Transcription
Washington State Institute for Public Policy110 Fifth Avenue SE, Suite 214 PO Box 40999 Olympia, WA 98504 360.586.2677 www.wsipp.wa.govJuly 2015Involuntary Civil Commitments:Common Questions and a Review of State PracticesIn 2014 and 2015, the Washington StateLegislature directed the Washington StateInstitute for Public Policy (WSIPP) to reviewstate practices regarding civil commitmentsfor involuntary mental health treatment (seenext page). For a treatment commitment tooccur, the court must make a determinationthat as a result of a mental illness, anindividual poses a danger to self or others.SummaryThis review examines differences in state laws andprocedures for involuntarily committingindividuals who may be a danger to themselvesor others as a result of mental illness. Aninvoluntary civil commitment may involve a shortterm emergency detention, where an individual isheld in temporary custody to prevent harm tothemselves or others. At an initial commitmenthearing, the court may issue an involuntarytreatment order that mandates hospitalization orparticipation in an agreed outpatient treatmentplan. In a limited percentage of cases, anextended commitment may be necessary, if anindividual requires ongoing treatment andhospitalization.This review examines state variation in thecivil commitment process—from theinitiation of a petition to the discharge of apatient. We answer common questionsrelated to involuntary civil commitmentsand address how policy and practices differfrom state to state. We cover the legalrequirements for civil commitments, discusswho may initiate a petition, and detail howindividuals are deemed eligible forinvoluntary holds. We also outline thelength of time committed persons may beheld and discuss options courts use toensure committed persons receiveappropriate treatment in the least restrictivesetting available.The Washington State Legislature directed theWashington State Institute for Public Policy(WSIPP) to investigate state practices regardingdifferent aspects of the involuntary commitmentprocess. This paper discusses common questionsrelated to civil commitments and includes aTechnical Appendix with detail on commitmentlaws in each state. Our review notes how aspectsof these laws are implemented in various statesand compares these practices to the legalguidelines in effect in Washington State.A detailed Technical Appendix includes adescription and reference for the civilcommitment statutes in each state. TheTechnical Appendix also provides detailabout emergency detentions (which occurprior to a court hearing) and court-orderedhospitalizations or outpatient treatmentorders.Suggested citation: Burley, M., & Morris, M. (2015).Involuntary civil commitments: Common questions anda review of state practices (Document Number 15-073401). Olympia: Washington State Institute for PublicPolicy.1
I. BackgroundThe review presented here answerscommon questions related to civilcommitments and highlights practices incertain states. The questions include:The modern practice of civil commitmentbegan with the deinstitutionalization ofpsychiatric patients in the 1960s.1 Prior tothis time, doctors or psychiatrists wereresponsible for the decision to commitpatients for mental health treatment. In1975, however, the United States SupremeCourt ruled that a person may not be heldinvoluntarily if he or she does not present adanger to self or others.2 States respondedto this ruling by adopting legal criteria forwhat constitutes “dangerousness” and whois allowed to petition for involuntarytreatment based on these criteria.1. What is the legal basis for involuntaryhospitalization?2. Who can be involuntarily hospitalized?3. How is “grave disability” defined?4. What is the “need for treatment”standard?5. What are the stages in an involuntarycivil commitment?6. Who can initiate a civil commitment orinvoluntary hospitalization?7. How long does an emergency detentionor involuntary hospitalization last?Legislative AssignmentThe 2014 Washington State Legislaturedirected WSIPP to complete a comprehensivestudy of the crisis mental health andinvoluntary commitment system. The studyincludes “a review of practices in other statesregarding third-party initiation of a civilcommitment petition ”8. Are there alternatives to court-orderedcommitments to inpatient mental healthfacilities?9. What is assisted outpatient treatment?Who qualifies?10. How is compliance with outpatientorders determined?(2014 ESSB 6002)The 2015 Washington State Legislaturedirected WSIPP to investigate “approachesused in other states to monitor and enforceleast restrictive orders, including associatedcosts.”Detailed information on the civilcommitment process in each state isprovided in the Technical Appendix. Thisinformation was compiled from anexamination of statutes in each state and areview of relevant policy documents andeducational materials that describe statecommitment practices. A summary of statesthat have enacted specific provisionsdiscussed in this paper is also presented inExhibit 1 (page 9).(2015 ESSB 5649)1Testa, M., & West, S.G. (2010). Civil Commitment in theUnited States. Psychiatry (Edgemont), 7(10), 30–40.2O’Connor v. Donaldson, 422 U.S. 563, 575 (1975).2
State commitment criteria fordangerousness may also include theconsideration of whether harm to self orothers is imminent. In addition to thedangerousness criterion, 46 states also allowa person to be hospitalized if theydemonstrate a “grave disability” (asexplained below).1. What is the legal basis forinvoluntary hospitalization?The right to make personal treatmentdecisions is a fundamental principal ofhealth care law.3 However, when individualsare unable to make rational decisions andcare for themselves, the legal doctrine ofparens patrae (parent of the country)permits the state to intervene and act in thebest interests of the individual.4 In theTechnical Appendix we list the statutes ineach of the 50 states that authorizeinvoluntary mental health treatment. Sincethis power involves temporarily depriving anindividual of liberty, each state hasdeveloped specific criteria and due processprotections to authorize involuntarytreatment.2.Washington State statute includes bothcriteria—to be civilly committed, a personmust demonstrate a likelihood of seriousharm or a grave disability as a result ofmental illness. In Washington, the court mayalso consider the recent historical behaviorof an individual while making itsdetermination for hospitalization.53. How is “grave disability” defined?The grave disability criterion generallysupports a civil commitment if an inability tocare for basic needs would result in dangeror harm to the person. Individuals may bedeemed unable to care for themselves ifthey cannot meet personal needs includingbut not limited to food, shelter, clothing, ornecessary medical care. Most statutesprovide a strict interpretation of thisrequirement—individuals capable of“surviving safely in freedom” would not beconsidered gravely disabled.6Who can be involuntarilyhospitalized?While each state has its own statutorycriteria for involuntary hospitalization, allstates require that an individual have amental illness in order to be involuntarilyhospitalized. However, the presence ofmental illness alone is not sufficient forcommitment. All states also have thecriterion that an individual can becommitted if they are likely to cause seriousharm to self or others as a result of a mentalillness. The dangerous behavior may bedemonstrated by actual or perceived threatsof violence to self or others.3Coggon, J., & Miola, J. (2011). Autonomy, liberty, andMedical decision-making. Cambridge Law Journal, 70, 523547.4Appelbaum, P.S., & Gutheil, T.G. (1991). Clinical handbookof psychiatry and the law. Baltimore: Williams & Wilkins. Also,see Revised Code of Washington, RCW 71.05.010.563RCW 71.05.245.O’Connor v. Donaldson, 422 U.S. 563, 575 (1975).
In Washington State, gravely disabled isdefined as a condition in which a person,due to mental illness:treatment standard may only be used toorder compliance with an outpatienttreatment plan. Some states, such asArizona or Wisconsin, permit an inpatientcommitment petition based on a need fortreatment if the individual has a history ofpersistent or acute disability combined withprior hospitalizations.is in danger of serious physical harmresulting from a failure to provide for hisor her essential human needs of health orsafety; or manifests severe deteriorationin routine functioning evidenced byrepeated and escalating loss of cognitiveor volitional control over his or heractions and is not receiving such care asis essential for his or her health or safety.7The grave disability criterion inWashington’s inpatient commitment statutepermits hospitalization if a mentally illindividual has “severe deterioration inroutine functioning” that could interferewith the individual’s health or safety.Recently enacted legislation in Washingtonestablishes additional grounds under whichan individual may receive an outpatientcommitment order.8 The new standard inWashington applies to persons “in need ofassisted outpatient mental healthtreatment.” This standard authorizes an180-day less restrictive alternative (LRA)outpatient treatment order when a person:Our review of statutes identified only fourstates that do not include grave disabilitylanguage in their involuntary commitmentcode (Alabama, Delaware, Maryland, andNew York). Some states, such as Florida,provide an exception in their grave disabilityclause for individuals who have willing andresponsible friends and family available toprovide assistance.4. What is the “need for treatment”standard?According to our review, 23 states, includingWashington, have adopted various forms ofa “need for treatment” criterion for civilcommitment. States with a need fortreatment standard permit an involuntarytreatment order when an individual lacksinsight into his or her illness and cannotmake an informed decision aboutpsychiatric care. In these cases, a court maymake a determination that a refusal to seektreatment will result in psychological orphysical deterioration.has been previously involuntarilycommitted at least once during the past36 months; is unlikely to voluntarily participate inoutpatient treatment without atreatment order (based on previoushistory); and is judged to require outpatienttreatment to prevent relapse ordecompensation that is likely to result inserious harm or grave disability within ashort period of time.Wisconsin’s “fifth standard,” adopted in1996, was the first state statute to authorizecommitment orders for individuals that may“suffer severe mental, emotional, or physicalThis criterion is often used in limitedcircumstances, however. In states such asMinnesota and Montana, the need for7 RCW 71.05.020(17).842015 ESSB 1450 (effective July 24, 2015).
harm” without mental health treatment.The criterion was ruled constitutional by theWisconsin State Supreme Court in 2002.9Generally, an emergency detention does notentail a full court hearing but may require apsychiatrist or other mental healthprofessional to certify that the individualmeets commitment criteria.5. What are the stages in an involuntarycivil commitment?Involuntary treatment commitment. Aninvoluntary treatment commitment orderoccurs following an evaluation by medicalprofessionals and a court hearing todetermine whether an individual meets thestate’s criteria for involuntaryhospitalization. The criteria for emergencydetention and commitment orders may ormay not be the same depending on thestate. For example, laws in 16 states,including Washington, explicitly state that aperson can only be placed in temporarycustody if the officer (or designatedexaminer) determines that a detention isnecessary to prevent immediate danger orinjury.Civil commitments are intended to ensurethat individuals receive needed mentalhealth treatment and reduce the likelihoodthat dangerous events occur as a result ofuntreated mental disorders. The scope oftreatment ordered depends on both thelevel of psychiatric intervention necessaryand an assessment of the potential harminvolved. The civil commitment process caninvolve three types of legal commitments: emergency detention involuntary treatment commitment extended commitment10Emergency detention. An emergencydetention permits an individual to be held intemporary custody to prevent a currentthreat or dangerous situation. The custodytypically occurs in a hospital emergencydepartment or approved mental healthtreatment facility.Washington State draws a further distinctionbetween emergent and non-emergentdetentions. An emergent detention requiresthe presence of an “imminent likelihood ofserious harm” for a temporary hold.11 In anon-emergent situation, a judicial officermust issue an order to detain for involuntarytreatment evaluation.12Ten states, including Washington, explicitlystate that the risk of harm must be“imminent” for an emergency detention tooccur. Most statutes include some type oflanguage requiring likelihood of harm“immediately” or “in the near future” toauthorize emergency involuntaryhospitalization.After the set period of temporary custody, acourt may make a determination if acontinued involuntary commitment isappropriate at an initial commitmenthearing. Not all states require a courthearing for an involuntary hospitalization.In New York, for example, if two physicianscertify that an individual meets criteria forinvoluntary treatment, that person can beheld for 60 days without a court hearing. AIn re Commitment of Dennis H., 647 N.W.2d 851 (Wis.2002).10Individuals subject to commitment proceedings will notnecessarily encounter all three stages.911125RCW 71.05.153.RCW 71.05.150.
hearing is only held if the individual or anadvocate for the patient petitions the courtfor a hearing. In South Dakota, involuntarycommitments are heard by a Mental IllnessBoard rather than the court.formal application for an emergencydetention.14 In the remaining states, theinitiation of a petition is limited to certainparties such as attorneys, health and socialservice professionals, law enforcementofficers, and medical and mental healthclinicians.In Washington, commitment hearingsusually take place in a county SuperiorCourt. Certain counties in Washington (suchas King County) have established MentalIllness Courts where a judicial officer hearscases with the medical center or hospital.13Upon a hearing or review of the petition, thecourt issues a warrant (or order) whichusually permits law enforcement officers totake the individual into custody andtransport him or her to a designatedtreatment facility. Once the individualarrives at the facility, he or she is examinedby a certified medical or mental healthprofessional. Most states, includingWashington, require that mental healthevaluations take place within the first 24hours after arrival.15 Massachusetts statuterequires an evaluation in the first two hours,while the law in Nebraska permits anindividual to be held in temporary custodyfor 36 hours prior to an evaluation.Extended commitment. An extendedcommitment occurs when a patient is foundto need ongoing treatment following theirinitial hospitalization and treatment order.Typically, the treating physician orpsychiatrist would petition the court,claiming the individual continues to meetcommitment criteria and requires furthertreatment. Both parties are represented bycounsel at a formal court hearing, and insome states, a jury (rather than judge) maydecide if an extended commitment isnecessary.If the evaluator determines the individualmeets the state’s criteria for involuntarytreatment, that person may continue to beheld until an initial commitment hearingtakes place. At the initial commitmenthearing, a judicial officer reviews the mentalhealth examination and hears evidence onthe alleged need for involuntary treatment.While initial commitments usually take placein a community hospital or treatmentfacility, extended commitments often occurin a state psychiatric hospital. InWashington, individuals with extended (90or 180-day) inpatient commitments areadmitted to Western or Eastern StateHospitals.An initial commitment hearing may occureven if the individual has not been held inemergency detention. In 32 states, includingWashington, interested adults may file a6. Who can initiate a civil commitmentor involuntary hospitalization?In 39 states, including Washington, an“interested” adult can submit a petition or14Recent changes to Washington’s civil commitment law(Engrossed Second Substitute Senate Bill 5269, Chapter 150,Laws of 2015) permit an immediate family member orguardian to petition the court for review of a decision not todetain an individual for involuntary evaluation and treatment.15See RCW 71.05.210 and 71.05.153 –The 24-hour timeperiod in Washington starts after medical periorCourt/ITACourt.aspx6
petition with the court for an involuntarytreatment commitment. In other states, suchas Arizona, Colorado, Georgia, Montana,and New Mexico, a petition for courtordered treatment is filed by the countyattorney, treating physician, or facilityadministrator.7. How long does an emergencydetention or involuntaryhospitalization last?In 28 states, including Washington, mentallyill persons requiring treatment can be heldfor up to 72 hours (three days) whileawaiting an initial court hearing. The lengthof this emergency detention is longer,however, in other states. A person mayremain in emergency custody for seven daysin Alabama, Nebraska, New Mexico, andNorth Dakota and up to ten days inMaryland, North Carolina, Rhode Island, andUtah. In New Jersey, a hearing can takeplace up to 20 days following an emergencydetention.Historically, in Washington State, onlyphysicians or designated mental healthprofessionals (DMHPs) could initiate apetition for involuntary commitment. In2015, however, the state’s InvoluntaryTreatment Act was amended to permit animmediate family member or guardian tofile an appeal if a DMHP decided not tohave a person detained for evaluation andtreatment.16At the initial hearing, the court may order acommitment for involuntary hospitalizationand treatment. In Washington, this initialinvoluntary commitment may last for up to14 days. Following that time, an extended90-day treatment commitment may beordered by the court. California and NorthDakota have similar 14-day initialcommitment periods.Other states have similar restrictions onthird party petitions. While petitions can befiled by a third party in Wisconsin, thepetition would only be heard if the countyattorney agreed. In 2014, Wisconsinchanged this process and required countycounsel to proceed with the petition undera limited appearance if there isdisagreement about probable cause for acommitment.17 In Minnesota, a petitionscreening team (PST) must initiate anemergency detention. A third-party canappeal the PST decision or decide to file apetition for a court-ordered judicial hold.18Tennessee has a similar law requiring aMandatory Prescreening Agent (MPA) tocertify an emergency detention.States may not necessarily distinguishbetween an initial and extendedcommitment. A 90-day treatmentcommitment is common in many states. Theinitial order may last for up to six months(180 days) in eight different states. In Idaho,the initial commitment can last for up toone year. Connecticut law does not specify alength of time for the initial commitmentbut permits petitions for release andrequires annual reviews to determine ifcommitment is still necessary.16The appeal must be decided within five days. SeeEngrossed Substitute Senate Bill 5269, Chapter 258, Laws of2015.17Wisconsin Act actmemo/act34018MINN. STAT. § 253B.7
8. Are there alternatives to courtordered commitments to inpatientmental health facilities?9. What is assisted outpatienttreatment? Who qualifies?Legal commitments that occur on anoutpatient basis are often referred to asassisted outpatient treatment (AOT). AOTorders require that an individual complywith a community-based treatment planunder the supervision of a designatedtreatment agency. The court-orderedtreatment plan may include psychotherapyappointments, medication management andmonitoring, and regular alcohol and drugtesting.The United States Supreme Court ruled inthe mid-1960s that an involuntarycommitment must take place in the “leastrestrictive” treatment setting that wouldbenefit the patient.19 Subsequent rulingsaffirmed the responsibility of the states toprovide treatment in a community settingfor non-dangerous psychiatric patients.20Consequently, all states have a requirementthat a commitment order occur in the leastrestrictive treatment setting available.Outpatient commitment orders are timelimited, but typically last longer than aninpatient commitment order. The criteria foroutpatient commitment are generally thesame as inpatient orders, but in some states,patients must meet additional requirementsto receive an AOT order.Nearly all states, including Washington,include options for civil commitments totake place in an outpatient treatmentsetting, rather than in a hospital.Connecticut, Maryland, Massachusetts, andNew Mexico are the four states that do nothave any statutory provisions for outpatientcommitments. In the remaining states,outpatient treatment may be ordered ifcommunity services are available anddeemed by a court to be appropriate.In Arizona and Kansas, for example, thecourt must find that an individual will notpose a danger to the community whilesubject to an outpatient treatment order.Outpatient commitment laws in certainstates, such as Florida and Maine, state thatcommunity treatment is reserved forpatients with a history of treatmentnoncompliance that may be at risk ofrelapsing without community supervision.In Washington, the 2015 Legislature enacteda new commitment criterion for persons “inneed of assisted outpatient treatment”.21This standard permits a less restrictive,outpatient treatment order in lieu of aninitial (72-hour) inpatient commitment if theindividual meets specified criteria.221921Lake v. Cameron, 364 F.2d 657 (1966).Lessard v. Schmidt 349 F. Supp. 1078 (E.D. Wis. 972) andOlmstead v. L.C., 527 U.S. 581 (1999).Engrossed Second Substitute House Bill 1450, Chapter150, Laws of 2015.22RCW 71.05.020 and RCW 71.05.212.208
10. How is compliance with outpatientorders determined?An AOT order usually requires a designatedperson or agency take responsibility forproviding treatment and oversight.Monitoring and enforcement of theseorders, however, varies significantly betweenstates. Our review found 41 of 46 statesauthorizing outpatient treatment includestatutory provisions for monitoring orenforcement.23 Information about the costsassociated with supervising and enforcingAOT orders is limited. Small-scale studieshave found that the non-compliance ratewith these orders varies from 5%-20% ofaffected patients.24In most statutes, cases of non-compliancerequire the designated treatment agency orperson to notify the court. The court maythen issue an order for law enforcement todetain the person for an evaluation. Statelaw in Alaska, Illinois, and South Dakotapermit the treatment agency to make adirect request to law enforcement officers totake non-compliant individuals into custody.At a status hearing, the court could ordermodifications to the outpatient treatmentplan or order an inpatient hospitalcommitment.Washington State’s new AOT law authorizesthe DMHP and agency overseeing treatmentto take a number of actions to enforcecompliance with an AOT order.25 Theseactions range include offering complianceincentives, increasing intensity of treatment,requesting a court review for modification,and having person transported for inpatientevaluation and assessment.Exhibit 1State Counts for Key Civil Commitment Criteria/ProceduresCivil commitment criterionNumber of statesWashington?Grave disability criterion46YesNeed for treatment criterion23YesImmediate danger for emergency detention16YesThird party filing for emergency detention39YesThird party filing for involuntary treatment32YesOutpatient commitment option46YesStatute for outpatient non-compliance41Yes23Arkansas, Colorado, Delaware, Hawaii, and Rhode Island.A Guide for Implementing Assisted Outpatient Treatment,June 2012. Downloaded ngrossed Second Substitute House Bill 1450, Chapter150, Laws of 2015.State counts based on WSIPP review and interpretation of state civil commitment statutes as of May 2015.For additional information, please consult Technical Appendix 9to this report.
Techn ica l A ppen dixInvoluntary Civil Commitments—Common Questions and Review of State PracticesAppendixA. I.A. II.State Inventory of Key Civil Commitment Criterion/Procedures 11State Statutory Detail on Emergency Detention and Civil Commitments . . . .1310
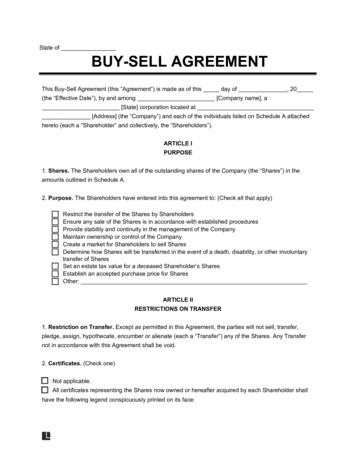
AppendixA. II. (continued)AppendixA. II.StateInventoryofKeyCivilCommitmentState Inventory of Key Civil HampshireCaliforniaNew JerseyColoradoNewMexicoConnecticutNew YorkDelawareNorthCarolinaFloridaNorth PennsylvaniaIndianaIslandRhodeIowa disabilityXX XXXXXXXXXXXXXXXXXXXX XX XXXXXXXXXXXXXXXX ttreatmentOutpatienttreatmentNonNonNeedEmergency InvoluntaryInvoluntary CommitmentCommitmentNeedforfor Emergencycompliancecompliancetreatment detentiondetention uteXXXXXXXXXXXXX XXXXXXXXXXXXXXXNotes:Notes:State inventory based on WSIPP review and interpretation of state civil commitment statutes as of May 2015. For additional information,State inventory based on WSIPP review and interpretation of state civil11commitment statutes as of May 2015. For additional information,please see Technical Appendix.please see Technical Appendix.11
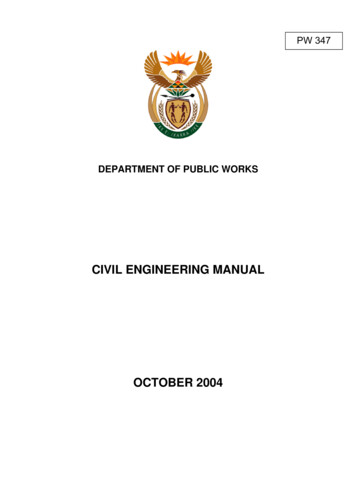
Appendix A. II. (Continued)State Inventory of Key Civil Commitment Criterion/ProceduresCommitment criterionStateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaRhode IslandSouth CarolinaSouth est XXXXXXXXXXXXXNeed fortreatmentThird party ent oncompliancestatuteXXXXXXXXXXXXXXXXXXXXXXX12 civil commitment statutes as of May 2015. For additional information,Notes: State inventory based on WSIPP review and interpretation of stateplease see Technical Appendix.12
A. II. State Statutory Detail on Emergency Detention and Civil CommitmentsOur review of each state statute on civil commitment is included in the following appendix. The review wasconducted through an online search related to relevant documents for “civil commitment,” “involuntarycommitment,” “involuntary treatment,” and “involuntary hospitalization.” We also carefully reviewed statutesavailable in each state (as of May 2015) and provide a statutory reference and online citation for each state.In some cases, statutory language may be paraphrased or summarized for purposes of clarity and brevity. Whilethe authors made every effort to provide a complete and accurate interpretation of these statutes, the informationwas not reviewed by state officials. For more detailed information about civil commitment process andprocedures, readers may want to contact experts in a given state.13
Alabama Civil Commitment LawsEmergency detentionWho may detain?Law enforcement officer or assessment of community mental health officerThird partyinvolvementNoLegal criteriaMentally ill and poses an immediate danger to self or othersMaximum time heldbefore hearingStatute7 days until probable cause hearing; 30 days until final hearingALA. CODE § 22-52-91(a); § 22-52-7(b); § 22-52-8Treatment commitmentThird party filing?Legal criteria same as emergencycriteria?.grave disability?.need for treatment?Length of initial orderLength of renewalStatuteYes(i) the respondent is mentally ill;(ii) as a result of the mental illness the respondent poses a real and present threat ofsubstantial harm to self and/or others;(iii) the respondent will, if not treated, continue to suffer mental distress and will continueto experience deterioration of the ability to function independently; and(iv) the respondent is unable to make a rational and informed decision as to whether ornot treatment for mental illness would be desirable.NoNo—"substantial harm to self and/or others"No—criteria for inability to make treatment decisions, but this criteria must beaccompanied by threat150 daysState may petition for renewal within 30 days of previous order expiring (renewalscannot exceed one year)ALA. CODE § 22-52-10.4; § 22-52-1.2; § 22-52-10.4(b)Outpatient treatment (least restrictive alternatives)StatuteA respondent may be committed to outpatient treatment if the probate court finds,based upon clear and convincing evidence, that:(i) the respondent is mentally ill;(ii) as a result of the mental illness the respondent will, if not treated, continue to suffermental distress and will continue to experience deterioration of the ability to functionindependently; and(iii
180-day less restrictive alternative (LRA) outpatient treatment order when a person: has been previously involuntarily committed at least once during the past 36 months; is unlikely to voluntarily participate in outpatient treatment without a treatment order (based on previous history); and is judged to require outpatient