Transcription
CalAIM: Leveraging Medicaid Managed Care for Housing andHomelessness SupportsApril 15, 2022 / Allie AtkesonIntroductionDriven by challenges facing individuals withcomplex care needs, states are increasinglyworking to address the physical, behavioral, andsocial needs of their Medicaid beneficiaries. Formany with complex care needs, research showssupportive housing services are essential forexiting homelessness and staying successfullyhoused.In January 2021, the Centers for Medicare andMedicaid Services (CMS) released a roadmap forstates to address social determinants of healththat includes several options for supportivehousing services. California’s most recentMedicaid transformation initiative, CalAIM, buildsupon the state’s previous work on whole personcare to meet the care needs for complex carepopulations. This paper summarizes the differentelements of California’s initiative, which provides amodel for other states seeking to expand housingservices and whole person care through Medicaid.California Advancing and Innovating MediCalIn late December 2021, CMS approved Medicaidauthorities for the California Advancing andInnovating Medi-Cal program, or CalAIM. Theprogram was launched through a five-yearextension of the state’s 1115 demonstration waiverand Medicaid managed care section 1915(b)www.nashp.orgWashington, DC1233 20th Street NW, Suite 303Washington, DC 20036202-903-0101Whole Person Care PilotsCalifornia launched Whole PersonCare (WPC) pilots in 2016 through theMedi-Cal 2020 1115 waiver. Thepilots support local efforts to addressphysical health, behavioral health,and social needs through contractingbetween managed care and socialservice providers. The goal of theinitiative is to increase coordinationacross agencies for the mostvulnerable Medi-Cal members andreduce emergency department andinpatient health costs.Health Home ProgramThe Home Health Program (HHP) isan optional state plan benefit thatCalifornia began in 2018. Through theHHP, community-based caremanagement entities coordinate withmanaged care plans to provideadditional services to members withchronic or behavioral health needs.Services include care management,care coordination, health promotion,transitional care services, memberand family support, and referral tocommunity services.Portland, MaineTwo Monument Sq., Suite 910Portland, ME 04101207-874-6524
waiver. CalAIM builds upon California’s previous Medi-Cal initiatives, including Whole PersonCare (WPC) pilots and the Health Homes Program (HHP).The CalAIM initiative is unique in that it relies on the state’s 1115 demonstration authority,Medicaid managed care section 1915(b) waiver and managed care contracting. In CalAIM,housing supports will be delivered through managed care plans under the 1915(b) authority,creating a sustainable funding source for these services. Shifting to enhanced caremanagement (ECM) and community supports (also known as in lieu of services, or ILOS)under managed care “represents an opportunity for MCPs (managed care plans) to work withproviders, counties, and community-based organizations (CBOs) to knit together a stronger setof supports for those who need it most, supported entirely within the managed care deliverysystem.”CalAIM will provide Medi-Cal members experiencing homelessness and housing instabilityservices through the ECM and ILOS programs. California’s Department of Health CareServices (DHCS) released the document “CalAIM’s Commitment to Addressing California’sHomelessness Crisis,” which identifies the following goals: Move beyond regional pilots to statewide implementation of housing services Tailor community-based ECM services for members who are homeless Establish a long-term sustainable approach to covering housing-related services in MediCal Support a broader array of housing services through community supports and targetedECM to support access to and coordination of these services Offer major new funding and resources to support the launch of ECM and take-up ofcommunity supports throughout CaliforniaEnhanced Care ManagementECM is intensive care coordination for Medi-Cal managed care plan (MCP) members with highneeds and complex care conditions. ECM will be delivered through the managed care 1915(b)waiver and contracting with MCPs and is accounted for in capitation rates. The benefit will berolled out in phases by county and populations of focus between January 2022 and July 2023depending on where WPC and HHP programs currently exist.ServicesECM includes seven core services:1. Outreach and engagement2. Comprehensive assessment and care management plan3. Enhanced coordination of care4. Health promotion5. Comprehensive transitional care6. Member and family supportswww.nashp.org2
7. Coordination of and referral to community and social support servicesMore information on these services can be found in Appendix B of the ECM policy guide.Target PopulationThe following are the rollout phases, populations of focus and definitions:Table 1: Populations of Focus and Definitions for CalAIM’s Enhanced Care ManagementBenefitRolloutPhase1Phase 1Population of FocusDefinitionIndividuals and FamiliesExperiencing Homelessness(1) are experiencing homelessness (as defined below)and (2) have at least one complex physical, behavioral,or developmental health need with inability tosuccessfully self-manage, for whom coordination ofservices would likely result in improved health outcomesand/or decreased utilization of high-cost services.Adults with (1) five or more emergency room visits in asix-month period that could have been avoided withappropriate outpatient care or improved treatmentadherence; and/or (2) three or more unplanned hospitaland/or short-term skilled nursing facility stays in a sixmonth period that could have been avoided withappropriate outpatient care or improved treatmentadherence.Adults who (1) meet the eligibility criteria for participationin or obtaining services through: The county Specialty Mental Health (SMH) System The Drug Medi-Cal Organization Delivery System(DMC-ODS) or the Drug Medi-Cal (DMC) programHigh-Utilizer AdultsAdults with severe mentalillness or substance usedisorder (SMI/SUD)and (2) are actively experiencing at least one complexsocial factor influencing their health (e.g., lack of accessto food, lack of access to stable housing, inability to workor engage in the community, history of adversechildhood experiences (ACEs), former foster youth,history of recent contacts with law enforcement relatedto mental health and/or substance use symptoms orassociated behaviors);and (3) meet one or more of the following criteria: Are at high risk for institutionalization, overdose,and/or suicide Use crisis services, emergency rooms, urgent care,or inpatient stays as the sole source of care1ECM will be rolled out by counties and populations of focus depending on where whole person care pilots andhealth home programs currently exist.www.nashp.org3
RolloutPhase1Population of FocusDefinition Phase 2Individuals Transitioning fromIncarcerationMembers Eligible for LongTerm Care and at risk ofInstitutionalizationPhase 3Nursing Home ResidentsTransitioning to theCommunityChildren and YouthExperienced two or more emergency room visits ortwo or more hospitalizations due to SMI or SUD inthe past 12 months; or Are pregnant or postpartum women (12 months fromdelivery)Individuals who:(1) are transitioning from incarceration or transitionedfrom incarceration within the past 12 monthsand (2) have at least one of the following conditions: Chronic mental illness Substance use disorder Chronic disease (e.g., hepatitis C, diabetes) Intellectual or developmental disability Traumatic brain injury HIV PregnancyIndividuals at risk for institutionalization who are eligiblefor long-term care services who, in the absence ofservices and supports, would otherwise require care for90 consecutive days or more in an inpatient nursingfacility. Individuals must be able to live safely in thecommunity with wraparound supports.Nursing facility residents who are strong candidates forsuccessful transition back to the community and have adesire to do so.1. Children (up to age 21) experiencing homelessness2. High utilizers3. Those with serious emotional disturbance oridentified to be at clinical high risk for psychosis orexperiencing a first episode of psychosis4. Those enrolled in California Children’s Services(CCS)/CCS Whole Child Model (WCM) withadditional needs beyond the CCS qualifyingcondition5. Those involved in, or with a history of involvement in,child welfare (Including foster care up to age 26)6. Those transitioning from incarcerationProvider NetworkECM builds on the provider networks designed through the WPC and HHP models. Managedcare plans contract with WPC lead entities or HHP community-based care managemententities as ECM providers. New provider standards were developed based on WPC and HHP.Managed care plans are also expected to work and contract with county behavioral healthsystems.www.nashp.org4
Community Supports (formerly “In Lieu of Services”)California is able to provide community supports, or “in lieu of services” (ILOS), as costeffective substitutes to medical services covered under the state plan under the federalregulation 42 C.F.R . § 438.3(e), as approved by CMS. The goal of community supports is tosupport managed care plans with alternative proven options to better be able to address socialdeterminants of health concerns with their members. Managed care plans are not required toprovide community supports but are strongly encouraged to do so by DHCS. Managed careplans may add community supports every six months and remove them annually with priornotice to DHCS.ServicesCommunity supports includes 14 broad categories:1. Housing transition navigation services2. Housing deposits3. Housing tenancy and sustaining services4. Short-term post-hospitalization housing5. Recuperative care (medical respite)6. Respite services7. Day habilitation programs8. Nursing facility transition/diversion to assisted living facilities, such as residential carefacilities for the elderly and adult residential facilities9. Community transition services/nursing facility transition to a home10. Personal care and homemaker services11. Environmental accessibility adaptations (home modifications)12. Medically tailored meals/medically supportive food13. Sobering centers14. Asthma remediationThe recuperative care and short-term post-hospitalization housing services are providedthrough California’s 1115 waiver while the other 12 community supports are provided underthe state’s 1915(b) waiver and incorporated into managed care plan contracts. Managed careplans that elect to offer any of California’s preapproved community supports may choose whichcounties to offer them in and do not need to offer the services or settings statewide or in allcounties in which the Medi-Cal managed care plan operate.www.nashp.org5
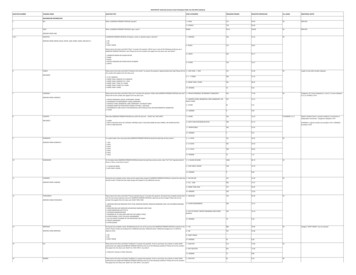
Table 2: Housing-Related Services Covered under Community SupportsServiceService DescriptionDuration gationServicesServices to assistmembers obtainhousing.Service duration isas long asnecessary in theindividual’sindividualizedhousing supportplan.Individuals prioritized forpermanent supportivehousing (PSH) throughthe homelesscoordinated entrysystem. Individuals who meet theU.S. Department ofHousing and UrbanDevelopment (HUD)definition ofhomelessness who arereceiving ECM; or have achronic condition, SMI, orSUD; or are at risk ofinstitutionalization2. HousingassessmentHousing supportplanHousing searchApplicationassistanceLandlordeducationMember advocacyCare coordinationIndividuals who meet theHUD definition of at riskof homelessness. Vocationalservices agenciesProviders ofservices forindividualsexperiencinghomelessnessLife skills trainingand educationprovidersCounty agenciesPublic hospitalsystemsMental health orSUD treatmentproviders,including countybehavioral healthagenciesService Rate(estimated, basedon non-bindingpricing guidance) 324–449 permember permonth(PMPM)32Qualifying institutions include hospitals, correctional facilities, mental health residential treatment facilities, substance use disorder residential treatment facilities,recovery residences, institution for mental disease, and state hospitals.3The pricing considers a housing care manager with a college degree providing services face-to-face in an office as well as in the community and via phone/othertechnology to a midpoint caseload of 1:35 individuals concurrently.www.nashp.orgWashington, DC1233 20th Street NW, Suite 303Washington, DC 20036202-903-0101Portland, MaineTwo Monument Sq., Suite 910Portland, ME 04101207-874-6524
ServiceService DescriptionDuration ofServiceEligibilityProvidersService Rate(estimated, basedon non-bindingpricing guidance) HousingDepositsServices to assist withidentifying,coordinating,securing, or fundingone-time services andmodifications to allowa person to establisha basic household.Does not includeroom and board. www.nashp.orgCecurity depositSet-up fees/utilitydepositsFirst monthcoverage ofutilities(telephone, gas,electricity,heating, water)First and last’smonth’s rentPest eradication,one-time cleaningAvailable once inan individual’slifetime. Servicesmust be identifiedas reasonable andnecessary in theindividual’shousing supportplan.Services can beapproved oneadditional time withdocumentation asto what conditionshave changed todemonstrate why itwould be moresuccessful on thesecond attempt.Members viduals prioritized forPSH by the coordinatedentry system.Affordablehousing providers Supportivehousing providers Federally qualifiedhealth centers andrural health clinicsCoordinating entitiesfor housing transitionnavigation services orMedi-Cal care plancase manager, carecoordinator, orhousing navigator.Plans maysubcontract services.Individuals who meet theHUD definition ofhomelessness who arereceiving ECM; or have achronic condition, SMI, orSUD; or are at risk ofinstitutionalization.7 Two times theFair MarketRent (FMR)value asestablishedunder HUD,which wouldrepresent firstand lastmonth’s rentplus 1,000 fordiscrete movingcosts/initialutilities.
ServiceService DescriptionDuration ofServiceEligibilityProvidersService Rate(estimated, basedon non-bindingpricing guidance)Available from theinitiation ofservices until theyare no longerneeded, asdetermined by theindividual’shousing supportplan.Individuals who receivedhousingtransition/navigationservices. HousingTenancy andSustainingServicesMedicallynecessaryadaptive aids andservicesService providestenancy andsustaining services. LandlordcommunityDispute resolutionEvictionpreventionAssistance withhousingrecertificationLease complianceIndependent livingand life skillsIndividuals prioritized forPSH by the coordinatedentry system.Individuals who meet theHUD definition ofhomelessness who arereceiving ECM; or have achronic condition, SMI, orSUD; or are at risk ofinstitutionalization. Individuals who meet theHUD definition of at riskof homelessness. Vocationalservices agenciesProviders ofservices forindividualsexperiencinghomelessnessLife skills trainingand educationprovidersCounty agenciesPublic hospitalsystemsMental health orsubstance usedisorder treatmentproviders,including countybehavioral healthagenciesSupportivehousing providersFederally qualifiedhealth centers andrural health clinics4 413–475(PMPM)4The pricing considers a housing care manager with a college degree providing services face-to-face in an office as well as in the community and via phone/othertechnology to a total caseload of 25 individuals concurrentlywww.nashp.org8
ServiceService DescriptionDuration lizationHousingHousing for memberswho do not have aresidence and areunable to meet suchan expense.Available once inan individual’slifetime and cannotexceed a durationof six months.Individuals exitingrecuperative care. Members must beoffered housingtransitionnavigationsupports duringthe period.Individuals exiting aninpatient hospital,residential SUDtreatment of recoveryfacility, residential mentalhealth treatment facility,correctional facility, ornursing facility who meetany of the followingcriteria:Individuals who meetHUD’s definition ofhomeless and who arereceiving ECM; or have achronic condition, SMI, orSUD; or are at risk ofinstitutionalization.Individuals who meet theHUD definition of at riskof homelessness.5 Interim housingfacilities withadditional on-sitesupportShelter beds withadditional on-sitesupportConverted homeswith additional onsite supportCounty directlyoperated orcontractedrecuperative carefacilitiesSupportivehousing providersCounty agenciesPublic hospitalsystemsSocial serviceagenciesProviders ofservices forindividualsexperiencinghomelessness5Service Rate(estimated, basedon non-bindingpricing guidance) 97–119 perdiem.6In addition to meeting one of these criteria at a minimum, individuals must have medical/behavioral health needs such that experiencing homelessness upondischarge from the hospital, substance use or mental health treatment facility, correctional facility, nursing facility, or recuperative care would likely result inhospitalization, rehospitalization, or institutional re-admission.6Pricing considers a direct care worker available 24 hours a day who provides monitoring/support to a facility of 15 to 30 beds.www.nashp.org9
ServiceService DescriptionDuration ofServiceEligibilityProvidersRecuperativeCare (MedicalRespite)7Interim housing andmeals in a recoverycare setting forindividuals who nolonger requirehospitalization.No more than 90days in continuousdurationIndividuals who are atrisk of hospitalization orare post-hospitalizationand Individuals who livealone with no formalsupports. Individuals who facehousing insecurity orhave housing that wouldjeopardize their healthand safety withoutmodification. Services may include: Assistance withinstrumentalactivities of dailyliving Transportationcoordination Connection toother ongoingservices (e.g.,mental health orSUD services) Support accessingbenefits andhousing Stability with casemanagementIndividuals who meet theHUD definition of at riskof homelessness. Interim housingfacilities withadditional on-sitesupportShelter beds withadditional on-sitesupportConverted homeswith additional onsite supportCounty directlyoperated orcontractedrecuperative carefacilities7Service Rate(estimated, basedon non-bindingpricing guidance) 181–226 perdiem.8Allowable under community supports if it is necessary to achieve or maintain medical stability and prevent hospital admission or re-admission. Cannot includefunding for building modification or rehabilitation.8The pricing considers medically trained direct care workers providing 24 hours a day of monitoring/support to a facility of 10 to 20 beds.www.nashp.org10
Providing Access and Transforming Health (PATH) Funding9As ECM and community supports build on whole person care, coordination between managedcare plans, counties, hospitals, and community-based organizations will be necessary tosupport patient-centered care coordination and evaluation. To do so, California is approved todeploy up to 1.44 billion in Providing Access and Transforming Health (PATH) fundingthrough the 1115 waiver to support local and cross-agency coordination over the five-yearrenewal period (January 2022 to December 2026). Importantly, this funding is not forreimbursable services but will be provided to qualified applicants to support capacity building,infrastructure, and systems for local networks to deliver care. This includes PATH supports tofund the following:Support for transition to managed care. WPC pilot lead entities will receive funding tocontinue services offered to members under WPC pilots until they can be transitioned tomanaged care. This includes funding to lead entities providing justice-involved services.Technical assistance marketplace.Funding for qualified applicants that workwith managed care plans to provide ECMor ILOS. Allowable expenditures include: Workforce training Assistance with data mining toidentify members eligible for ECMand/or community supports services Guidance on data-sharing practicesto connect members to housingcommunity support services Creating and implementing regionallearning collaboratives Training on connecting justiceinvolved individuals to housingservicesQualified applicants: entities approved bythe state to receive PATH payments.Criteria for qualified applicants depends onthe PATH initiative but are generally cities;counties; other government agencies;county and community-based providersincluding but not limited to public hospitals,CBOs, and Medi-Cal Tribal and theDesignees of Indian Health Programscontracted with or that intend to contractwith MCPs as ECM or community supportsproviders; and other entities as approvedby DHCS. Qualified applicants for thejustice-involved planning andimplementation program include jails,county behavioral health agencies, youthcorrectional facilities, probation offices,sheriff’s offices, state prisons, and otherentities as approved.Collaborative planning. Funding for third-party vendors to convene localities, governmentagencies, community- based providers, public hospitals, Indian Health programs, and otherstakeholders that plan to contract with managed care plans. Regular meetings over the five-9Approved 1115 waiver, STC 31, Page 32www.nashp.orgWashington, DC1233 20th Street NW, Suite 303Washington, DC 20036202-903-0101Portland, MaineTwo Monument Sq., Suite 910Portland, ME 04101207-874-6524
year period will include development of implementation plans and service gap analysis, servicedelivery challenges, and quality improvement processes.Support for expanding access to services. Funding for workforce, closed loop referralsystems, billing systems, and up-front funding to providers and community-basedorganizations to deliver ECM and ILOS. Counties, county hospitals, community-basedproviders, and Indian Health programs are eligible to receive funding.PATH justice-involved planning and implementation program. Investments to supportcollaboration and planning between DHCS, state prisons, county jails, youth correctionalfacilities, probation officers, peer support specialists, health plans, sheriff’s offices, andenrollment offices. Allowable expenditures include: Electronic health record for Medi-Cal applications pre-release and coordination of pre- andpost-release services Hiring of staff and training by qualified applicants to assist with care coordination for preand post-release services Billing systems Conferences and meetings to support collaboration Planning and process development for identification of uninsured, application assistanceand submission, and ongoing oversight and monitoringConclusionIn 2022, 95,000 Medi-Cal members will be eligible for ECM, and an estimated 40,000members will transition into community supports from existing WPC and HHP. CalAIM buildsupon California’s success in addressing the physical, behavioral, and social needs of Medi-Calmembers. Whole Person Care pilots have already shown the effectiveness of ECM andcommunity supports. For example, Los Angeles County saw a 71 percent reduction in hospitalreadmissions and 24 percent reduction in emergency department visits from the use of apsychiatric recuperative care service. Additionally, emergency department and inpatientutilization rates decreased, and positive indicators for preventive care and engagementincreased. CalAIM moves beyond the state option for innovation in 1115 demonstrationwaivers by creating sustainable funding for services through the managed care deliverysystem. As states consider how to address the health and social needs of their Medicaidmembers, CalAIM provides a model for leveraging Medicaid managed care for housingservices.Additional Resources: Contract Template Provisions for ECM and Community Supports (ILOS) ECM and Community Supports Provider Standard Terms and Conditionswww.nashp.org12
CalAIM Enhanced Care Management and Community Supports Repository of DataSharing Authorization Forms and Agreements CalAIM Data Guidance: Billing and Invoicing between ECM/Community SupportsProviders and MCPs Community Supports (In Lieu of Services) Fact SheetAcknowledgements: The National Academy for State Health Policy (NASHP) would like tothank the state officials from the California Department of Health Care Services, TylerBrennan, Bambi Cisneros, and Dana Durham, who reviewed a draft of the document. Theauthors also wish to thank Hemi Tewarson, Neva Kaye, Sandra Wilkniss, and Ella Roth ofNASHP for their contributions to the paper. This project was supported by the HealthResources and Services Administration (HRSA) of the U.S. Department of Health and HumanServices (HHS) under co-operative agreement number UD3OA22891, National Organizationsof State and Local Officials. The information, content, and conclusions are those of the authorand should not be construed as the official position or policy of, nor should any endorsementsbe inferred by HRSA, HHS, or the U.S. government.www.nashp.org13
8. Nursing facility transition/diversion to assisted living facilities, such as residential care facilities for the elderly and adult residential facilities 9. Community transition services/nursing facility transition to a home 10. Personal care and homemaker services 11. Environmental accessibility adaptations (home modifications) 12.