Transcription
Stroke & Neurovascular CenterNew JerseyJawad F. Kirmani, MDDirector Stroke & Neurovascular CenterProfessor, Seton Hall UniversitySpozhmy Panezai, MD; Mohammad Moussavi, MD; Martin Gizzi,MD, PhD; Thomas Steineke, MD; Stephen Bloomfield, MD;Gregory Przbylyski, MD; Asif Bashir, MD; Siddharat Mehta, MD;Noam Eshkar, MD; Daniel Korya, MD; Florence Chukwuneke, RN;Veronica Larson,RN NP; Charles Porbeni, MD; Nnamdi Uhegwu,MD; Madhu Gupta, MD
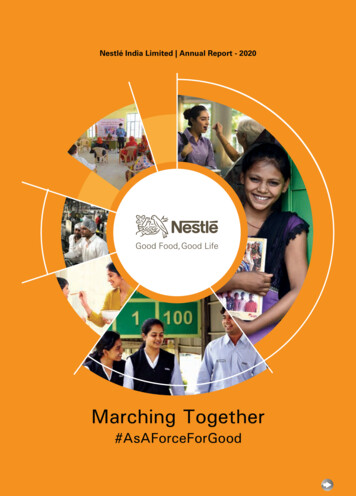
2012: 1st CSCNorthEast JC2ndStroke & Neurovascular CenterNew Jersey2003-05Architect ofNJ’s Stroke1996: NJ’s1st BiplanarDesignationLawAngiography1995: SuiteNJ ��s 1stIV tPA usein stroke2011: InitiatedNCCU2007: NJDesignatedComprehensiveStroke Center2013: StrokeDedicatedCritical CareTransport2014: StrokeBays in EDwith a built inCT1983:NJ’s 1stBrainTrauma Unit1956: 1st Case of angiographic Fibrinolytic administration in US forstroke treatment
Steps to Advanced Certification Certification Eligibility Criteria Program in US or under charter of US congress Is within the JC accredited organization Meets designated volume criteria Program Delivers Standardized clinical care – CPG’s PM and PI to improve its performance over time Application Process Meet the requirements Performance Measures
JFK Medical Center Stroke Program AHA/GWTG Gold Plus Award AHA/GWTG Stroke Target Honor RollAward Health Grades Top stroke hospital in NJ since 2003 Top 100 in US since 2011
Stroke Program GoalsRapid assessment and treatment of all patients withacute and complex stroke to ensure optimal outcomesProvision of comprehensive clinical serviceswithin a seamless continuum of careProvision of patient, family andcommunity educationRecruitment and retention ofhighly skilled medical and alliedhealth professionalsRecognition as a national center of excellence forstroke care through research and education effortsrelated to cerebrovascular disease
Board-CertifiedVascular NeurologistsNeurologyResidents andFellowsNIHSScertified;adjunct toattendingsBoard-Certified EDPhysiciansPATIENTNursing (ED orStroke Unit)8hrs ofCerebrovascularCME NIHSS8hrs ofCerebrovascularCEU NIHSS
Core Stroke arNeurosurgeonsDevelops, Reviews,& Revises ClinicalPractice Guidelines(CPGs)Oversees StrokeProgram PIActivitiesStroke onalOutreach NeedsStrokeRegistrarEDNCC Unit &Stroke UnitNurse ManagersStroke APNCoordinates carewith affiliatedPrimary StrokeCenters
Approves CPGsDesigns tools forimplementationand measurementEMSQICoordinatorEDCore ogyStaffPATIENTSocialWorkAssessescompliancewith escompliancewith StrokePerformanceMeasures
“CodeStroke!!!”Pager systemto acute stroketeam, CT,laboratory andEKGEMSinitiates prehospitalprotocol andnotifies ED ofstroke patientarrivalPATIENTwithneurologicalchange 24hrsdurationNextCalled inED or onInpatientUnits
Acute StrokeTeamrespondsimmediately& performsNIHSSPhlebotomyrespondsimmediatelyand labs aresent withstroke label asSTATPATIENTwithneurologicalchange 24hrsdurationCT Scan staffclears ascanner h study givento attendingteam member
Acute Stroke Teamdetermineseligibility for IVtPA, endovasculartreatment orclinical trialPATIENTNeurologyconsultationis calledwithneurologicalchange 24hrsdurationAcute StrokeTeam willadministeracute therapyas appropriateTreatmentdecision basedon history,NIHSS, CTresults,laboratory dataand BP
JC/NJ StateDesignatedCSCTransfer Protocol1-877-NJ-BLEEDHave transferagreements with13 PSCsAnswered by a Strokologist 24/7Non-EmergencyEmergencyCentral One call CCTinformedNCC arranges forbedResident/Fellow callsappropriate staffTransport: CCT ortransferring facility arrangesStroke Team meets patient inED and begins assessmentTeam transports patient toappropriate location andperforms handoff of careBed board will calltransferring facilitywhen bed available
Educational Outreach to PSCs Tele Stroke Tele NCCEducational Outreach to EMS
Advanced Imaging Capabilities On site 24/7 Computed Tomography (CT) CT Angiography (CTA) CT Perfusion (CTP) Magnetic Resonance Imaging (MRI) MR Angiography (MRA) Conventional Angiography Carotid Ultrasound Transcranial Doppler and Extracranial Ultrasonography Transthoracic and Transesophageal Echocardiography
Staff Availability Physicians Available 24/7 2 Endovascular Neurologists 4 Interventional Radiologists (neurointervention) 5 Neuroradiologists 2 Neuro-Intensivists & Medical Intensivists 4 Vascular Neurologists 2 Vascular Neurosurgeons 4 Surgeons with expertise in carotid endarterectomy Imaging Staff Available 24/7 Certified Radiology Technicians, MRI Technologists,Endovascular Nurses & Technicians
Staff Availability Rehabilitation Staff Director of Inpatient Rehabilitation Director of JFK Rehabilitation Consult Service BoardCertified Physiatrists Physiatry Residents PT/OT- available 6 days, on call the 7th ST- available 7 days a week
Inpatient Stroke CareNCCU 5 dedicated NCCU beds Neurointensivists and Medical Intensivists RN staff: 8 hrs stroke CEUs annually NIHSS certifiedStroke Unit 8 bed unit with telemetry monitoring RN staff – Inpatient Code Stroke responders 8 hrs of stroke education annually NIHSS certifiedAccess Center RN staff: 8 hrs stroke CEUs annually NIHSS certified
Cerebrovascular Program FellowshipsJawad F. Kirmani, MDBANEUROCRITICALCAREFELLOWSHIPYEARS 2 , 3 and ERS/TCD’S TRAININGANGIOGRAPHYVASCULARFELLOWSOngoing Clinical an Basic Science ResearchYEAR 1VASCULAR NEUROLOGY FELLOWSHIP
Care Coordination Multidisciplinary Approach: PT/OT/ST, Social Work, Case Management, Pharmacy,Rehabilitation, Nursing, Physician(s) Expertise regarding neurology & stroke careKnowledge of different levels of rehab & appropriate referralCommunity resources Multidisciplinary Rounds Stroke Education
Care Coordination Post Hospital Planning: Social Work and Case Management coordinate withother team members to prepare patient and familyfor discharge and/or next level of care Continuum of Services including Acute Rehab (onsite), Long Term Care, Outpatient Rehab, HomeCare Services, Palliative Care, and referrals toRespite Care Services and Adult Day Care
Community Education Large volume of ischemic stroke & hemorrhagic stroke Community education focus : Recognizing stroke as an emergencySymptoms recognitionActivation of EMSPrimary & Secondary Prevention
Meeting Community Needs Needs assessment 2011, increased stroke market share 7.5%in past 3 years Focus groups interviewed to assess opinion, needs, andfeelings Focused strategic planning with Medical/Dental Staff Clinical Vision Steering Committee Recommended priority tactics and actions
Needs Assessment: Focus Groups4 Focus groupsResidents ofprimaryand secondaryareasAge 45-654 Focus groupsEthnic/minorityhealthIssues: Asian,Hispanic,Asian Indian, andAfrican-American
Needs Assessment: Identified Strategies Specialized ED treatment space to accommodate strokepatients Upgrade interventional radiology suite to support servicegrowth with emphasis on neuroradiology and specialtyprocedures Enhance EMS relationships to promote program awareness Improve process to expedite transfers and admissions Broaden stroke network and enhance referrals Promote quality outcomes and performance data tocommunity
Selection and Implementation ofCPGs
Selection and Implementation of CPGsEmergency Management ofAcute Ischemic StrokeFocus on Thrombolysis andReduction ofPeristroke ComplicationsInpatient Treatment ofStrokeFocus on AntithromboticsIdentification of SourcesSecondary Stroke PreventionManagement ofHemorrhagic StrokeFocus on Management of ICHand Reduction of PeristrokeComplicationsTransient Ischemic Attackwith ObservationalServicesFocus on Monitoring, RapidWork Up, and StrokePreventionManagement ofAneurysmal SubarachnoidHemorrhageFocus on Management ofPeristroke ComplicationsEndovascular ProceduresGuidelinesFocus on Appropriate Use ofProcedures
Performance Improvement Initiatives& Peer Review
Implementation and EvaluationPerformance improvementQICoordinatorConcurrenttracking of codestroke processStroke NurseCoordinatorConcurrenttracking of strokeorder sheet useCore StrokeCommitteeConcurrent tracking ofcompliance with orders,smoking cessation, patientstroke education, strokemeasures
Stroke Measures JC 8 Core Stroke Measures Dysphagia Screening Smoking Cessation Code Stroke Response Times Code Stroke called Door to MD contact Door to CT done CT done to read Labs & EKG ordered to read Door to Drug In Hospital complications UTI, DVT, and pneumonia
Implementation and EvaluationPerformance Improvement Process Weekly clinical quality meeting reviews ED cases,admissions and discharges Monthly retrospective data analysis by theMultidisciplinary Stroke Committee Retrospective data presentation to JFKMC PI committee(Med Exec & Board)
Medical Peer Review Process:Comprehensive Stroke CareGeneric ScreensIdentified IssuesDepartment/DivisionQuality ReviewMedical Staff ComprehensiveStroke Review pective DepartmentTrendsPerformance ImprovementCommittee(Semi Annually)TrendsMedicalExecutive CommitteeTrendsBoard of Directors
RadiologyNEUROLOGYED/EMS/CCTPT/OT/ST/RehabCode StrokeAttendingAttendingVascularFellowNeurology ResidentStroke Floor/UnitAttendingVascular FellowResidentNursesNeuro CCUAttendingNCC urgeryCardiologyAnesthesiologyNeuro-Intervention Endovascular FellowVascular FellowAttendingStroke ClinicsStroke EducationOutreachEndovascular FellowVascular FellowNursesAttendingVascular FellowEndovascular FellowNurses
Recommendations for Comprehensive StrokeCenters: A Consensus Statement from the BrainAttack Coalition. Brain Attack Coalition andAmerican Stroke Association, Stroke 2005. Advanced Disease- Specific Care CertificationCore Standards: Program Management (PR) Delivering/Facilitating Clinical Care (DF) Supporting Self-Management (SE) Clinical Information Management (CT) Performance Measurement (PM)
Eligibility Volume 20 or more patients per year with a diagnosis ofaneurysmal subarachnoid hemorrhage. 15 or more endovascular coiling or surgical clippingprocedures for aneurysm are performed per year. Administration of IV tPA to 25 eligible patients per year Over 2 year average countsIVtpA given over Tele stroke at another hospital countsIVtpA given at another hospital that is then transferred counts
Eligibility Advanced Imaging Capabilities Available on-site 24 hours a day, 7 days a week Catheter angiographyCT angiographyMR angiography-MRAMRI, including diffusion weighted MRI Transcranial Doppler Carotid duplex ultrasound Extracranial ultrasonography Transesophageal Echocardiography Transthoracic Echocardiography
Eligibility Post Hospital Care Coordination for Patients Dedicated Neuro-Intensive Care Unit for ComplexStroke Patients Peer Review Process Participation in Clinical Stroke Research (IRBapproved) Performance Measures
JC Core Measure for Primary Stroke Centers DVT Prophylaxis by hospital day 2 Antithrombotics by hospital day 2 Discharged on Antithrombotics Anticoagulation for Patients with AtrialFibrillation tPA given Discharged on Statin Stroke Education Plan for Rehabilitation
CSTK Draft Measures CSTK-01 CSTK-02 CSTK-03NIHSS on ArrivalModified Rankin Score (mRS) at 90 daysSeverity Measurement on Arrival SAH/ICH CSTK-04 CSTK-04a CSTK-04bINR Reversal AchievedMedian Time to Treatment with a Procoagulant Reversal AgentMedian Time to INR Reversal CSTK-05 CSTK-05aHemorrhagic Complication (Overall)Hemorrhagic Complication for Patients treated with IV tPAwithout catheter based reperfusionHemorrhagic Complication for Patients treated with IAThrombolytic Therapy or Mechanical Endovascular Procedurewith or without IV tPA CSTK-05b CSTK-06Nimodipine Treatment Initiated CSTK-07 CSTK-7aMedian Time to Recanalization TherapyThrombolysis in Cerebral Infarction (TICI)Post Treatment Reperfusion Grade
2012: 1st CSCNorthEast JC2ndStroke & Neurovascular CenterNew Jersey2003-05Architect ofNJ’s Stroke1996: NJ’s1st BiplanarDesignationLawAngiography1995: SuiteNJ ��s 1stIV tPA usein stroke2011: InitiatedNCCU2007: NJDesignatedComprehensiveStroke Center2013: StrokeDedicatedCritical CareTransport2014: StrokeBays in EDwith a built inCT1983:NJ’s 1stBrainTrauma Unit1956: 1st Case of angiographic Fibrinolytic administration in US forstroke treatment
Thank You!
Standards
Standard PR: Program Management PR1: The program defines its leadership roles.
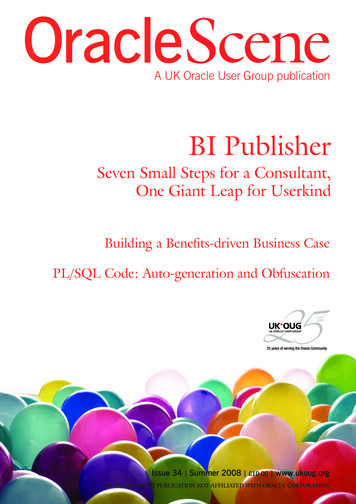
JFKMCSTROKE CENTERORGANIZATIONExecutive VP & System COOExecutive VP & COO JFKMedical ExecutiveCommitteeVascular vicesNursingChairman of NSIDirector Stroke &Neurovascular irectorOf Social Workand ke hief MedicalOfficerPrimaryMedicalDoctors &PrivateNeurologistsNeuroscienceResidents, ilitationDirectorEmergencyMedicalServicesClinical and AlliedHealth Services(PT/OT/Speech)(Dietary/Lab)
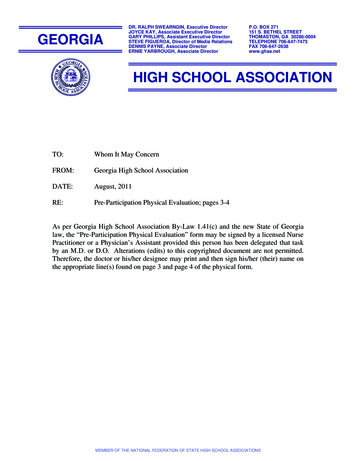
Standard PR.2: The program is designed, implemented, andevaluated collaboratively.QICoordinatorapproves CPGsEMSEDCore ogyStaffPATIENTSocialworkassesses compliancewith CPGsdesigns tools forimplementation toryassessescompliance withquality measures
Standard PR.2: The program is designed, implemented, andevaluated collaboratively.JFK MedicalCenter SquadCouncilNeuroIntervention/NCCUEMSPATIENTCore StrokeCommitteeED
Standards: The Program . PR3- meets the needs of the target population and/orhealth care service area Needs survey, program mission PR4- follows a code of ethics PR5- complies with applicable laws and regulations PR6- has current reference and resource materials readilyavailable Clinical Practice Guidelines-hospital intranet Standard written order sets- patient care areas PR7- facilities are safe and readily accessible
Clinical Practice GuidelinesEmergency Management ofAcute Ischemic StrokeInpatient Treatment ofStrokeManagement ofHemorrhagic StrokeTransient Ischemic Attackwith ObservationalServicesManagement ofAneurysmal SubarachnoidHemorrhageEndovascular ProceduresGuidelines
PR8- The Program communicates to participants the scope andlevel of care, treatment, and services it provides. Advanced Imaging CapabilitiesProcedures: Aneurysms: Microsurgical Neurovascular Clipping/ NeuroendovascularCoiling Extracranial Carotid Artery Stenting/ EndarterectomyStaff Availability (24/7)Physicians 2 Endovascular Neurologists Interventional RadiologistsNeuroradiologists Vascular NeurologistsVascular Neurosurgeons Neuro-Intensivists & Medical Intensivists Surgeons with expertise in carotid endarterectomyImaging Staff Available 24/7 Certified Radiology Technicians, MRI Technologists, Endovascular Nurses& Technicians
Staff Availability Rehabilitation Staff Director: Expertise & experience in neuro-rehabilitation Director of Inpatient Rehabilitation Director of JFK Rehabilitation Consult Service PT/OT- available 6 days, on call the 7th ST- available 7 days a week Advanced Practice Nurse Support delivery of evidence based acute stroke assessment andmanagement Expert nursing consultation and oversight Develop and deliver acute stroke continuing education programs Participate in PI processes and CSC research
PR9- The scope and level of care, treatment, andservices provided are comparable for individualswith the same acuity and type of disease beingmanaged Code Stroke Process 24/7 availability of neurological assessment for IVtPA PR10- Eligible patients have access to the program
Standard DF: Delivering/Facilitating Clinical Care DF1: Practitioners are qualified and competent DF2: The program develops a standardized processoriginating in clinical practice guidelines (CPG) orevidence-based practice to deliver or facilitate thedelivery of clinical care. Patient assessed to identify post hospital carerequirements DF3: The program is designed to meet the participant’sneeds. DF.4: The program manages co-morbidities andconcurrently occurring conditions and/orcommunicates the necessary information to managethese conditions to appropriate practitioners. Transfer Protocols
Standard SE: Supporting Self Management SE1: The program involves participants in makingdecisions about managing their disease or condition. SE2:The program addresses lifestyle changes thatsupport self-management regimens. Stroke Patient/Family Education booklet Stroke Care Discharge Instruction Sheet SE.3: The program addresses participants’ educationneeds. Post hospital care, durable medical equipment, respitecare CSC sponsors at least 2 public educational activities thatfocus on stroke prevention annually
Standard CT: Clinical Information Management CT.1: Participant information is confidential and secured. CT.2: Information management processes meet theprogram’s internal and external information needs. Stroke Team response times CT.3: Participant information is gathered from a varietyof sources. CT.4: The program shares information with any relevantpractitioner or setting about the participant’s disease orcondition across the continuum of care. CT.5: The program initiates, maintains, and makesaccessible a health or medical record for everyparticipant.
Standard PM: Performance Measurement PM1: The program has an organized, comprehensiveapproach to performance improvement. Peer Review Process Collection of data: Periprocedure complication rates for: Placement of transducer & ventriculostomy Performance of decompressive craniectomy & endovascularrecanalization Volume requirements Follow up phone calls CSC publicly reports outcomes related to interventionalprocedures
Performance improvementQICoordinatorConcurrenttracking of codestroke processStroke NurseCoordinatorConcurrenttracking of strokeorder sheet useCore StrokeCommitteeConcurrent tracking ofcompliance with orders,smoking cessation, patientstroke education, strokemeasures
JC 8 Core Stroke Measures Dysphagia Screening Smoking CessationStrokeMeasures Code Stroke Response Times Code Stroke called Door to MD contact Door to CT done CT done to read Labs & EKG ordered to read Door to Drug In Hospital complications UTI, DVT, and pneumonia
Standard PM: Performance Measurement PM2: The program uses measurement data toevaluate processes and outcomes. Stroke registry Analysis of measurement data Complication rates for CEA & CAS ( 6%)Diagnostic catheter angiography Periprocedure stroke and death rate 1% Aggregate serious complication rate 2% PM3: The program maintains data quality andintegrity.
Standard PM: Performance Measurement PM4: The process for identifying, reporting,managing, and tracking sentinel events is definedand implemented. PM5: The program collects and analyzes dataregarding variance from the clinical practiceguidelines to improve the standardized process. PM6: The program evaluates participantperception of the quality of care.
1983: NJ's 1stBrain Trauma Unit 1996: NJ's 1st IV tPA use in stroke 1996: NJ's 1st Biplanar Angiography Suite 2007: NJ-Designated Comprehensive Stroke Center 2003-05 Architect of NJ's Stroke Designation