Transcription
Multisystemic Therapy(MST) OverviewPresented byMST ServicesMultisystemic Therapy (MST)Overview1
MST Foundation for All MSTTreatment ModelsCommon elements of MST treatmentmodels include the following: Theory of change Nine guiding treatment principles Clinical decision making, problem-solvingprocess (analytic process)2
MST Foundation (continued) Use of research-based treatment techniquesStandard service delivery structureMSTI data system for decision supportStandard Quality Assurance processes andongoing training/support for providers3
What is “MST”? Community-based, family-driven treatment forantisocial/delinquent behavior in youth Focus is on “Empowering” caregivers (parents) to solvecurrent and future problems The MST “client” is the entireecology of the youth family, peers, school,and neighborhoodMultisystemic Therapy (MST)Overview4
MST Research andDisseminationThe Medical University of South Carolina,MST Services and the MST InstituteLicensed and affiliated organizations:MST Network Partner OrganizationsLocal MST Provider OrganizationsMultisystemic Therapy (MST)Overview5
MST Presence Around the WorldMultisystemic Therapy (MST)Overview6
How Does MST Work?Key Points: Theoretical and Research Underpinnings Assumptions and MST Theory of Change Core Treatment ComponentsMultisystemic Therapy (MST)Overview7
Theoretical UnderpinningsBased on social ecological theory ofUri Bronfenbrenner Children and adolescents live in a socialecology of interconnected systems that impacttheir behaviors in direct and indirect ways These influences act in both directions(they are reciprocal and bi-directional)Multisystemic Therapy (MST)Overview8
Social Ecological ModelCommunityProvider AgencySchoolNeighborhoodPeersExtended FamilyCaregiverFamilyMembersCHILDSiblings9
MST Assumptions Children’s behavior is strongly influenced by their families,friends, and communities (and vice versa) Families and communities are central and essential partners andcollaborators in MST treatment Caregivers/parents want the best for their children and wantthem to grow to become productive adults Families can live successfully without formal, mandated services Professional treatment providers should be accountable forachieving outcomes Science/research provides valuable guidanceAnd Change can occur quicklyMultisystemic Therapy (MST)Overview10
MST Theory of edAntisocialBehavior andImprovedFunctioningCommunityMultisystemic Therapy (MST)Overview11
MST Treatment Principles Nine principles of MST intervention designand implementation Treatment fidelity and adherence ismeasured with relation to these nineprinciplesMultisystemic Therapy (MST)Overview12
Principles of MST (Cont.)1. Finding the Fit:The primary purpose of assessment is tounderstand the “fit” between the identifiedproblems and their broader systemic context2. Positive & Strength FocusedTherapeutic contacts should emphasize thepositive and should use systemic strengths aslevers for change.Multisystemic Therapy (MST)Overview13
Principles of MST (Cont.)3. Increasing ResponsibilityInterventions should be designed to promoteresponsibility and decrease irresponsible behavior amongfamily members.4. Present-focused, Action-oriented & Well-definedInterventions should be present-focused and actionoriented, targeting specific and well-defined problems.Multisystemic Therapy (MST)Overview14
Principles of MST (Cont.)5. Targeting SequencesInterventions should target sequences of behaviorwithin and between multiple systems that maintainidentified problems.6. Developmentally AppropriateInterventions should be developmentally appropriateand fit the developmental needs of the youth.Multisystemic Therapy (MST)Overview15
Principles of MST (Cont.)7. Continuous EffortInterventions should be designed to require dailyor weekly effort by family members.8. Evaluation and AccountabilityIntervention efficacy is evaluated continuouslyfrom multiple perspectives, with providersassuming accountability for overcoming barriersto successful outcomes.Multisystemic Therapy (MST)Overview16
Principles of MST (Cont.)9. GeneralizationInterventions should be designed to promotetreatment generalization and long-termmaintenance of therapeutic change byempowering care givers to address familymembers’ needs across multiple systemiccontexts.Multisystemic Therapy (MST)Overview17
ReferralBehaviorMSTAnalyticalProcessDesired Outcomesof Family and OtherKey ParticipantsOverarchingGoalsEnvironment of Alignment and Engagementof Family and Key ParticipantsMST Conceptualizationof “Fit”Re-evaluatePrioritizeAssessment ofAdvances & Barriers toIntervention rmediaryGoalsDoInterventionDevelopment18
Treatment InterventionsIntervention strategies: MST draws fromresearch-based treatment techniques Behavior therapyParent management trainingCognitive behavior therapyPragmatic family therapies- Structural Family Therapy- Strategic Family Therapy Pharmacological interventions (e.g., for ADHD)Multisystemic Therapy (MST)Overview19
Service Delivery Structure The team is on call 24/7 and conducts evening andweekend visits whenever needed Services delivered in home or community Contacts occur 2-4 times per week on average butfrequency is determined by clinical need anddecreases in the final stage of treatmentMultisystemic Therapy (MST)Overview20
MST’s Research HeritageKey Points: 40 years of Science Consistent Outcomes Role of Model AdherenceMultisystemic Therapy (MST)Overview21
40 Years of Science74 Published Outcome, Benchmarking, and Implementation StudiesIncluding 26 randomized trials and 51 independent evaluations(yielding 140 peer-reviewed journal articles)with serious juvenile offendersindependent studieswith adolescents with seriousconduct problemsindependent studiesMultisystemic Therapy (MST)Overview22
Consistent OutcomesIn Comparison with Control Groups, MST: Led to higher consumer satisfaction Decreased long-term rates of re-arrest 25% to 70% 47% to 64% decreases in long-term rates of days in out-of-homeplacements Improved family relations and functioning Increased mainstream school attendance and performance Decreased adolescent psychiatric symptoms Decreased adolescent substance useBut, none of this happens without adherence to MSTMultisystemic Therapy (MST)Overview23
20 Year / Long-TermOutcomesMultisystemic Therapy (MST)Overview24
MST Fidelity Monitoring/QAActivities Required training and support activities (orientationtraining, boosters, weekly expert consultation, andweekly supervision) MST Institute hosted web-based decision supportsystem Research supported adherence measures Bi-annual review of MST implementation with programleadership using feedback from the above with goalsestablished for improvementMultisystemic Therapy (MST)Overview25
MST Fidelity MeasuresResearch-based adherence measures: TAM – youth criminal charges 36% lower for families withmaximum adherence score (1) than for families withminimum adherence score (0) SAM – youth criminal charges 53% lower for families withmaximum SAMSP score (1) than for families with minimumSAMSP score (0) CAM – consultant/MST expert adherence predicts improvedtherapist adherence and improved youth outcomesMultisystemic Therapy (MST)Overview26
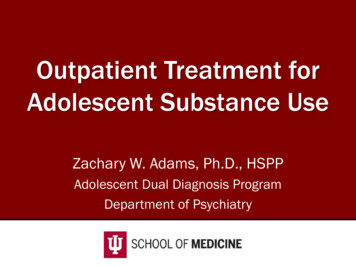
MST Transportability Study:Relationship between TAM-R and YouthCriminal Outcomes (2.3 year follow-up)TAM-R Predicting Post-Treatment Criminal ChargesNumber of Post-Treatment Charges2.50 (Min.)2.32.10.38 (-1 SD)1.90.64 (Mean)1.70.92 ( 1 SD)1 (Max.)1.5Youth criminal charges 36% lower!1.30 (Min.)0.10.20.30.40.50.60.70.80.91 (Max.)TAM-R ScoreMultisystemic Therapy (MST)Overview27
Implementation SupportGoal of MST Implementation: Obtain positive outcomes for MST youth and theirfamiliesStandard Implementation supports: Program development/start up (e.g., site visit, hiring)Organizational manual and support as neededOngoing training and support from an MST ExpertOngoing implementation monitoring (measureadherence and outcomes, and work sample reviews)Multisystemic Therapy (MST)Overview28
Implementation Support (cont.)Additional Optional Resources Yearly supervisor workshops Conferences Evaluation support from MST Institute (MSTI)Multisystemic Therapy (MST)Overview29
MST- SUBSTANCE ABUSE(MST-SA)Multisystemic Therapy (MST)Overview30
What is MST-SA? Adaptation developed to give providers expertisein contingency management (CM) interventionswhich are proven effective in the treatment ofsubstance abuse MST-SA adaptation is intended for programs thatserve a high percentage of substance-abusingyouth
Contingency ManagementIncorporated into MST Contingency Management (CM) is a substance abusetreatment approach based in behavioral and cognitivebehavioral therapy that includes– Tailored assessments of use/non-use conducted withthe youth and caregivers– Family Drug-Management Planning, including DrugRefusal Skills Training– Point and Level Reward System– Drug Testing Protocol used primarily by caregivers– Strong focus on engagement and sustainability
ACS - MST/MST-SA TargetPopulation (ages 12-18 years)Inclusionary CriteriaExclusionary Criteria Youth withdelinquent/challengingbehaviors, includingsubstance abuse Families with a high levelof conflict Youth living independently Sex offending in the absence of otheranti social behavior Youth with moderate to severe autism(difficulties with social communication, socialinteraction, and repetitive behaviors) Actively homicidal, suicidal or psychotic Youth whose psychiatric problems areprimary reason leading to referral, orhave severe and serious psychiatricproblemsMultisystemic Therapy (MST)Overview33
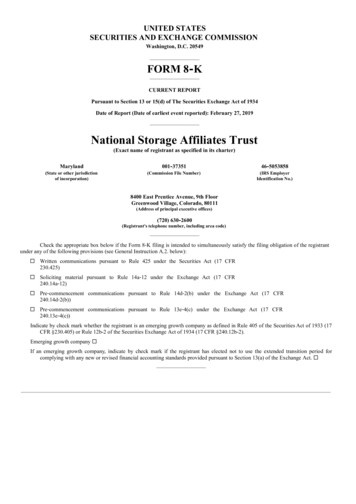
Greaterposttreatmentreductionsfor MSTSchool Attendance 98% of MSTfamiliescompletedtreatmentSubstance UseEngagement & RetentionSubstance AbuseResults in MST Significantincrease inregularschoolsettingsRandomized Trial with Substance Abusing / DependentOffenders (N 118); MST vs. Community TreatmentHenggeler, Pickrel, & Brondino, 1999
Research Conclusions Integrating CM with MST has enhanced theeffectiveness of MST in treating youthsubstance abuse. Training in contingency managementinterventions has been successfullyincorporated into all MST programs
MST-SA Staffing andStructure within ACS Supervisor full-time, masters degreeTeams of 3-4 therapists, masters degreeCaseload of 4 – 6 casesThe use of a full-time case-aide position may beapproved by MST Services on a case-by-casebasis. Treatment length 3 – 5 monthsMultisystemic Therapy (MST)Overview36
Training RequirementsSupervisors and Therapists 5-day MST orientation training Quarterly on-site booster trainingSupervisors Supervisor orientationAll of the above offered regularly in NYC
MST- PREVENTION(MST-P)Multisystemic Therapy (MST)Overview38
What is MST-Prevention? MST-SA modified to specifically meet the needs ofa child welfare preventive services system like ACS Objectives for making changes– Target the same families referred to MST-SA– Address areas of low alignment between MST-SAand the child welfare system– Implement additional practices and evaluate theimpact of the changes to further improveoutcomes within ACS Preventive Services
Implementation ChallengesThe following issues were identified as differences in contextbetween implementing standard MST in child welfare vsjuvenile justice Requirements related to all youth in the home vs just thetarget youth Focus on child safety and well-being as opposed to priorityon community safety for juvenile justice High level of monitoring against ACS standards to ensure allsafety issues are met which results in longer length oftreatment
MST-PreventionTarget Population for ACS Target child 10 – 18 years old Young people involved with child welfare that are atrisk of child abuse or neglect due to delinquent/incorrigible behaviors or challenges parenting anadolescent Young people with substance use problems Families with high family conflict41
Toward A More Specific Treatmentfor CW Prevention ServicesBuilding on all treatment components of MST/MST-SA,MST-P added the following: Increased focus on use of motivation enhancementtechniques and skill building with caregivers to: Increase interpersonal effectiveness and impulse control Decrease emotional dysregulation Increase positive affect in the family Higher sense of urgency regarding child safetyconcerns driven by weekly and long-term goals Standardized assessment of child well-being42
MST-Prevention Outcomes Pilot project conducted with MST-SA ACS TeenPrevention Project teams using data collectedat the MST Institute between 11/1/2013 and1/31/16. Single team implementing adaptationcompared to other teams on the MST keyoutcomesMultisystemic Therapy (MST)Overview43
Key MST OutcomesNo families were closed due to lack of engagement in MST-PreventionMultisystemic Therapy (MST)Overview44
Measure of Child Well-BeingMultisystemic Therapy (MST)Overview45
Family Support CaseworkerOutcomesInstrumental Outcomes:For Families with Identified Need, the Percent of FamiliesDemonstrating Improvement at Discharge:1. Access to resources for basic needs (including food, clothing,furniture)2. Skills to pursue employment opportunities3. Skills or resources to maintain benefits through public assistance asneeded4. Resources for adult education, ESL, or vocational programs5. Access to referrals, programs, or resource for pro-social activities forall minor children6. Support to ensure supervision to all minor children7. Skills and resources to ensure appropriate educational programs forall minor childrenUltimate Case Work Outcomes1.Family is financially stable meeting all basic needs for children2.Family’s health and mental health needs are met3. Family housing is stabilized without risk of homelessness4. No safety factor presentNumber ofCases withNeeds Identified% Yes23100%42375%100%34667%87%302970%93%Number ofCases 5298%90%98%90%46
Summary of Findings fromInitial Research Outcomes for MST-Prevention were comparable toMST-SA and included additional outcomes related tochild welfare, e.g., child well-being and caseworkoutcomes Casework outcomes improved during treatment formost families– Instrumental (e.g., increase family access to resourcesfor basic needs, public assistance, and educationalprograms) and– Ultimate (e.g., family financial stability, health, housing,and safety)47
MST-PreventionStaffing and Structure for ACS Supervisor full-time, masters degreeTeams of 3-4 therapists, masters degreeFamily support caseworker, bachelor degreeCaseload of 4 – 6 casesTreatment length 4 – 9 monthsMultisystemic Therapy (MST)Overview48
Casework ActivityDifferencesMST/MST-SA Per model standards, thereis no one on the team toassist families with theircasework needs In NYC, some providers havestaff at the agency to assistwith casework, notstandardizedMST-PREV Family Support Caseworkerposition is fully integratedon team and accountable toMST-PREV supervisor Standard assessmentprotocol including SDQ,safety, and psychosocialneeds and outcomes49
Training RequirementsTraining requirements are the same as MST-SAwith the following additions: 2 day MST-Prevention Orientation for alltreatment staff MST-Prevention Supervisor Orientation
Thank you for your time and uestions?Contact Melanie.Duncan@mstservices.comMultisystemic Therapy (MST)Overview51
Contingency Management (CM) is a substance abuse treatment approach based in behavioral and cognitive-behavioral therapy that includes - Tailored assessments of use/non-use conducted with the youth and caregivers - Family Drug-Management Planning, including Drug-Refusal Skills Training - Point and Level Reward System