Transcription
[2015]ALC 2: Psychosocial interventions for the management of alcohol dependence. [2015]SCOPING QUESTION: In people with alcohol dependence, are psychosocial interventions (including twelve step facilitationtherapy, cognitive behavioural therapy, motivational enhancement therapy, and screening and brief intervention) effective inthe management of alcohol dependence?BACKGROUNDAlcohol use disorders are common and are associated with a range of adverse health outcomes with physical, psychological and social implications(Srivastava et al., 2008). There exists a link between alcohol use disorders and non-communicable diseases, which necessitates a public healthresponse to this issue.Psychosocial interventions are best described as “psychologically-based interventions aimed at reducing consumption behaviour or alcohol-relatedproblems” (Kaner et al., 2007), which exclude any pharmacological treatments. This term refers to a heterogeneous collection of interventions,which vary depending on (a) theoretical underpinnings (e.g., psychodynamic, behavioural, motivational); (b) duration or intensity (e.g., brief,extended); (c) setting (e.g., primary care based, inpatient); (d) mode of delivery (e.g., group, individual, web based); or (e) treatment goals (e.g.,abstinence oriented, harm reduction). To date, many psychosocial interventions specifically designed to address problem alcohol use have beendescribed. The most frequently used interventions include motivational interviewing (MI), cognitive-behavioural therapy (CBT), brief interventions(SBI) and Twelve Step facilitation programmes.Primary care practitioners may not be trained in specific mutualized or psychoanalytical therapeutic techniques, but they are nonetheless likely tobe able to offer a degree of psychosocial assistance to people with alcohol dependence and their families. This question examines the effectiveness ofpsychosocial support interventions.
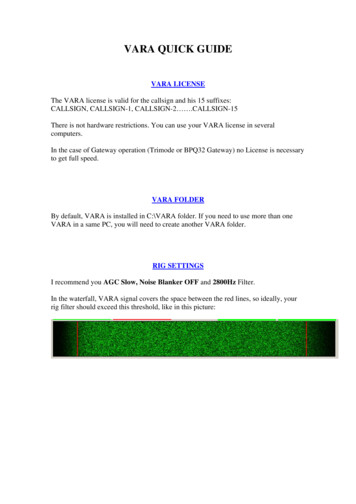
[2015]PART 1: EVIDENCE REVIEWPopulation/ Intervention / Comparison / Outcome (PICO) Population: People with alcohol dependenceInterventions:Psychosocial interventions (including Twelve Step Facilitation, Cognitive Behavioural Therapy, MotivationalEnhancement andScreening and Brief Intervention)Comparisons: Treatment as usual, wait list, no treatment, head to head comparisonOutcomes:o CRITICAL - Alcohol consumption risk patterns, alcohol consumptiono IMPORTANT - Alcohol-related harm, psychosocial functioning, deathSearch strategyA systematic literature search was conducted for systematic reviews from 2004 to 2014 including cannabis, alcohol and psychostimulants, resultingin 2550 references. Of these, 220 papers were selected for full text screening, with 58 related to alcohol, two to the combination of alcohol andcocaine dependence and 130 did not specify a primary substance. After the full text screening, 35 systematic reviews met the eligibility. SeeAppendix 1 for a detailed description of search strategies. The search and inclusion assessment process is outlined in Figure 1.The NICE guideline was selected as the systematic review because it was the most recent systematic review on this topic identified that used similarstandards and processes to WHO guidelines. The NICE guidelines lumped together different active interventions as control interventions (e.g., CBTvs. other active interventions). To enable a more precise analysis of the benefit of specific interventions, pairwise comparisons were made of eachcombination of active intervention vs. other active interventions or control. This resulted in 25 pairwise comparisons, most of which contained onlyone study. New meta-analyses were performed using the data from the NICE guidelines when comparisons of active interventions vs. activeintervention contained more than one study.
[2015]Figure 1. Selection process of systematic reviews and relevant studies
[2015]Included in GRADE tables or footnotes National Collaborating Centre for Mental Health. 2011. Diagnosis, assessment and management of harmful drinking and alcohol dependence National Clinical Practice Guideline [CG115]. London: The British Psychological Society and The Royal College of Psychiatrists. In this review synthesis the components of the NICE guidelines accepted include the systematic literature search, categorization ofpsychosocial interventions and the outcome data extraction. The researchers made new head-to-head comparisons between interventions,including meta-analysis where appropriate, which were not made in the NICE guidelines. Alden LE (1988). Behavioural self-management controlled-drinking strategies in a context of secondary prevention. Journal of Consultingand Clinical Psychology.56(2):280-286. Alessi SM, Hanson T, Wieners M, Petry NM (2007). Low-cost contingency management in community clinics: delivering incentives partially ingroup therapy. Experimental and Clinical Psychopharmacology.15(3):293–300. Burtscheidt W, Wolwer W, Schwarz R, Strauss W, Gaebel W (2001). Out-patient behaviour therapy in alcoholism: treatment outcome after 2years. Acta Psychiatrica Scandinavica.106(3):227–232. Connors GJ and Walitzer KS. Reducing alcohol consumption among heavily drinking women: evaluating the contributions of life-skillstraining and booster sessions (2001). Journal of Consulting and Clinical Psychology.69(3):447–456. Davidson D, Gulliver SB, Longabaugh R, Wirtz PR, Swift R (2007). Building better cognitive behavioral therapy: is broad-spectrum treatmentmore effective than motivational enhancement therapy for alcohol-dependent patients treated with naltrexones? Journal of Studies onAlcohol and Drugs.68(2):238–247. Davis WT, Campbell L, Tax J, Lieber CS (2002). A trial of “standard” outpatient alcoholism treatment vs. a minimal treatment control. Journalof Substance Abuse Treatment.23(1):9-19. Easton CJ, Mandel DL, Hunkele KA, Nich C, Rounsaville BJ, Carroll KM (2007). A cognitive behavioural therapy for alcohol-dependentdomestic violence offenders: an integrated substance abuse-domestic violence treatment approach (SADV). The American Journal onAddictions.16(1):24–31. Eriksen L, Björnstad S, Götestam G (1986). Social skills training in groups for alcoholics: One-year treatment outcome for groups andindividuals. Addictive Behaviors.11(3):309–329.
[2015] Fals-Stewart W, Birchler GR, Kelley ML (2006). Learning sobriety together:a randomized clinical trial examining behavioral couple’s therapywith alcoholic female patients. Journal of Consulting and Clinical Psychology.74(3):579–591. Fals-Stewart W, Klosterman K, Yates BT, O’Farrell TJ, Birchler GR (2005). Brief relationship therapy for alcoholism: A randomized clinicaltrial examining clinical efficacy and costeffectiveness. Psychology of Addictive Behaviors.19(4):363–371. Hester RK, Squires DD, Delaney HD (2005). The Drinker’s Check-up: 12-month outcomes of a controlled clinical trial of a stand-alonesoftware program for problem drinkers. Journal of Substance Abuse Treatment.28(2):159-169. John U, Veltrup C, Driessen M, Wtterling T, Dilling H (2003). Motivational intervention: an individual counselling vs a group treatmentapproach for alcohol-dependent in-patients. Alcohol and Alcoholism.38(3):263-269. Lam WKK, Fals-Stewart W, Kelley ML (2009). Parent training with behavioral couples therapy for fathers’ alcohol abuse: Effects on substanceuse, parental relationship, parenting and CPS involvement. Child Maltreatment.14(3):243–254. Litt MD, Kadden RM, Cooney NL, Kabela E (2003). Coping skills and treatment outcomes in cognitive-behavioural and interactional grouptherapy for alcoholism. Journal of Consulting and Clinical Psychology.71(1):118–128. Litt MD, Kadden RM, Kabela-Cormier E, Petry N (2007). Changing network support drinking: initial findings from the network supportprojects. Journal of Consulting and Clinical Psychology.75(4): 542-555. Marques ACPR and Formigoni MLOS (2001). Comparison of individual and group cognitive-behavioral therapy for alcohol and/or drugdependent patients. Addiction.96(6):835-846. Monti PM, Abrams DB, Binkoff JA, Zwick WR, Lipeman MR, Nirenberg TD, Rohsenow DJ (1990). Communication skills training,communication skills training with family and cognitive behavioral mood management training for alcoholics. Journal of Studies onAlcohol.51(3):263–270. Monti PM, Rohsenow DJ, Rubonis AV, Niaura RS, Sirota AD, Colby SM, Goddard P, Abrams DB (1993). Cue exposure with coping skillstreatment for alcoholics: a preliminary investigation. Journal of Consulting and Clinical Psychology.61(6):1011–1019.
[2015] Morgenstern J, Irwin TW, Wainberg ML, Parsons JT, Muench F, Bux DA Jr, Kahler CW, Marcus S, Schulz-Heik J (2007). A randomizedcontrolled trial of goal choice interventions for alcohol use disorders among men who have sex with men. Journal of Consulting and ClinicalPsychology.75(1):72–84. O’Farrell TJ, Cutter HSG, Choquette KA, Floyd FJ, Bayog RD (1992). Behavioral marital therapy for male alcoholics: Marital and drinkingadjustment during the two years after treatment. Behavior Therapy.23(4):529-549. Petry NM, Martin B, Cooney, JL, Kranzler HR (2000). Give them prizes, and they will come: Contingency management for treatment of alcoholdependence. Journal of Consulting and Clinical Psychology.68(2):250–257. Project MATCH Research Group [no authors listed] (1997). Matching alcoholism treatments to client heterogeneity: Project MATCHposttreatment drinking outcomes. Journal of Studies on Alcohol.58(1):7–29. Project UKATT Research Group (2005). Effectiveness of treatment for alcohol problems: findings of the randomised UK alcohol treatmenttrial (UKATT). BMJ: British Medical Journal.331(7516):541-544. Rosenblum A, Cleland C, Magura S, Mahmood D, Kosanke N (2005). Moderators of effects of motivational enhancements to cognitivebehavioural therapy. The American Journal of Drug and Alcohol Abuse.31(1):35–58. Rosenblum A, Magura S, Kayman DJ, Fong C (2005). Motivationally enhanced group counselling for substance users in a soup kitchen: arandomized clinical trial. Drug and Alcohol Dependence.80(1):91–103. Sandahl C, Herlitz K, Ahlin G, Ronnenberg S (1998). Time-limited group psychotherapy for moderately alcohol dependent patients: arandomized controlled clinical trial. Psychotherapy Research.8(4):361–378. Sellman JD, Sullivan PF, Dore GM, Adamson SJ, MacEwan I (2001). A randomized controlled trial of motivational enhancement therapy (MET)for mild to moderate alcohol dependence. Journal of Studies on Alcohol.62(3):389-396. Shakeshaft AP, Bowman JA, Burrows S, Doran CM, Sanson-Fisher RW (2002). Community-based alcohol counselling: a randomized clinicaltrial. Addiction.97(11):1449–1463. Sitharthan T, Sitharthan G, Hough MJ, Kavanagh DJ (1997). Cue exposure in moderation drinking: a comparison with cognitive-behaviortherapy. Journal of Consulting and Clinical Psychology.65(5):878–882.
[2015] Timko C and DeBenedetti A (2007). A randomized controlled trial of intensive referral to Twelve Step self-help groups: one year outcomes.Drug and Alcohol Dependence.90(2-3):270–279. Vedel E, Emmelkamp PMG, Schippers GM (2008). Individual cognitive behavioral therapy and behavioural couples therapy in alcohol usedisorder: a comparative evaluation in community-based addiction treatment centres. Psychotherapy and Psychosomatics.77(5):280–288. Walitzer KS and Dermen KH (2004). Alcohol-focused spouse involvement and behavioral couples therapy: evaluation of enhancements todrinking reduction treatment for male problem drinkers. Journal of Consulting and Clinical Psychology.72(6):944-955. Walitzer KS, Dermen KH, Barrick C (2009). Facilitating involvement in Alcoholics Anonymous during out-patient treatment: a randomizedclinical trial. Addiction.104(3):391–401. Wiers RW, Eberl C, Rinck M, Becker ES, Lindenmeyer J (2011). Retraining Automatic Action Tendencies Changes Alcoholic Patients’ ApproachBias for Alcohol and Improves Treatment Outcome. Psychological Science.22(4):490 –497.PICO TablePopulation: People with alcohol dependenceInterventionMotivational enhancement therapy(MET)Cognitive behavioural therapy (CBT)ComparisonOutcomeIncluded studiesJustification for studyuseRelevantGRADE tableAbstinenceHester et al. (2005)Rosenblum et al.(2005b)Sellman et al. (2001)Studies met inclusioncriteriaTable 1Burtscheidt et al.(2001)Monti et al. (1993)Rosenblum et al.(2005b)Wiers et al. (2011)Alden et al. (1988)Monti et al. (1993)Studies met inclusioncriteriaTable 2Studies met inclusioncriteriaTable 3ControlAlcoholconsumptionTreatment as usual (TAU) orcontrolAlcoholconsumptionRelapseBehavioural therapiesControlAbstinenceAlcohol
[2015]consumptionSocial network therapyControlRelapseAbstinenceLitt et al. (2007)Study met inclusioncriteriaTable 4Litt et al. (2007)Study met inclusioncriteriaTable 5Alessi et al. (2007)Petry et al. (2000)Studies met inclusioncriteriaTable 6AlcoholconsumptionContingency olconsumptionTreatmentretentionContingency managementStandard care/treatment as eSellman et al. (2001)Studies met inclusioncriteriaTable 7Motivational enhancement therapy(MET)Twelve Step FacilitationAlcoholconsumptionAbstinenceMATCH (1997)Study met inclusioncriteriaMotivational enhancement therapy(MET)Cognitive behavioural therapyAbstinenceMATCH (1997)Study met inclusioncriteriaMotivational enhancement therapy(MET)Social behaviour and networktherapyAbstinenceUKATT (2005)Study met inclusioncriteriaAlcoholconsumptionAbstinenceNo GRADEtable (singlestudy)No GRADEtable (singlestudy)No GRADEtable (singlestudy)Davidson et al. (2007)Study met inclusioncriteriaCounsellingMotivational enhancement therapyBroad spectrum treatmentAlcoholconsumptionNo GRADEtable (singlestudy)
[2015]Twelve Step FacilitationTwelve Step FacilitationCBT (Easton 2007),MET and CBT (MATCH 1997),Easton et al. (2007)MATCH (1997)Studies met inclusioncriteriaTable 8Fals-Stewart et al.(2005)Fals-Stewart et al.(2006)Fals-Stewart et al.(2005)Study met inclusioncriteriaTable 9Study met inclusioncriteriaLam et al. (2009)Vedel et al. (2008)Studies met inclusioncriteriaNo GRADEtable (singlestudy)Table 10Eriksen et al. (1986)Litt et al. (2003)Studies met inclusioncriteriaTable 10AlcoholconsumptionSitharthan et al.(1997)Study met inclusioncriteriaNo GRADEtable (singlestudy)TreatmentretentionAbstinenceSandahl et al. (1998)Study met inclusioncriteriaNo GRADEtable ceAlden et al. (1988)Study met inclusioncriteriaCouples therapyAlcoholconsumptionAbstinenceNo GRADEtable (singlestudy)Walitzer et al. (2004)Study met inclusioncriteriaNo GRADEtable (singlestudy)Psychoeducational eTwelve Step FacilitationCouples therapyCognitive behavioural therapyCouples ceCognitive behavioural therapyAlcoholconsumptionCognitive behavioural therapyCognitive behavioural therapy (CBT)Behavioural therapyShort term psychodynamictherapyAlcoholconsumptionBehavioural therapiesBehavioural therapiesAlcoholconsumption
[2015]Couples therapyCouples therapyCounsellingMultimodal therapyCounsellingAbstinencePsychoeducation interventionTreatmentretentionAbstinenceMultimodal ncePsychoeducation sumptionTreatmentretentionO’Farrell et al. (1992)Study met inclusioncriteriaNo GRADEtable (singlestudy)Fals-Stewart et al.(2006)Study met inclusioncriteriaNo GRADEtable (singlestudy)John et al. (2003)Study met inclusioncriteriaNo GRADEtable (singlestudy)Davis et al. (2002)Study met inclusioncriteriaNo GRADEtable (singlestudy)Narrative table detailing the studies that went into the analysisStudy nameAlden et al.(1988)Study designRCTNot blindedParticipantsN 94Alessi et al.(2007)RCTNot blindedBurtscheidt etal. (2002)RCTNot blindedN 103Outpatients enteringtreatment who met diagnosticcriteria for cocaine, opiate andalcohol abuse or dependenceN 120100% dependentConnors et al.(2001)RCTNot blindedN 144Problem-drinking womenIntervention – Group 1Group 1Behavioural self-managementstrategiesGroup 1Standard treatmentIntervention – Group 2Group 2Modified developmentalcounsellingGroup 2Prize-based contingencymanagement (CM)Intervention – Group 3 / 4Group 3Waiting list controlNon-specific supportive therapyN 40Coping skills training26 weekly sessions, 100 minuteseachN 40Group 2DRT – 13 hoursBooster sessions – 8 hoursCognitive behavioural therapy26 weekly sessions, 100 minuteseachN 40Group 3DRT -13 hoursLife-skills training – 7 hoursBooster sessions – 8 hoursGroup 1Drinking-reduction treatment(DRT) – 13 hoursLife-skills training – 7 hours
[2015]Group 4DRT only – 13 hoursDavidson et al.(2007)RCTNot blindedN 149100% alcohol-dependentDavis et al.(2002)RCTNot blindedN 105Easton et al.(2007)RCTNot blindedEriksen et al.(1986)RCTBlindingunclearRCTNot blindedN 78Alcohol-dependent malesarrested for domestic violencewithin previous yearN 24Inpatients at alcoholismtreatment centreN 100Male alcoholic patientsN 100Non-sunstance-abusing femalepartnersGroup 1N 40CBT Substance Abuse DomesticViolence groupGroup 1Social Skills Training GroupN 138Female alcoholic patientsN 138Non-substance-abusing malepartners (married orcohabiting)N 61Minimum score of 8 in AlcoholGroup 1N 46Behavioural couples therapyplus individual-based treatmentGroup 2N 46Individual-based treatment onlyGroup 1 (N 35)Computer-based briefGroup 2 (N 26)Wait-list control groupFals-Stewartet al. (2005)Fals-Stewart etal. (2006)RCTNot blindedHester et al.(2005)RCTNot blindedGroup 1Cognitive behavioural therapyfor alcoholism broad spectrumtreatment, together with atherapeutic dose of naltrexoneGroup 1 (N 52)Standard outpatient treatmentstarted with a 3-weekorientation period consisting ofsix group therapy sessions, threealcohol education sessions inwhich alcohol education filmswere shown, three leisureeducation sessions, threecommunity meetings, and aminimum of six AA meetingsGroup 1Brief relationship therapyGroup 2Motivational-enhancementtherapy, together with therapeuticdose of naltrexoneGroup 2 (N 53)Minimal treatmentpatients were assigned to view analcoholism education movie oneevening a week at 17:00. in agroup setting, but with nodiscussion afterwards except foronce a month, when a therapistjoined the group, obtainedinformation about the patients'sobriety, and led a discussion ofthe movieGroup 2N 38Twelve Step Facilitation groupGroup 2Control GroupGroup 2Standard behavioural couplestherapyGroup 3Individual-based treatmentGroup 4Psychoeducational attentioncontrol treatmentGroup 3N 46Psychoeducational attentioncontrol treatment
[2015]Use Disorders Inventory Test(AUDIT)N 322Alcohol-dependent in-patientsat psychiatric hospitalJohn et al.(2003)RCTNot blindedLam et al.(2009)RCTNot blindedN 30Male participants enteringoutpatient alcohol treatment,their female partners and acustodial child (8-12 years old)Litt et al.(2003)RCTNot blindedN 128Alcohol-dependent men andwomenLitt et al.(2007)RCTNot blindedMarques et al.(2001)RCTNot blindedN 210Alcohol-dependend men andwomenN 155Alcohol and/or drugdependent patientsmotivational intervention(Drinker’s Check-Up)Group 1 (N 161)Individual counsellingthree individual counsellingsessions on their ward inaddition to detoxificationtreatmentGroup 1N 10Parent Skills with BehavioralCouples TherapyBoth partners attended 12PSBCT treatmentsessions, which included 6 coreBCT sessions and 6parent-skills training sessions.The parent training moduleand materials were adaptedfrom Forehand’s programdescribed in Helping theNoncompliant Child (Forehandand Long, 2002; McMahon andForehand, 2003), which hasestablished effectiveness atimproving parenting andchild functioning (Forehand,Rogers, McMahon, Wells,& Griest, 1981; Jones et al.,2005).Group 1Cognitive-behavioural treatmentintended to develop coping skills(26 weeks)Group 1Network supportGroup 1N 77Individual treatment in 2phases:Group 2 (N 161)Group treatment programme2 weeks of in-patient treatmentand four out-patient groupsessions in addition todetoxificationGroup 2N 10Behavioral Couples TherapyBoth partnersattended 12 manualized BCTsessions, which includedcollecting urine screens, reviewingthe previous week’s homework,improving communication andproblemsolvingskills, and reinforcing sobriety(O’Farrell &Fals-Stewart, 2006).Group 2Interactional therapy intended toexamine interpersonalrelationships (26 weeks)Group 2Network support contingencymanagementGroup 2N 78Group treatment in 2 phases:Acquisition (8 sessions) andGroup 3N 10Individual-Based TreatmentOnly male patients participated inthe IBT condition;the nonsubstance-abusing femalepartners did not participate inthis standard clinicalintervention. TheIBT condition included 12individual-based copingskills sessions modified fromMonti et al.’s (1989) cognitivebehavioral treatment foralcoholism.Group 3Case management (control)
[2015]Match (1997)TwoindependentRCTsNot blindedMonti 1990RCTNot blindedMonti et al.(1993)RCTBlindingunclearN 952; 72% males; alcoholdependent, in outpatienttherapyN 774; 80% males; clientsreceiving aftercare therapyfollowing inpatient or dayhospital treatmentN 69Male alcoholics in standardinpatient treatmentN 40Males; mean age of 42.9 -12.7years; 33.3% married orcohabiting; 94% White, 6%Black; Mean score on AlcoholDependence Scale 20.7 -9.0and on Short MichiganAlcoholism Screening Test9.97 -2.42; during 6 monthsprior to treatment consumedmean of 12.1 -12.3 drinks perpossible drinking day, wereabstinent 47% -38% ofpossible drinking days anddrank heavily on 45% -39% ofpossible drinking days;included if they met DSM-III-Rcriteria for alcohol dependenceand if they drank heavily theweek prior to admission.Acquisition (8 sessions) andmaintenance (9 sessions) overan 8-month periodGroup 1Cognitive Behavioural CopingSkills Therapy (12 weeks)maintenance (9 sessions) over an8-month periodGroup 2Motivational EnhancementTherapy (12 weeks)Group 3Twelve-Step Facilitation Therapy(12 weeks)Group 1Communication skills traininggroupGroup 1N 22Cue exposure treatment6 individual treatment sessions,55-minutes long, within a 2week periodTreatment sessions started bycompleting daily urge ratings;then presenting most frequentlyconsumed beverages, whichremained present throughoutthe session; identification ofdrinking trigger situations;constant reporting of urge todrink until peak was reached,then terminating beverageexposure when urge diminishedto at least half of peak urgevalue. Five coping skills weretaught gradually, first one at atime and in the final 2 sessionspatients were encouraged toselect and combine theirpreferred strategies.Group 2Communication skills traininggroup with family participationGroup 2N 18Contrast conditionDesigned to control for dailycontract. Patients receivedstandard treatment, participatedin all pre-, post-, and follow-upassessment protocols and on adaily basis in a 10-min interviewgave a treatment provider dailyurge ratings.Group 3Cognitive behavioural moodmanagement training group
[2015]Morgestern etal. (2007)RCTNot blindedN 89HIV-negative men who havesex with men with alcohol-usedisordersGroup 14 sessions of motivationalinterviewingGroup 212 sessions of combinedmotivational interviewing andcoping skills trainingO’Farrell et al.(1992)RCTNot blindedN 36Group 1No marital treatment controlgroupGroup 2Behaviour marital therapy10 weekly sessionsPetry et al.(2000)RCTNot blindedN 42Alcohol-dependent veteransGroup 1Standard treatmentRosenblum etal. (2005a)RCTNot blindedN 230Rosenblum etal. (2005b)RCTNot blindedN 290Soup kitchen guests whoreported drug or alcoholproblems; mean age 42; 82%male; 68% African-American;81% unstable residence; 14%HIV .Group 1n 114Cognitive behavioural therapyTwo treatments a week for 10weeks; 15-week follow-upGroup 1n 139Information and referral pluspeer advocacy (control)Sandahl et al.(1998)RCTNot blindedN 49Moderately alcohol-dependentmale (44%) and female (56%)patients (diagnosed by DSMIII-R)Sellman et al.(2001)RCT6-monthfollow-up.Outcomeassessmentwas blind totreatmentallocation.N 122Patients with mild to moderatealcohol dependenceGroup 2Standard treatment pluscontingency management (CM)Group 2n 116Group motivational interventionTwo treatments a week for 10weeks; 15-week follow-upGroup 2n 15112-session motivational group (3sessions/week for 3 weeks)followed by 36-session cognitivebehavioural group (3sessions/week for 12 weeks) plusinformation and referral and peeradvocacy.Group 2n 25Psychodynamically oriented timelimited group treatment (PD)15 weekly 90-minute groupsessions, average number ofsessions attended was 8.9Group 2 (N 40)Nondirective reflective listening(NDRL)4 sessionsNonstrategic reflective listeningwithin a therapeutic venue inwhich subjects were invited to talkabout anything they wanted, notGroup 1n 24Cognitive behavioural treatment(CB)15 weekly 90-minute groupsessions, average number ofsessions attended was 9.5Group 1 (N 42)Motivational EnhancementTherapy4 sessionsMotivational enhancementtherapy (MET) was very similarto that used in Project MATCH(Miller et al., 1992), guided byGroup 3N 109Declined treatment but werefollowed as a non-help-seekinggroupGroup 3Interactional couples therapygroup10 weekly sessionsGroup 3 (N 40)No further counselling
[2015]Shakeshaft2002RCTNot blindedN 295Patients attending communitybased drug and alcoholcounselling in AustraliaSitharthan etal. (1997)RCTNot blindedTimko et al.(2007)RCTNot blindedUKATT (2005)RCTNot blindedN 52Problem drinkers whorequested moderationdrinking goalN 345Individuals with substance usedisorders enterning a newoutpatient treatment episodeN 742Vedel et al.RCTN 64five key principles (Miller andRollnick, 1991)— expressingempathy, deploying discrepancy,avoidingargumentation, rolling withresistance and supporting selfefficacy—and introducing aseries of specific strategieswithin two major phases oftherapy: Phase 1 - Buildingmotivation for change and Phase2 - Strengthening commitment tochangeGroup 1Brief Intervention90 minutes of face-to-face timecomprising the followingelements: feedback,responsibility, advice, menu,empathy, self-efficacyGroup 1Modified cue exposure (CE)6 90-minute group sessionsGroup 1n 164Standard referralGroup 1 (N 320)Social behaviour and networktherapycomprises cognitive andbehavioural strategies to helpclients build social networkssupportive of change. In our trialthe therapy comprised eight 50minute sessions over eight to 12weeksGroup 1necessarily issues related todrinking. The direction of contentthroughout the treatment wasintentionally left for subjects todetermine.Group 2Cognitive-behavioural therapy6 45-minute weekly sessions onthe topics: introduction; cravingsand urges; managing crises; saying‘no’and solving problems;emergencies and lapses; andmaintenance.Group 2Standard cognitive behaviourtherapy (CBT)6 90-minute group sessionsGroup 2n 181Intensive referral to self-helpGroup 2 (N 442)Motivational enhancementtherapycomprised three 50 minutesessions over eight to 12 weeks. Itcombined counselling in themotivational style with objectivefeedback.Group 2
[2015](2008)Not blindedMale (55) and female (9)people with alcoholdependence and their partnersbeing treated for alcohol usedisorders in communitytreatment centres; mean age45.5 years; alcohol abuse ordependence diagnosis withDSM-IVN 64Male clients and their femalepartnersn 30Stand-alone behavioural couplestherapy (BCT)10 sessions of 90 minutes each,over a 5 to 6-month periodn 34Individual cognitive-behaviouraltherapy (CBT)10 sessions of 45-60 minutes each,over a 5 to 6-month periodWalitzer et al.(2004)RCTNot blindedGroup 1Treatment for problem drinkersonly (PDO)Group 2Couples alcohol-focused treatmentWalitzer et al.(2009)RCTNot blindedN 169Alcoholic out-patients; 57womenRCTNot blindedN 214 alcoholic inpatientsGroup 1n 53Twelve Step directive approachto facilitating AA involvement12-sessions (1st one 90 minutes,others 60 minutes)Group 1Control 1 – No trainingFour brief session ofexperimental cognitive-biasmodification (CBM) beforeregular inpatient treatmentGroup 2n 58Motivational enhancementapproach to facilitating AA12-sessions (first one 90 minutes,others 60 minutes)Group 2Control 2 – Sham trainingFour brief session of experimentalcognitive-bias modification (CBM)before regular inpatient treatmentWiers et al.(2011)Group 3Couples alcohol-focusedtreatment Behavioural couplestherapy (BCT)Group 3n 58Treatment as usual with noemphasis on AA12-sessions (first one 90 minutes,others 60 minutes)Group 3Experimental 1 – explicitlytrained to make avoidancemovements in response to alcoholpicturesFour brief session ofexperimental CBM before regularinpatient treatmentGroup 4Experimental 2 – implicit trainingFour brief session ofexperimental CBM before regularinpatient treatment
[2015]GRADE TABLESPsychotherapy vs. control or treatment as usual (TAU)Table 1. Motivational enhancement therapy (MET) vs. controlAuthors: N Clark and J Vieira FloresQuestion: Should motivational techniques vs control be used for management of alcohol dependence?Bibliography: National Collaborating Centre for Mental Health. 2011. Diagnosis, assessment and management of harmful drinking and alcohol dependence - National Clinical Practice Guideline [CG115].London: The British Psychological Society and The Royal College of Psychiatrists. Included studies: Hester RK, Squires DD, Delaney HD (2005). The Drinker’s Check-up: 12-month outcomes of a controlled clinical trial of a stand-alone software program for problem drinkers. Journal of SubstanceAbuse Treatment.28(2):159-169. Rosenblum A, Cleland C, Magura S, Mahmood D, Kosanke N (2005). Moderators of effects of motivational enhancements to cognitive behavioural therapy. The American Journal of Drug andAlcohol Abuse.31(1):35–58. Sellman JD, Sullivan PF, Dore GM, Adamson SJ, Ma
Vedel E, Emmelkamp PMG, Schippers GM (2008). Individual cognitive behavioral therapy and behavioural couples therapy in alcohol use disorder: a comparative evaluation in community-based addiction treatment centres. Psychotherapy and Psycho