developed in the14Level one- palliative care approach: Palliative care principles shouldpersonnel. Level two – general palliative care: At an intermediate level, aproportion of patients and families will benefit from the expertise ofNEEDS UNDINGIMPLEMENTATIONOTHER MOCsIMPLEMENTATION
INTRODUCTIONINTRODUCTION EXEC. SUMMARYhealth care professionals who, although not engaged full time inwhen referring to both services providing a palliative care approach aspalliative care, have had some additional training and experience inpart of usual care provision (level 1 and 2) and specialist palliative carepalliative care, perhaps to diploma level. Such intermediate levelservices. The term ‘specialist palliative care’ is used when referring toexpertise may be available in hospital or community settings.specialist palliative care only.Level three – specialist palliative care: Specialist palliative careThe National Clinical Programme for Palliative Care has produced aservices are those services whose core activity is limited to theGlossary of Terms that provides explanations for other terms commonlyprovision of palliative care. These services are involved in the care ofused in this Model of Care.patients with more complex and demanding care needs, andWHEN WILL THE MODEL OF CARE BE REVIEWED?consequently, require a greater degree of training, staff and otherresources. Specialist palliative care services, because of the nature ofthe needs they are designed to meet, are analogous to secondary ortertiary health care services.Commonly, since the publication of the Report, the term ‘generalistpalliative care provider’ is used to refer to those health and social careprofessionals practicing at level one or two. However, we have learnedover the course of engaging with stakeholders that the term ‘generalistpalliative care provider’ is not liked or comprehended by many. Therefore,we use the term ‘professionals providing a palliative care approach as partof usual care provision’ in its place.Additionally, throughout this document the term ‘palliative care’ is usedThis document is envisaged as being a ‘living’ document that will beupdated regularly to reflect emerging practice and the developingevidence base. A full-scale review of the document will be carried out in2023.CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCs15IMPLEMENTATION
INTRODUCTIONINTRODUCTIONKEY POINTSEXEC. SUMMARYo Clinical staff should use the model of care as a reference for bestpractice. Palliative care is care that improves the quality of life of patientsand their families who are facing the problems associated with lifelimiting or life-threatening illness. Palliative care can be provided by a range of health and social carestaff and may be done alongside treatment intended to reverseparticular conditions. The purpose of the palliative care model is to provide a frameworkfor the organisation of care for people with life-limiting or lifethreatening conditions. Essentially, it is a tool to help commissionersand providers ensure that people get the right care, at the right Throughout this document the term ‘palliative care’ is used whenreferring to both services providing a palliative care approach aspart of usual care provision (level 1 and 2) and specialist palliativecare services. The term ‘specialist palliative care’ is used when referring tospecialist palliative care only. This document is envisaged as being a ‘living’ document that will beupdated regularly to reflect emerging practice and the developingCASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYSGUIDELINESevidence base. A full-scale review of the document will be carriedout in 2023.QItime, by the right team and in the right place. Commissioners, managers, clinical and non-clinical staff should alluse different parts of this model of care to guide their work.o Commissioners and managers should use the model of care as apractical guide for the provision of specialist palliative careservices and for the integration of the palliative care approachinto hospital, community and primary care THER MOCs16IMPLEMENTATION
INTRODUCTIONINTRODUCTIONREFERENCES1. World Health Organization. WHO definition of palliative care.Available from: /Accessed January 4, 20182. Saunders C. Care of the dying-1. The problem of euthanasia. NursingTimes. 1976;72(26):1003–53. Department of Health. Report of the National Advisory Committee forPalliative Care. DOH: Dublin; 2001.EXEC. SUMMARY7. All Ireland Institute of Hospice and Palliative Care. Availablefrom: final-report/Accessed January 4, 2018CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYS4. Palliative Care Services. Three Year Development Framework (20172019). velopment-framework.pdf(accessed 4 January 2018)GUIDELINES5. Department of Health. National Cancer Strategy 2017 nal-cancer-strategy-20172026/ (accessed 4 January 2018)WORKFORCE6. Houses of the Oireachtas Committee on the Future of HealthcareSlaintecare Report. Available 7.pdf Accessed January 4, 2018QIICTMETRICSFUNDINGIMPLEMENTATIONOTHER MOCs17IMPLEMENTATION
EXECUTIVE SUMMARYINTRODUCTIONEXEC. SUMMARYCASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS UNDINGIMPLEMENTATIONOTHER MOCs18IMPLEMENTATION
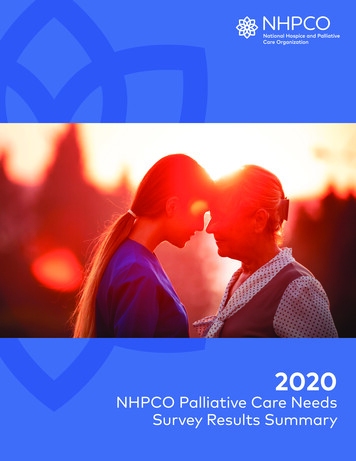
INTRODUCTIONEXECUTIVE SUMMARYThe aim of the Palliative Care Model of Care is that:EXEC. SUMMARY6. Effective and timely flow of information between hospitals,community, primary healthcare and specialist palliative care providers‘Every person with a life-limiting or life-threatening condition can easilyaccess a level of palliative care appropriate to their needs regardless ofcare setting or diagnosis in order to optimise quality of life.’To realise this aim and deliver care according to the Model of Care, thefollowing eight foundations should be in place:is in place. Communication is inclusive of patients and carers.7. A culture of quality improvement is embedded in palliative careprovision.8. A research and innovation agenda that improves the quality and valueof palliative care is supported.1. People with life-limiting or life-threatening illness receive regular,The eight foundations are illustrated in the graphic on page 20. Thestandardised assessment of palliative care need and individualisedoverview patient pathway is illustrated on page 21. Detailed explanationcare plans are co-developed to meet identified need, with the aim ofof the eight foundations and the overview patient pathway are providedoptimising quality of life.in the Model of Care section of this document. Action points for2. Carers receive practical, emotional, psychosocial and spiritual supportincluding into bereavement.3. An enabling environment is created where hospital, community andprimary healthcare providers are supported to provide a palliativecare approach as part of their normal service provision.implementation of the Model of Care are provided in the Implementationsection of the document.CASE FOR CHANGEPOLICY TO DATEMODEL OF CARENEEDS ASSESSMENTPATHWAYSGUIDELINESQIWORKFORCEICT4. Access to specialist palliative care is provided for those patients withcomplex needs and the capability of services is developed.METRICS5. Hospital, community, primary care and specialist palliative careproviders are supported to work together to provide an integratedFUNDINGmodel of care provision.IMPLEMENTATIONOTHER MOCs19IMPLEMENTATION
EXECUTIVE SUMMARY- EIGHT FOUNDATIONSPeople with life-limiting or life-threatening illness receive regular,POLICY TO DATEstandardised assessment of palliative care need and individualised careplans are co-developed to meet identified need, with the aim ofMODEL OF CAREoptimising quality of life.2.Carers receiv
48 Night Nursing Pathways 91 51 Key Points 95 56 References 95 59 61 GUIDELINES Foundation 3: Palliative Care Approach Service Provision Foundation 4: Specialist Palliative Care Foundation 5: Integrated Networks Of Care Foundation 6: Information flow Foundation 7: Quality Improvement Foundation 8: Research & Innovation