Transcription
Original PapersThe effect of educationalintervention on interculturalcommunication:results of a randomised controlled trialHans Harmsen, Roos Bernsen, Ludwien Meeuwesen, Siep Thomas,Govert Dorrenboom, David Pinto and Marc BruijnzeelsINTRODUCTIONABSTRACTBackgroundDue to worldwide migration to Western countries,physicians are increasingly encountering patients withdifferent ethnic backgrounds. Communicationproblems can arise as a result of differences in culturalbackgrounds and poor language proficiency.AimsTo assess the effectiveness of an educational interventionon intercultural communication aimed to decreaseinequalities in care provided between Western and nonWestern patients.Design of studyA randomised controlled trial with randomisation at theGP level and outcome measurements at the patient level.SettingGeneral practice in Rotterdam.MethodThirty-eight Dutch GPs in the Rotterdam region, with atleast 25% of inhabitants of non-Western origin, and 2407visiting patients were invited to participate in the study. Atotal of 986 consultations were finally included. The GPswere educated about cultural differences and trained inintercultural communication. Patients received avideotaped instruction focusing on how to communicatewith their GP in a direct way. The primary outcomemeasure was mutual understanding and the secondaryoutcomes were patient’s satisfaction and perceivedquality of care. The intervention effect was assessed forall patients together, for the ‘Western’ and ‘non-Western’patients, and for patients with different culturalbackgrounds separately.ResultsAn intervention effect was seen 6 months after theintervention, as improvement in mutual understanding(and some improvement in perceived quality of care) inconsultations with ‘non-Western’ patients.ConclusionsA double intervention on intercultural communicationgiven to both physician and patient decreases the gap inquality of care between ‘Western’ and ‘non-Western’patients.Keywordscommunication; cultural differences; ethnicity; quality ofcare; randomised controlled trial.Worldwide migration induces multicultural contactsin societies, including health care. However,multicultural contacts and communication are oftencomplicated by language barriers, and obstructionsare caused by different culturally defined views andperceptions.1 Consequently, the physician–patientrelationship may also be affected.2–4 According toKleinman, both physician and patient need toexchange each other’s perceptions about thepatient’s illness (their ‘explanatory models’) in orderto achieve understanding and agreement aboutdiagnosis and treatment.5 Lack of understandingand agreement is assumed to lead to lesscompliance and a reduction in perceived quality ofcare.1-2 Kleinman also argued that ‘uncovering andsolving discrepancies in explanatory models’between physician and patient is determined bymutual understanding between them, as well as bygeneral feelings, such as patient satisfaction and thepatient’s feeling that the physician has beenH Harmsen, PhD, MD, GP researcher, Department of HealthPolicy and Management; Department of General Practice;R Bernsen, MSc, research statistician; S Thomas, PhD, MD,professor and head of department, Department of GeneralPractice; MA Bruijnzeels, PhD, associate professor, Departmentof Health Policy and Management, Erasmus MC, UniversityMedical Centre Rotterdam, Rotterdam. L Meeuwesen, PhD,associate professor, Interdisciplinary Social Science Department,Research Institute for Psychology and Health, UtrechtUniversity, Utrecht. G Dorrenboom, MD, retired GP. D Pinto,PhD, professor of intercultural communication, Social andBehavioural Sciences, University of Amsterdam, Amsterdam.Address for correspondenceJAM (Hans) Harmsen, Department of Health Policy andManagement, Erasmus MC, University Medical CentreRotterdam, P.O. Box 1738, 3000DR Rotterdam,The Netherlands. E-mail: j.harmsen@erasmusmc.nlSubmitted: 9 August 2004; Editor’s response: 29 October2004; final acceptance: 7 January 2005. British Journal of General Practice 2005; 55: 343–350.British Journal of General Practice, May 2005343
H Harmsen, R Bernsen, L Meeuwesen, et alHow this fits inCultural differences between GPs and patients increase the chance ofmiscomprehension and can lead to patient non-compliance with treatment. Adouble educational intervention given to both physician and patient aimed toimprove their intercultural communication, reduce their mutualmisunderstanding and improve patients’ perception of the quality of care. Thisintervention effect occurs only 6 months after GP training and is probably dueto the slow changing of attitudes and communication style. The effect is thestrongest in consultations with non-Western patients, who live between thetraditional culture of their country of origin and Western culture. This is also thegroup of patients with the greatest improvement in comprehension with theirphysician.considerate.6–9 Misunderstanding and patientdissatisfaction tended to increase when the culturalgap between physician and patient was wider.6,10,11By improving communication during theconsultation ‘discrepancy in explanatory models’can be reduced in order to achieve better mutualunderstanding and consequently better perceivedcare and patient compliance; this improvement canbe achieved by instruction and training incommunication of both physician and patient.12–13The aim of this study is to assess the effect of ion given to both GPs and patients (bothWestern and non-Western countries of origin) onmutual understanding and perceived quality of care.The intervention aims to reduce differences inmutual understanding and perceived quality of carein consultations with patients of different nativeorigins and its effect was assessed using arandomised controlled trial. We hypothesise that ion, given to both GP and patient, coulddecrease inequalities in care between Western andnon-Western patients.population of at least 25% of patients with a nonWestern country of origin were invited to participateby letter and by one repeat request by telephone.Inclusion criteria for the patients were a visit to theirGP for a consultation on random days in February,May and November 2000 (in which months eachgeneral practice was visited once for measurement).We excluded adolescents aged 13–17 years becauseof expected problems in an interview due to thenature of the questions. A parent of the children agedup to 12 years was interviewed.To estimate the sample size we considered ourmain outcome parameter, mutual understanding, asa dichotomous variable. Assuming a power of 80%,a significance level of 5%, a fraction of 0.5 mutualunderstanding in the control group, an absolutetreatment effect of 0.2, taking the multilevel designinto account and assuming an intracluster correlationof 0.2 and 20 patients per physician, 748 patients(corresponding with 38 physicians) are required foreach measurement.14InterventionBoth GPs and patients received intervention with on between them.Patient interventionThis consisted of a 12-minute videotaped instructionin the waiting room for all patients immediately beforethe consultation; the videos were available in Dutchand the languages of the major ethnic minority groups(Moroccan–Arabic, Moroccan–Berber, Turkish). Themain message was to instruct patients tocommunicate directly and to express freely anymisunderstanding and disagreement. Two examples(one with unsatisfactory and indirect communicationand one with satisfactory and direct communicationof the patient) were used to illustrate the mainmessage of the videotape.METHOD344ParticipantsGP interventionGPs were randomised to an intervention or a controlgroup and the effects of the study were analysed atthe patient level. Measurements took place atbaseline (first measurement), and within 1 month(second measurement) and at 6 months (thirdmeasurement) after the GP intervention. At the threemeasurement times the same GP was involved,whereas the patients differed all the time. Blindingthe GPs for the intervention was impossible as itinvolved training. Interviewers, experts and researchassistants, who conducted preliminary dataprocessing, were blinded for interventionassignment. Patients were ignorant about the groupassignment of their GP. GPs with a practiceThis consisted of 2.5 days of training on interculturalcommunication for the GPs, based on Pinto’s ‘threestep method’.15 First, the GPs were allowed to reflecton their own culturally-defined norms, views andcommunication style. Second, we aimed to improvesensitivity and knowledge about culturallydetermined differences in views and behaviour(including communication style), mainly in patientsoriginating from non-Western countries, and, third, totrain the GPs in (self-chosen) strategies to solve thegaps in views and culturally-defined communicationstyle. Two weeks later (in a final training session) anyproblems experienced were discussed andsupplementary advice was given.British Journal of General Practice, May 2005
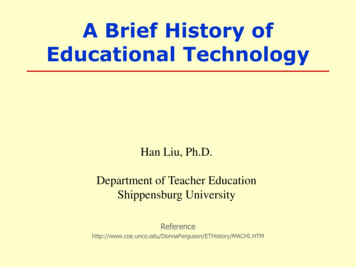
Original Papers38 GPs in Rotterdam agreed to participateIntervention group 19 GPsControl group 19 GPsPlanned measurements (1–2 days at each practice for 10–20consultations) on arbitrarily selected days within measurement period(4–6 weeks/each measurement)aBaseline or first measurementa(February 2000, 19 GPs)355 patients invited 1(44% non-Western)237 patients agreed (37% non-Western)175 completed interview/GP questionnaire (33% non-Western)Baseline or first measurementa(February 2000, 19 GPs)362 patients invited 1(42% non-Western)270 patients agreed (42% non-Western)176 completed interview/GP questionnaire (35% non-Western)Interventional postgraduatetraining of GPs (April 2000)Video instruction for patientsbefore consultationSecond measurementa (May 2000, 18 GPs)395 patients invited (46% non-Western)247 patients agreed 1(46% non-Western)161 completed interview/GP questionnaire (40% non-Western)Second measurementa (May 2000, 19 GPs)453 patients invited (52% non-Western)273 patients agreed 1(53% non-Western)172 completed interview/GP questionnaire (48% non-Western)Video instruction for patientsbefore consultationThird measurementa (November 2000, 17 GPs)395 patients invited (35% non-Western)207 patients agreed 1(35% non-Western)151 completed interview/GP questionnaire (31% non-Western)Third measurementa (November 2000, 18 GPs)447 patients invited (44% non-Western)244 patients agreed 1(44% non-Western)151 completed interview/GP questionnaire (41% non-Western)aAt each measurement the GP remained the same whereas patients were different. All patients (regardless of their ethnic origin) visiting the GP on measurementdays were asked to participate until at least 10 and at most 20 consultations were included per measurement for each GP. Consequently, each measurement took1-2 days for each practice. Because the patients were visited at home for an interview after the consultation there was a second level of non-response. The studygroup consisted only of the consultations for which a match with data from the patient’s home interview and the GP questionnaire could be made.MeasuresData were collected by means of a GP questionnairecompleted immediately after the consultation, and bymeans of patient interviews at home 3–8 days afterthe consultation. The GP questionnaire and thepatient’s home interview contained similar questionson the presenting health complaint, their own and theother’s ideas about the cause of the health complaintand diagnosis, and on the proposed treatment ormedical investigations.To assess our primary outcome, mutualunderstanding between GP and patient, answersfrom the GP and patient about different aspects ofthe consultation were compared and scaled on avalidated scale.16 The response could range from-1 (total misunderstanding) to 1 (complete mutualunderstanding).British Journal of General Practice, May 2005Secondary outcomes were the patient’ssatisfaction with the consultation and the patient’sfeeling that the physician had been considerate.Both these items were explored in the homeinterview with three answering categories(yes/doubtful/no) and answers were dichotomised(‘yes’ versus ‘doubtful’ and ‘no’). A further outcomewas quality of care and was measured by thevalidated questions of Quote-Mi (quality of carethrough patient’s eyes) (JAM Harmsen, et al,unpublished data 2004).17 Response to the QuoteMi ranged from 1 (perceived poor quality) to 10(perceived good quality).Country of origin was based on own and parentalcountry of birth: responders were divided into a‘Western’ (mostly Dutch but also some patients fromother West European, North American, Canadian andFigure 1. Flowchart of thelevels of response of thepatient population.345
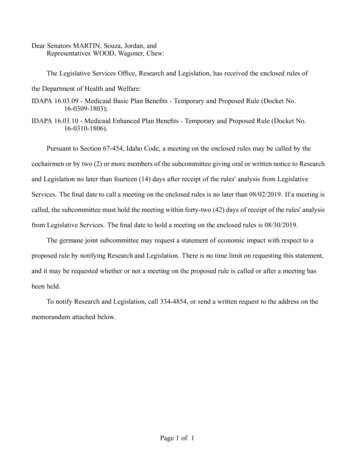
H Harmsen, R Bernsen, L Meeuwesen, et alTable 1. Patient characteristics.aTotal study groupn 986%Western patientsn 614%Non-Western patientsn 369%Age in 6618.0 6517017.416126.492.5Monthly net income ( ) .53813.21588–1951577.7419.0165.6 1951283.8214.672.4EducationPrimary school not completed464.7193.2278.0Primary school completed28528.917529.311032.5Lower professionalcand secondary education20922.314424.16519.2Medium professionalc andsecondary education13414.38514.24914.5Higher secondary education525.5254.2267.7Higher professional educationand 5Poor or speaks no male61562.838863.522461.2Self-perceived proficiency in DutchSexMissing data (not registered or refusal of information by patients): ethnicity (Western versus non-Western) n 3, age n 8,income n 243, education n 47 language proficiency n 63, sex n 6. bThe age band 13–17 years was not studied. cLower/higher professional education (technical education and vocational education) and lower/higher secondary education.aAustralian origin) and a ‘non-Western group’ (mainlyTurkish, Moroccan, Cape Verdean and Surinamesepatients).18Cultural background was assessed through thepatient’s score on the validated patient culturalbackground scale: on the basis of culturally definednorms and values patients were divided in modern,traditional and in-between (partly traditional/modern)group.19AnalysisThe effect on mutual understanding and perceivedquality of care was analysed using multilevelmultiple regression techniques adjusted forbaseline values. Analyses were performed for all346patients together and, because the focus of theintervention was on intercultural communication,sub-analyses were made for Western and nonWestern patients and for patients with ditional/modern and modern).‘Satisfaction’ and ‘feeling that the GP had beenconsiderate’ was analysed at the physician level andthe fraction of satisfied patients was calculated perphysician and per measurement. Differencesbetween the two patient groups were tested bymeans of regression analysis with adjustment forbaseline fraction, weighing cases (physicians) withthe total number of patients seen at baseline plus atthe measurement concerned.British Journal of General Practice, May 2005
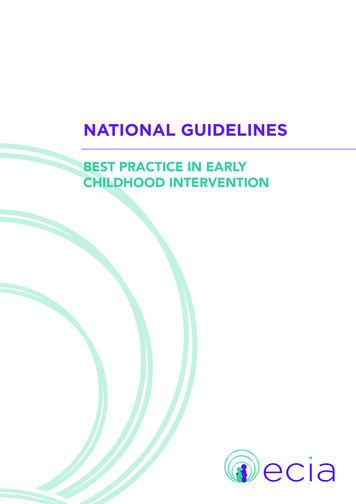
Original PapersTable 2. Results of outcome measures at baseline and after intervention.BaselineImmediately afterGP intervention(Change from baseline)InterventionControl6 months afterGP intervention(Change from baseline)ICInterventionControlMean mutual understanding (range 0.144(0.01)Mean patient’s perception of quality of care (range 0.14)Patient’s satisfaction with the consultation (% yes)848683(-1)85(-1)87(3)82(-4)Patient’s feeling that consideration was shown (% yes)838188(5)88(7)88(5)86(5)Mean mutual understanding (range -1–1)0.1450.1590.149 (0.004) 0.186(0.03)0.177(0.03)0.238(0.08)Mean patient’s perception of quality of care (range 0.24)Patient’s satisfaction with the consultation (% yes)928685(-7)88(2)86(-6)85(-1)Patient’s feeling that consideration was shown (% yes)908592(2)91(6)91(1)91(-1)All patientsWestern patientsNon-Western patientsMean mutual understanding (range -1–1)-0.074 0.0850.028(0.10)0.097(0.01)0.127(0.20) -0.060 -0.15)Patient’s satisfaction with the consultation (% yes)708680(10)78(-8)88(18)77(-9)Patient’s feeling that consideration was shown (% yes)697483(14)83(9)84(15)77(3)Mean patient’s perception of quality of care (range 1–10)I intervention group. C control group.RESULTSParticipantsOne hundred and seventy GPs received a letter ofinvitation and 13 of these spontaneously enrolled.The remaining GPs were subsequently invited bytelephone to participate. This telephone recruitmentwas stopped after calling 120 GPs as the maximumnumber of 38 GPs had been reached. In theintervention group all 19 GPs participated in thethree measurements. In the control group one GPdropped out during the second measurement dueto illness, and another in the third measurement dueto cessation of the medical practice. All GPs (eightof whom were female) had worked for more than5 years in their current practice setting. Two GPshad a non-Dutch (but Western) ethnic backgroundand had lived and worked for more than 20 years inthe Netherlands. Figure 1 is a flow diagram of datacollection and the responses during the threemeasurement periods, according to the CONSORTstatement.20 The total net response of patients was40% in the intervention group and 43% in thecontrolgroup.Mutualunderstandinginconsultations with non-Western patients waspoorer than with Western patients, which wassimilar to our earlier findings.21Patients with a non-Western country of originrefused more often to participate in the study (56%British Journal of General Practice, May 2005and 44% of the total number of refusals,respectively). At the home interview non-Westernpatients dropped out more often than Westernpatients did (55% and 45% of the total number offailed home interviews, respectively). Reasons fornon-response at the home interview for nonWestern and Western patients were that thepatients were not at home (43% and 42.5%,respectively), refusal to make an appointment (14%and 15%, respectively), absence of a suitableinterviewer (22% and 19%, respectively) and otherreasons or unknown (21% and 24%, respectively).Both research groups did not essentially diverge intheir pattern of non-response (Table 1; Figure 1).The study group consisted of 986 consultations forwhich a match could be made between patient andGP data.Effect of the interventionThe scores on all outcome measures in eachmeasurement are shown in Table 2.There are some differences at baseline betweenthe intervention and control groups, but in generalnon-Western patients scored less affirmatively thanWestern patients did.For the total patient population at 1 and 6 monthsafter the intervention no differences were foundbetween the intervention and control group in347
H Harmsen, R Bernsen, L Meeuwesen, et alTable 3. Intervention effect on primary and secondary outcomes with multilevel regression techniques1 month and after 6 months after intervention.1 month6 monthsDifference between interventionand control group adjusted for baselinemeasured direct after the GP interventionDifference between interventionand control group adjusted forbaseline measured 6 monthsafter the GP intervention.Effect size(% of rangea)ß95% CIEffect size(% of rangea)ß95% CIAll patientsMutual understanding 3.00-0.06 -0.171 to 0.043 0.500.01 -0.103 to 0.129Patient’s perception of quality of care 3.00-0.31 -0.742 to 0.127 0.200.02 -0.437 to 0.469Patient’s satisfaction with the consultationa,b 0.03-0.124 to 0.068 0.03-0.060 to 0.122Patient’s feeling that consideration was showna,b 0.01-0.107 to 0.096 0.01-0.092 to 0.071Mutual understanding 2.00-0.04 -0.168 to 0.095 3.00-0.06 -0.201 to 0.079Patient’s perception of quality of care 2.00-0.22 -0.721 to 0.275 2.50-0.25 -0.759 to 0.259Patient’s satisfaction with the consultationa,b 0.06-0.191 to 0.079 0.02-0.088 to 0.132Patient’s feeling that consideration was showna,b 0.08-0.214 to 0.059 0.02-0.088 to 0.135Mutual understanding 4.00-0.08 -0.246 to 0.082 11.000.21Patient’s perception of quality of care 4.000.40 -1.120 to 0.312 7.000.74 -0.005 to 1.494Patient’s satisfaction with the consultationa,b 0.03-0.131 to 0.190 0.14-0.031 to 0.305Patient’s feeling that consideration was showna,b 0.03-0.218 to 0.151 0.12-0.043 to 0.287Western patientsNon-Western patients0.002 to 0.422Size of the effect: decreased % of range / increased % of range of measure. bWe computed per physician and per measurement the fraction of patients thatwere satisfied with (‘felt GP had been considerate’ during) the consultation. The difference between the two groups was tested by means of regression analysiswith adjustment for baseline fraction, weighing cases (physicians) with the total number of patients seen at baseline plus at the measurement concerned.aprimary and secondary outcomes, or for the Westernpatients alone (Table 3). For the non-Westernpatients, 6 months after the intervention there was an11% improvement (95% confidence interval [CI] 0.002 to 0.422) in mutual understanding and a 7%improvement (95% CI -0.005 to 1.494) in theperceived quality of care; satisfaction and the feelingthat the GP had been considerate also showed aneffect in the desired direction. More detailed study ofthe patient’s cultural background in the non-Westerngroup showed that the partly traditional/moderngroup accounted for most of the effect on mutualunderstanding after 6 months (19% improvement,95% CI 0.027 to 0.535).DISCUSSIONSummary of main findingsOur intervention on intercultural communication forboth GPs and patients was effective in the nonWestern patient group, which supports our aim ofdecreasing differences in outcomes of care betweenWestern and non-Western patients. Both mutualunderstanding and perceived quality of care348improved. The effect was almost completelyexplained by improvement within the group of thepartly traditional/modern patients. We observed noeffect when considering the total study population orin the Western patients alone. Despite a change inthe perceived quality of care, more generic measuressuch as ‘feeling that the GP had been considerate’and ‘consultation satisfaction’ did not changesignificantly, although there was a change in desireddirection. A speculative explanation for this result isthat for generic measures more time is needed.22 Wecan only hypothesise why the effect was minimalwithin 1 month after the intervention and becamemore apparent after 6 months. It may be thatchanging one’s personal approach, attitude andcommunication style in a very short time is difficult. Itis unknown whether one intervention is sufficient toachieve consistent changes. In advertising, forexample, the phenomenon of the repeatedly givenmessage is widely employed and therefore retrainingof physicians and instruction of patients needs to begiven continuously. In our opinion, these results mayprovide an argument for more culturally centredBritish Journal of General Practice, May 2005
Original Paperscommunication training in the education of medicalstudents and vocational training of GPs.Comparison with existing literatureThe observed effect after 6 months is not quite in linewith Kleinman’s theory: that the larger the culturaldistance between physician and patient the greaterthe misunderstanding.5 Detailed analysis of our studyand results from an earlier study showed that partlytraditional/modern patients had the mostmisunderstanding with their physician.21 Thus, for thetraditional group other mechanisms such assatisfaction and the ‘feeling that the physician wasconsiderate’ may be more important for mutualunderstanding. The success of physician’s retrainingis often regarded as minimal23,24 and little is knownabout providing videotaped instruction to patients,especially non-Western patients.25 Therefore, it isnoteworthy that an effect was demonstrated in thetargeted group of non-Western patients; theseresults also support those who claim a positive effectof retraining for physicians.26,27We chose a double intervention, for both patientsand physicians, because both parties are responsiblefor adequate communication in medical encountersand this approach conforms with Pinto’s three-stepmethod and Kleinman’s theory of exchangingexplanatory models.5,15Strength and limitations of the studyThere was a considerably high rate of non-responsefrom GPs and a high refusal rate for non-Westernpatients. Participating GPs were highly motivatedand therefore the results cannot be generalised. Onthe other hand, it should be considered thatcommitment with the subject matter is alwaysnecessary for effective learning. The positiveintervention effect showed that improvement ispossible even though awareness and commitmentshould be raised first. The differences in responsefrom Western and non-Western patients (in both theintervention and control groups) may havenegatively influenced the results due to loss ofstatistical power; the focus of our intervention wason patients with a more traditional culturalbackground and we could not include the plannednumber of patients. On the other hand, because thedata were analysed with mutual understanding ascontinuous variables, the estimates in the powercalculation were conservative (an overestimate ofthe number of patients needed).Implications for research and clinical practiceA double intervention on intercultural communicationshowed improvement of mutual understandingbetween physicians and non-Western patients andBritish Journal of General Practice, May 2005decreased differences in outcomes of care. Thisfinding should encourage greater efforts regardingthe teaching of intercultural communication formedical students and physicians. The interventionwould be most effective for physicians working withnon-Western patients who recognise communicationproblems due to different cultural backgrounds andare willing to improve their interculturalcommunication. Students should also be taught thatthe patient’s cultural background is a substantial partof their context. They should reflect and be aware oftheir own cultural norms and values and learn moreabout different culturally defined opinions and views.Patients also should be invited to communicate in away that is expected by and helpful to the physician.This study proves that cultural differences play animportant role in medical consultations, but certainlythese are not unbridgeable. More research,especially trials aiming to bridge the cultural gapbetween physician and patient, should be performedin order to reduce differences in quality of carebetween Western and non-Western patients.Funding bodyTheia Foundation of Zilverenkruis Achmea (JvH/agbrf640),ZonMW: Netherlands Organisation for Health Research andDevelopment. Fonds Aachterstandswijken, DistrictsHuisartsen Vereniging Rotterdam (Besluit FAW:98/09/H-O),Stichting Bevordering van Volkskrach (MK/avg/000–001).Ethics committeeUniversity Ethical Commission of the Erasmus MedicalCentre, University Medical Centre in Rotterdam (MEC163.267/1997/122)Competing interestsNoneAcknowledgementsThe authors wish to thank all patients and GPs for theircooperation in this study.REFERENCES1. Penn NE, Kar S, Kramer J, et al. Ethnic minorities, health caresystems, and behavior. Health Psychol 1995; 14(7): 641–646.2. Brown CM, Segal R. The effects of health and treatmentperceptions on the use of prescribed medication and homeremedies among African American and white Americanhypertensives. Soc Sci Med 1996; 43(6): 903–917.3. Patel S. Intercultural consultations. Language is not the onlybarrier [letter; comment]. BMJ 1995; 310: 194.4. Stone MA, Patel H, Panja KK, et al. Reasons for non-compliancewith screening for infection with Helicobacter pylori, in a multiethnic community in Leicester, UK. Public Health 1998; 112(3):153–156.5. Kleinman MA. Patients and healers in the context of culture.London: University of California Press; 1980.6. Van Wieringen JC, Harmsen JA, Bruijnzeels MA. Interculturalcommunication in general practice. Eur J Public Health 2002;12(1): 63–68.7. Williams SJ, Calnan M. Key determinants of consumer satisfactionwith general practice. Fam Pract 1991; 8(3): 237–242.8. Naish J, Brown J, Denton B. Intercultural consultations:investigation of factors that deter non-English speaking womenfrom attending their general practitioners for cervical screening.BMJ 1994; 309(6962): 1126–1128.9. Kleinman A. Clinical relevance of anthropological and crosscultural research: concepts and strategies. Am J Psychiatry 1978;135(4): 427–431.349
H Harmsen, R Bernsen, L Meeuwesen, et al10. Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, andpartnership in the patient-physician relationship. JAMA 1999;282(6): 583–589.11. Laveist TA, Nuru-Jeter A. Is doctor-patient race concordanceassociated with greater satisfaction with care? J Health Soc Behav2002; 43(3): 296–306.12. Rosenberg EE, Lussier MT, Beaudoin C. Lessons for clinicians fromphysician-patient communication literature. Arch Fam Med 1997;6(3): 279–283.13. Cegala DJ, Marinelli T, Post D. The effects of patientcommunication skills training on compliance. Arch Fam Med 2000;9(1): 57–64.14. Underwood M, Barnett A, Hajioff S. Cluster randomisation: a trapfor the unwary. Br J Gen Pract 1998; 48(428): 1089–1090.15. Pinto D. Intercultural communication. A three-step method fordealing with differences. Leuven: Garant; 2000.16. Harmsen JAM, Bernsen RMD, M
PhD, professor of intercultural communication, Social and Behavioural Sciences, University of Amsterdam, Amsterdam. Address for correspondence JAM (Hans) Harmsen, Department of Health Policy and Management, Erasmus MC, University Medical Centre Rotterdam, P.O. Box 1738, 3000DR Rotterdam,