Transcription
TL1TL1: Provide one example, with supporting evidence, of an initiative in nursingpractice that is consistent with the organization’s mission statement. Provide a copy of the organization’s mission statement as one of thesupporting documents.Parenteral Opioid ShortageMission of UVA Health SystemTo provide excellence, innovation and superlative quality in the care of patients, thetraining of health professionals, and the creation and sharing of health knowledge withina culture that promotes equity, diversity and inclusiveness. [Exhibit TL1.a. MissionStatement screenshot from UVA Health System website.]In early March 2018, UVA Health System began planning for a looming nationalparenteral opioid shortage. As an organization that provides more than 1,500 surgicalprocedures each month, one of the greatest concerns was the management of postoperative pain.The Opioid Shortage Task Force was an interprofessional team formed to quicklyassess the potential impact of the parenteral opioid shortage and develop action plansfor each phase of care. The group consisted of experts from across the health systemwho provided insight on logistics, Epic needs and tools, medication availability andsupply, as well as physician and nursing practice. One phase of care of particularconcern was the immediate post-operative phase in the Post-Anesthesia Care Unit(PACU).TL1 Table 1. Participants: Opioid Shortage Task ForceNameKate Bidwell HortonDisciplinePharmacyNursingTitleMedication Use PolicyCoordinatorAssistant Nurse ManagerDepartmentMedical Useand PolicyPACUEleanor Bergland, MSN,RN, CPANLaurie Brock, MSN, RNMark ChabotAngel Cyphert, MSN, RN,CNMLC. Page Dunbar, MSN,RN, FNP-BC, urse ian 3EnhancedRecoveryAfter Surgery(ERAS)PACUNancy Farish, BSN, RN,BC-PMKatelyn HipwellPharmacyManagerPharmacy1
TL1Steve Morton, BSN, RN,RN-BCKathleen Rea, DNP, RN,ACNS-BC, PCCN, CNLGeorge Rich, MDReza Salajegheh, MDBethany Sarosiek, MSN,RN, CNLJennifer SimpsonAnne Stadelmaier, BSN,RN, RN-BCKaren Thomas, BSN, RN,CNMLNursingClinician 4NursingAPN3-CNSAcute PainService (APS)5 CentralPhysicianPhysicianNursingProfessorAssistant ProfessorERAS Program l PharmacistClinician 3PharmacyPACUNursingNurse ManagerSurgicalAdmissionSuite (SAS),PreanesthesiaTesting Center(PETC)The primary concern of the task force was maintaining pain control in post-operativepatients. They evaluated options available throughout the continuum of care with aprimary goal to reduce the amount of intravenous (IV) rescue opioids, measured inmorphine milli-equivalents (MME), needed in the PACU. To facilitate changes in bothmedical and nursing practice, new ordering pathways and practice-guiding resourcetools were developed.New order sets were built in Epic to support the following: pre-operative phase: long-acting opioids post-operative phase: multimodal pain management options includingo oral medications as first-line rescueo non-opioid medicationsExhibit TL1.b. is a March 30, 2018 email from C. Page Dunbar, MSN, RN, FNP-BC,RN-BC, RNC-OB, APN1-NP with the ERAS program. She sent a draft of the order setsdeveloped by the task force and invited feedback from the group.Nancy Farish, BSN, RN, BC-PM, Clinician 3; Anne Stadelmaier, BSN, RN, RN-BC,Clinician 3; Eleanor Bergland, MSN, RN, CPAN, PACU Assistant Nurse Manager; andAngel Cyphert, MSN, RN, CNML, PACU Nurse Manager, focused on the immediatepost-operative phase of care in the PACU setting. The specific nursing practices theysought to address in the PACU were pain assessment, intervention and patienteducation.2
TL1Nancy and Anne, both of whom are certified in pain management, served as expertsand leaders in the PACU to facilitate the changes in nursing practice. As members ofthe task force, they advocated for the tools that the PACU team needed, andcommunicated and educated interprofessional colleagues as the changes weredeployed.Nancy and Anne collaborated with Steve Morton, BSN, RN, RN-BC, Clinician 4, with theAcute Pain Service, who developed an opioid shortage clinical decision-makingresource for use in the PACU. This flow-chart tool helped nurses evaluate optionsbased on yes/no questions about the patient’s status. Exhibit TL1.c. is a March 23,2018 email from Steve to Angel, Nancy and Anne, sharing the tool.They invested significant time in information sharing and educating team membersabout the work of the task force, the changes in pathways and tools, as well as newlyrevised nursing practices. Communication avenues included: Staff and shared governance meetings during April and May 2018 [ExhibitTL1.d. May 9, 2018 PACU Shared Governance meeting minutes] Email communications to the team daily from April 16 through May 16, thenweekly Daily team huddles from April 16 through May 16, then weekly One-on-one conversations within the practice environment to reinforceinformation sharing and answer questionsTopics included in the team communications: Changes in Epic order sets Emphasis on comprehensive initial pain assessments and pain reassessments Non-pharmacological interventions such as dimming of lights, positioning,application of heat/ice as appropriate and providing the option of music viaheadphones Early involvement of the patient’s family as soon as possible Alternative non-opioid pharmacologic interventions Review of pharmacology to reinforce understanding of the new order sets andoptions Patient education: how to help reinforce preoperative teaching and how toexplain changes in pain management interventions, especially if they havereceived IV opioids with previous surgeriesExhibit TL1.e. is an April 13, 2018 email from CNO Mary Dixon, MSN, RN, NEA-BC, toall registered nurses and nursing leaders within the organization, communicating anoverview of the task force work and a link to a newly created patient educationresource.3
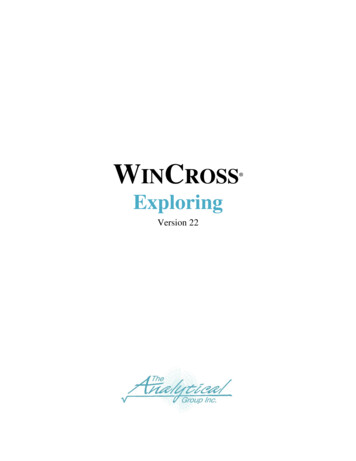
TL1On April 16, the revised order sets were implemented. Nancy and Anne activelysupported their colleagues as the PACU team changed nursing practices related to painassessment, intervention and patient education. Capitalizing on the collective expertiseof the Opioid Shortage Task Force and the leadership provided by Nancy and Anne, thePACU demonstrated a successful reduction in the use of parenteral opioids andmaintained patient satisfaction with pain control.TL1 Figure 1. Average Morphine Milliequivalents (MME) and Pain Scores in PACU,January-June 2018Average Morphine Milligram Equivalents (MME) and Pain ScoresPACU8257.5Average MMEPractice Change:April 16, 2018156.565.51054.55Average Pain Scores72043.50Jan 2018Feb 2018Mar 2018Apr 2018May 2018Jun 3.73.583.613.833The PACU RNs participated in a survey in November 2018 to evaluate this change innursing practice. The survey demonstrated the following related to frequency of use oforal opioids as a first line rescue pain medication route. Ninety-one percent of the PACURNs completed the survey.TL1 Table 2. PACU RN Survey Responses: “How Frequently Did You Use OralOpioids as a First Line Rescue Pain Medication Route?”Responsen 30 RNsPrior to 4
TL1November 2018 7%30%53%10%(6 months later)Additionally, the methods of education and practice change supports were evaluated.PACU RNs rated these four methods in Table 3 for greatest impact:TL1 Table 3. PACU RN Survey Responses: “Which Educational Methods HadGreatest Impact on Practice Change?”Responsen 27 RNsStaff Meeting DailyHuddlesEmails% statedgreatestimpact19%19%30%Point of CareAssistance fromColleagues63%Alignment with MissionFacets of the Opioid Shortage Task Force’s efforts speak to all aspects of the UVAHealth System mission: To provide excellence and superlative quality in the care of patients: In thecontext of a national parenteral opioid shortage, the nurses from the task force andPACU did not merely maintain pre-shortage effectiveness of post-operative painmanagement, they actually improved patients’ self-reported pain scores while usingfewer MME, as shown in TL1 Figure 1. To provide innovation in the care of patients: Nurses co-led the creation andimplementation of new multimodal pain management order sets and an opioidsparing decision-making flow chart (Exhibits TL1.b and TL1.c). The training of health professionals: Nurses actively led the development of trainingmaterials and educated both nurses and interprofessional colleagues on newprocesses and resources. TL1 Tables 2 and 3 are examples from the learners’perspective of how effectively the training impacted their practice. The creation and sharing of health knowledge: From a health literacy standpoint,new patient education approaches helped patients understand the empoweringbreadth of options being tailored to their individual needs while learning about thenational constraints driving the change. Within a culture that promotes equity, diversity and inclusiveness: The task forceleveraged the different role perspectives and expertise of a collaborativeinterprofessional team, resulting in a more comprehensive and successfulmultimodal pain management program than silos would have achieved.5
TL1Opioid Task Force members Nancy Farish, Steve Morton, and Anne Stadelmaier6
Nursing Assistant Nurse Manager PACU Laurie Brock, MSN , RN IT Informaticist Epic Mark Chabot Pharmacy Manager Pharmacy Angel Cyphert, MSN, RN, CNML Nursing Nurse Manager PACU C. Page Dunbar, MSN, RN, FNP-BC, RN-BC, RNC-OB Nursing APN1-NP Enhanced Recovery After Surgery (ERAS) Nancy Farish, BSN, RN, BC-PM Nursing Clinician 3 PACU