Transcription
DIRECTIVES OF BOARD OF DIRECTORSCORPORATE OFFICERS President - Eduardo Martínez Tull Executive Director - Allan Cintrón Salichs, MBA, MHCM. Vice-President – Gladys Santos Medical Director - Awilda García Rodríguez, MD Secretary – María Roque Finance Director - Francisco Bayanilla, MBA Treasurer – Victor Montalvo1
2
A NOT-FOR-PROFITCOMMUNITY BASEDHEALTHCARE SERVICESCORPORATION3
Founded in 1971 as “Consejo de Salud de laComunidad de la Playa de Ponce, Inc.”, thecorporate name was changed in November 18,2009, to “Consejo de Salud de Puerto Rico, Inc.”and the brand of “Med Centro ” was registered asa trade mark.This institution is qualified by CMS as a FederallyQualified Health Center (FQHC) under Section 330of the Public Health Service Act (42 USCS § 254b).4
SITE MAP LOCATIONS5
HRSA APPROVED SITES FOR MED CENTROFixed Sites6Mobile Unit Sites4Total Sites106
7
8
9
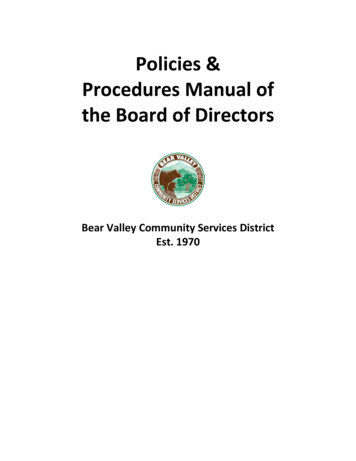
POPULATION IN AREAS OF SERVICE200,000180,312N ,94760,00029,28430,05440,00020,000-PonceJuana DíazPeñuelasVillalba (NAP)10
NUMBER OF PATIENTS SERVED11
UDS 2014PRIMARY CARE PATIENTSCHARACTERISTIC0 TO 17YEARS OLD18 YEARSAND OLDERTOTALNone/Uninsured3,3194,0577,376Regular Medicaid (Title 327,09440,337MedicarePrivate InsuranceTOTALTOTAL CLINICAL VISITSAVERAGE VISIT PER PATIENT179,2314.44Numbers from HRSA, UDS Reports12
RYAN WHITE PART CTotal Number of PatientsFY-2013246FY-2014254NETCHANGE8Numbers from HRSA/HAB, RSR13
RANKING ACCORDING TOFEDERAL AWARDS14
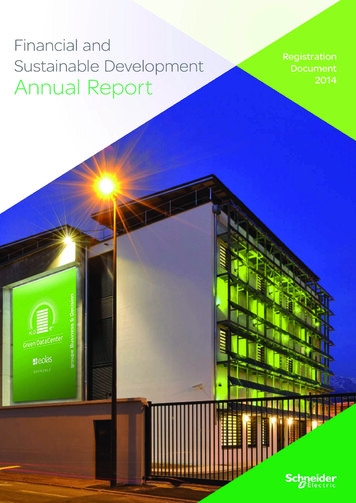
FY 2015330 Health Centers Ranking Position According to Federal Grant AwardTotal Awardees 1,381Total Awards CaliforniaCLINICA SIERRA VISTA 18,566,3030.5072%2WashingtonYAKIMA VALLEY FARM WORKERS CLINIC 14,602,7280.3989%3New YorkSUNSET PARK HEALTH COUNCIL, INC. 14,564,6430.3978%4New YorkHUDSON RIVER HEALTHCARE, INC. 13,886,1120.3793%5CaliforniaFAMILY HEALTH CENTERS OF SAN DIEGO, INC. 13,634,8680.3725%6AlabamaQUALITY OF LIFE HEALTH SERVICES INC 13,340,8130.3644%7IllinoisSOUTHERN ILLINOIS HEALTH CARE FOUNDATION, INC. 13,215,1050.3610%8ColoradoDENVER HEALTH AND HOSPITALS AUTHORITY 13,162,6200.3596%9ColoradoPLAN DE SALUD DEL VALLE, INC. 12,579,4160.3436%10CaliforniaCOMMUNITY HEALTH CENTERS OF THE CENTRAL COAST, INC. 12,195,2850.3331%11IllinoisACCESS COMMUNITY HEALTH NETWORK 12,062,5370.3295%12CaliforniaNORTHEAST VALLEY HEALTH CORPORATION 12,045,0640.3290%13FloridaCOMMUNITY HEALTH SOUTH FLORIDA, INC. 11,779,2920.3218%14WashingtonSEA-MAR COMMUNITY HEALTH CENTER 11,572,4650.3161%15CaliforniaGOLDEN VALLEY HEALTH CENTERS 11,559,1450.3158%16CaliforniaFAMILY HEALTHCARE NETWORK 11,203,3790.3060%17AlabamaFRANKLIN PRIMARY HEALTH CENTER, INC. 11,082,8190.3027%18OhioNORTHEAST OHIO NEIGHBORHOOD HEALTH SERVICES, INC. 10,756,8830.2938%19IllinoisAUNT MARTHA'S YOUTH SERVICE CENTER, INC. 10,664,1970.2913%20Puerto RicoCONSEJO DE SALUD DE PUERTO RICO, INC. 10,206,4160.2788%CSPR ranks # 20 among 1,381 HRSA 330 grantees across the nation15
FY 2015330 Health Centers Ranking Position According to Federal Grant AwardTotal Awardees 1,381Total Awards 3,660,849,11216
17
18
19
20
21
RECRUITMENT AND RETENTION CRITICAL AREA: PhysiciansEXTERNAL PROBLEM: Throughout years 2012 to 2015 Puerto Rico’s economical crisis hasprovoked in the Island a massive immigration of physicians tomainland states. This is expected to worsen throughout coming years.Thus, this has become an external threat to all healthcareorganizations in the Island.INTERNAL PROBLEM: Throughout 2012, 2013 and 2014, Med Centro lost physicians at anaverage rate of 12 per year. In 2015 physician turnover rate was reduced to 6 in a year and withshorter recruitment intervals.22
PROBLEM CONTRIBUTORS Salaries offered at states in mainland double those offered in PR.A drag is produced by physicians who move to states in mainland andcall their colleagues in the Island to follow their successful stepsabroad.Economic incentives offered by local HMO’s promote physiciansmovement to independent practices. However, it is our opinion thatsome of these incentives encourage practices that are highlyquestionable regarding quality of care and non compliances withstandards of care.Cost of living has significantly increased in PRRules of economy: DECREASE IN SUPPLY INCREASE IN DEMAND INCREASE IN COSTThus, physician recruitment and retention is now more that everbefore vulnerable to the offerings of a local competitive marketplace.Economic restrains under which Health Centers must operate reducesthe ability to be competitive.23
OPPORTUNITIES Physicians with social and other local attachments are looking forfinancially stable organizations where they can shelter Wraparound payments to FQHCs provide institutional financialleverage as to be able to offer economically competitivecompensation packages to physicians Physicians benefit of free Medical Malpractice Immunity under theFederal Tort Claims Act (FTCA), for acts or omissions in theperformance of medical, surgical, dental, or related functions resultingin personal injury, including death, and occurring within the scope ofemployment at qualified Federally Qualified Health Center (FQHC) National Health Services Corps Loan Repayment Program forqualifying physicians who still owe education loans.24
Licensed health care providers may earn up to 50,000 toward studentloans in exchange for a two-year commitment at an NHSC-approved sitethrough the NHSC Loan Repayment Program (NHSC LRP). Qualifyingapplications must be from providers working at or have an accepted offerof employment at an NHSC-approved service site. Facts: Application period: Window normally opens from February throughout Augusteach yearProvider Specialties: Family Medicine; Gynecologists; Internal Medicine;Psychiatrists; Psychologists; Geriatrics; Critical Care Nurse; Dental PrimaryCare; Pediatricians (NOTE: Other non-provider specialties qualify)Time and effort required: Part-time (20 hours) / Full time (40 hours)Benefit: Incentive amount for practitioner is up to 25,000 (tax free) per yeartoward loan repayment. There are no costs for the institutionDuration: Up to 2 years and normally renewable for an extension of 2 moreyears for a total of 4 years25
MED CENTRO STRATEGIES Merit Based Incentive Program through which commitment andperformance are financially acknowledged with awards of up to 30,000 above the base salary in the year (number for FY 2015). Recruitment Bond of 10,000 (upfront and above base salary) fornewly contracted provider. Retention Bond of 5,000 (upfront and above base salary) for providercontract renewal . High commitment with an enhanced work environment and the socialacknowledgment of the Med Centro brand Sustained reputation of a financially stable organization and itscommitment to high quality care26
Merit Based Incentive Program is a financial award that isavailable only for Clinical Faculty Providers who areemployees of Med CentroUsing a metric based methodology on Qualifying Indicatorsand Merit Indicators providers who qualify for the incentiveare acknowledged for their commitment and performance.This program was created by Med Centro in 2013 as astrategy to improve recruitment and retention of clinicalproviders.27
Qualifying Indicators are those which the provider mustcompletely meet before being considered for any incentive.Not meeting all of these completely disqualifies a providerfrom receiving an incentive. There are 6 Qualifying IndicatorsMerit Indicators provides the metric to determine theprovider’s amount of share of the total amount allocated bythe Board of Directors in the Institutional Budget for theFinancial Incentive in a year. There are 12 Merit IndicatorsIn year 2015 the BOD approved a budget allocation for theMerit Based Incentive in the amount of 1,000,000, plusmandatory taxes.28
(1-A) NO SEVERE DISCIPLINARY ACTIONS FILED –Refers to disciplinary actions executed by the HumanResources Department against the employee in the yearbeing considered for the ATION – Complaint refers to complaints of seriousmisconduct by the provider. Affirmative means that there is aformal complaint against the provider.29
(3-A) IN COMPLIANCE WITH PATIENT QUOTA – Eachprovider must reach a minimum number of face to faceencounters with patients during the fiscal year.(4-A) ACTIVE EMPLOYEE THAT IS A FACULTY MEMBERFOR THE LAST FULL FISCAL YEAR – Refers to a providerthat holds an employee status and that has uninterruptedlyworked either as a full-time or part-time provider for lastconsecutive fiscal year in CSPR.30
(5-A) EVALUATION SCORE OVER 70% - Participatingproviders must attain a score of at least 70% in the prior orcurrent year’s Performance Evaluation (the latest apply)(6-A) PROVIDER IS NOT UNDER RESTRICTIVECONTRACT AGREEMENT – A provider under a contractagreement that specifically excludes the participation in anyor specifically in a retention merit incentive will not be incompliance with this indicator31
(1-B) PROFESSIONAL RANK – Merit value points areawarded according to a scale in correlation with theprofessional ranking of the provider (e.g.: general medicine;specialized medicine; subspecialized medicine; dentist; psychologist)(2-B) ANNUAL EVALUATION – Merit value points areawarded according to a scale that measures the percentageof compliance attained in the year evaluation.32
(3-B) ATTENDANCE COMMITMENT – Attendance andpunctuality commitment is acknowledged with merit valuepoints according to a scale that determines the level ofcompliance(4-B) CREDENTIALING COMPLIANCE – Credentialing andauthorizing privileges to professional providers stands at thehighest legal and financial risk factors in healthcare. Total,diligent and timely compliance of providers with theInstitution’s credentialing requirements is acknowledged witha fixed amount of value points. This indicator is measured interms of full compliance only (Met or Not met)33
(5-B) PRESIDENCY OF INSTITUTIONAL COMMITTEE ORDEPARTMENT DIRECTOR – Professional providers thatpreside an Institutional Committees or are Director of aDepartment are acknowledgment for their contribution to theoverall wellness of the Institution. Provider must demonstratethat their role was consistently executed to receive a fixedamount of value points. This indicator is measured in termsof full compliance only (Met or Not met)34
(6-B) EXTRAORDINARY ACHIEVEMENT – An extraordinaryachievement is an action or an endeavor carried out by theprovider, outside the routine of his duties, and that producesan added value to the Institution. Merit value points arediscretionary awarded, according to a scale, by the firstexecutive of the organization.35
(7-B) QUALITY COMPLIANCE – Quality stands atop of allpriorities in the organization. Merit value points are awardedaccording to a scale to those practitioners that demonstrateto be in measurable high compliance with the expectationsof the clinical indicators according to the reports of theDepartment of Continuous Quality Improvement / QualityAssurance.36
(8-B) ADMINISTRATIVE COMPLIANCE – Administrativecompliance is directly correlated with a cost effectiveoperation. The thin financial margins as well as the denseregulatory environment to which healthcare organizationsare subject to require a high level of diligent compliance inall administrative issues. Some of these issues are directlyinherent to the endeavors carried out by the provider. Meritvalue points are awarded according to a scale to thosepractitioners that demonstrate to be in high compliance withtheir inherent administrative responsibilities (e.g.: Coding;Patient Check-Out closing)37
(9-B) SICK LEAVE ALLOWANCE – The amount of workdays the provider is available to serve patients during theyear and the continuum of programed availability of servicesfor patients with appointments or walk-ins are factors thatcontribute to the overall expected efficiency of CSPR. Sickleave allowance merit value points are awarded according toa scale38
(10-B) CMS EHR INCENTIVE DESIGNATION IN FAVOR OFCSPR – The Medicare and Medicaid Electronic HealthRecords (EHR) Incentive Program will provide incentivepayments to eligible professionals and eligible hospitals asthey demonstrate adoption, implementation, upgrading ormeaningful use of certifier EHR technology. As providers arede facto employees of Institution who owns and operates theEHR, these may elect to designate CSPR to receive theincentive funds on their behalf. Providers that file anattestation in favor of the institution are awarded a fixedamount of value points. This indicator is measured in termsof full compliance only (Met or Not met)39
(11-B) PRODUCTIVITY – Productivity will be measured byaccounting the number of face to face encounters a providerperforms in a given year. While a productivity quota is aqualifying criterion for receiving any Retention MeritFinancial Incentive, some providers are able to exceed theirquota thus denoting an extra effort and commitment with thehealthcare service they render. The merits of suchproductive endeavor is acknowledged with merit value pointsaccording to a scale40
(12-B) PLEDGED FOR FORTHCOMING YEAR – Retentionof good professional providers is important for Consejo deSalud de Puerto Rico. Accordingly the institution providesthese professionals the option of subscribing a pledge forcontinuing their contractual agreement with CSPRthroughout the fore coming year. In appreciation for thatcommitment the institution awards a fixed amount of valuepoints. This indicator is measured in terms of full complianceonly (Met or Not met)41
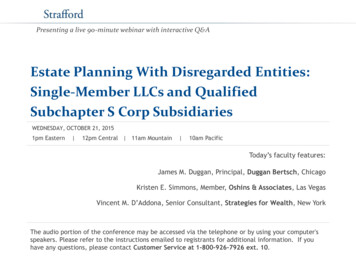
STATISTICSFY20152014AWARDSSTATITICSOFOF FYAWARDSTotal Qualifying Agregated PointsHighest 20,000Lowest 4,430Board Approved Retention 505,000Mean 17,791Total Awarded Cost of Incentives 462,574Mode 20,000Next Year Un-awarded Carryover 42,426Mediam 20,000Standard Deviation 9,342Total Qualified26Total Disqualified23Total Incomplete0Total "N"49422735.7
STATISTICSFY20152014AWARDSSTATITICSOFOF FYAWARDSTotal Qualifying Agregated PointsHighest 20,000Lowest 4,430Board Approved Retention 505,000Mean 17,791Total Awarded Cost of Incentives 462,574Mode 20,000Next Year Un-awarded Carryover 42,426Mediam 20,000Standard Deviation 9,342Total Qualified26Total Disqualified23Total Incomplete0Total "N"492735.7In year 2015 the BOD approved abudget allocation for the MeritBased Incentive in the amount of 1,000,000, plus mandatory taxes.Conversely the Capping (themaximum amount per provider) wasincreased from 20,000 to 30,00043
44
45
46
47
48
49
and a chance to meet great people!50
51
52
53
About La MaestraOur Mission: “To provide quality healthcare and education, improvethe overall well-being of the family, bringing the underserved,ethnically diverse communities into the mainstream of our society,through a caring, effective, culturally and linguistically competentmanner, respecting the dignity of all patients.”How we started: Clinic formed in 1990 under La Maestra AmnestyCenter. The need for culturally competent healthcare was identifiedby Student Council representing over 12,000 students whoparticipated in legalization programs, ESL, VESL, job training at LMAC.First Clinic, opened 1990LEED Certified Gold Health Center, opened 2010
Locations 4 Medical and 8 DentalSites in San Diego County,plus 4 school-based clinics City HeightsEl CajonNational CityLemon Grove El Cajon - AdditionalMedical & Dental siteopening soon Mental Health Servicesonsite & via telehealth Digital Imaging – Mammo,Xray, Ultrasound, Dexa, CT Mobile Clinic – medical,dental, optometry,telehealth NEW - Mobile Mammo
Serving the Culturally Diverse Communityo One of the most culturally diverse health centers in California – sitesare in refugee resettlement areas and along US-Mexican border.o 70% of patients prefer to communicate in a language other thanEnglisho Staff come from the cultures served, ensuring cultural and linguisticcompetency.o More than 28 languages and dialects spoken by 400 employeeso Medically Trained Cultural Liaisons provide valuable, ongoingsupport, education to local residents and identify new needs two-way communication
Innovative Models at La Maestrao La Maestra’s Circle of Care - All services and programs have elementsfocusing on education, case management, social services - IntegratedApproacho Medically Trained Cultural Liaison Modelo School-Based Clinics, Mobile Clinics, Hope Clinic, Telehealth:Alternative Access Points and Bringing Services to where residentsLive, Work, Learn, Play and Worshipo Electronic and Cloud-based Program/Case Managemento Specialty Care in the Medical Home via Telehealth and Partnershipso Digital Imagingo Contemporary Management Team Model
La Maestra’s Circle of Care
“Grassroots” Recruitment & Retentiono La Maestra was created and developed by community members whohad networks with ethnic and faith based organizations, schools, etc.Those networks have continued to grow over 25 years.Tips for Recruiting Culturally Competent Staff:o Contact ethnic based community organizations, faith basedorganizations to reach out and find staff to recruit from those diversepopulationso Also look for physicians from other countrieso Sponsor their vocational training to obtain required certificationo New staff from the populations served may work as promotoras andcultural liaisons, or admin support roles, while in healthcare training
“Grassroots” Recruitment & RetentionExamples:o A Vietnamese cultural liaison/outreach worker pursued Lab Techniciantraining, then attended university while working in lab now Director forall of LM’s laboratory sites.o A Sudanese refugee who started as a student, then worked as a jobcounselor and outreach worker, pursued Mental Health training and is nowan MFT at La Maestra (also has children graduating in healthcare field whoask to work at LM)o A Somali refugee records clerk working summers during high school, thenbecame a front desk receptionist while studying for a degree in nutrition.She is now a health educator, cultural liaison and pursuing Dietician license.o Many examples from other cultures and special populations, includingVeterans, Homeless, Older Adults, Survivors of Violent Crime includingTrafficking Victims, Cancer Survivors and those in Recovery from SubstanceAbuse.
Other Recruitment Resourceso Utilize local, state and national resources for recruitment, some arefree and some at a discount through associationso La Maestra Examples:o Local: Council of Community Clinics (consortia), YoungNonprofit Network, San Diego Workforce Partnership,Craigslist, Indeed.como State: CA Primary Care Association, Health Career Connections,State Loan Repayment Program, CA Health InterpretersAssociationo National: National Association for Community Health Centers,National Medical Fellowships, National Council of La Raza
Other Recruitment ResourcesHost Residents, Interns and Volunteers from:o Medical and Dental Schoolso Universitieso Vocational Trainingo Adult/Continuing Educationo High Schoolso Job Placement organizationsTips for Working with Volunteers, Interns and Pre-med students: Recruit from within these student pools for future employmentneeds While they are studying, offer flexible administrative andsupportive positions and recruit for special projects in the summer
Recruitment and Retention ChallengesCompetition in Recruiting and Retaining Staffo Large Hospital Systems offer better Salaryo But burnt out physicians, or those looking to help specialpopulations not frequent at hospital come to work at FQHCso Rural vs. Urban Salaryo Hospitals growing primary care arms to form their own ACOs andavoid including FQHCs - unintended consequence of reform
Retention Strategieso Increasing pay and benefitso Paying CME, license renewal feeso Offering or sponsoring training in other areas of specialtyo Positive feedbacko Reiterating their value to the community
an introduction to
to provide comprehensive,high-quality medical and dental care, patientadvocacy and related servicesto people who need them most,regardless of their ability to pay
ServicesMedical Care: Acrossthe lifespan For people living withHIV/AIDS HIV & STI testing Chronic care programming Women’s health services Podiatry Physical Therapy ImmunizationsBehavioral HealthCare:Mental Health Counseling Chemical DependencyCounseling Psychiatry Dental Care:Partials & Dentures X-Rays Extractions Fillings Cleanings SupportiveServices:Medical CaseManagement Health Literacy Benefits and MedicalInsurance enrollment
Care Alliance cares for the homeless,residents of public housing, and theunderserved. In 2014, Care Alliance provided careto over 10,000 patients, generatingnearly 34,000 encounters. Patient demographics: 45% completely uninsured 45% (4,500 residents) living in public housing Approximately half of patients have a chronic illness 93% at or below 100% Federal Poverty Level
Current LocationsClinic Sites:St. Clair Clinic1530 St. Clair AvenueCarl B. Stokes Clinic6001 Woodland AvenueRiverview Tower Clinic1795 West 25th StreetCentral Neighborhood Clinic2916 Central AvenueMobile ClinicPermanent Supportive HousingPartner Sites: Lutheran Metropolitan Ministry’sMen’s ShelterNorma Herr Women’s CenterThe City MissionWest Side Catholic CenterBishop Cosgrove CenterSt. MalachiCommunity Assessment & TreatmentCenterFrontLine ServiceCenters for Families and ChildrenArbor Park
Common recruitment and retention challenges at CareAlliance Health Center:1. Medical – Charge and/or Staff Nurses2. Qualified and/or experienced candidates
Tactics used to recruit personnel within the communitiesserved by PHPCs:1. Careerboard2. Postings at sites3. Job Openings via Outreach staff4. Colleges
Strategies to recruit and retain clinical and non-clinical staff:1. Remaining comparable in benefits2. Raising salaries to compete with market in samecategories of employment3. Raising awareness about the people we serve at CareAlliance4. Marketing efforts
For more information, please contact:Francis Afram-Gyening, MBA, MPH, FACHEPresident & CEO216-781-6228, ext. 253faframgyening@carealliance.org
Merit Based Incentive Program through which commitment and performance are financially acknowledged with awards of up to 30,000 above the base salary in the year (number for FY 2015). Recruitment Bond of 10,000 (upfront and above base salary) for newly contracted provider. Retention Bond of 5,000 (upfront and above base salary) for provider