Transcription
The 5 Minute Low Back ExamRobert Arnsdorf, MDRehabilitation Medicine AssociatesEugene, OregonDecember 2, 2017
Disclosure Information Presenters Robert Arnsdorf, MD, has nothing to disclose. Bryan Andresen, MD, has nothing to disclose. Planning Committee Jim Chesnutt, MD, has nothing to disclose. Brick Lantz, MD, has nothing to disclose. Erin Owen, PhD, has a spouse who receives a salary from Wright Medical.
GOALS: Define the purposes of a screening physicalexam for low back pain patients Learn a complete, efficient low back exam Assess the validity of such an exam Discuss interesting clinical findings from milesand miles of low backs
Goals of the low back exam:Identify spinal conditions requiringspecific treatment: nerve root injury,fracture, etc.Exclude non-spinal sources of backand leg painCorroborate imaging findings and/orprevent unnecessary imaging
LIMITATIONS: Exact pathology will be identifiable for a minorityof patients with low back pain. ( 15% per Chou,et al.)
Validity of back exam: Unknown Cochrane Back Group, 2010:“When used in isolation, current evidenceindicates poor diagnostic performance of mostphysical tests to identify lumbar disc herniation. Better performance may be obtained whentests are combined .Few studies presented dataon test combinations.”
What do national guidelines say?American College of Physicians and American PainSociety, Chou, et al, 2007:“Clinicians should conduct a focused history andphysical examination to help place patients with lowback pain into one of three broad categories: nonspecific LBP; back pain potentially associated withradiculopathy or spinal stenosis; or back painpotentially associated with another specific spinalcause.” (Strong recommendation, moderate qualityevidence)
What evil lurks in the spines of men?Patients presenting to PCP with low back pain:0.7% Cancer4% Compression fracture3% Spinal stenosis4% Symptomatic disc herniation0.3 to 5% Ankylosing spondylitis (5%?)0.01% Spinal infection0.04% Cauda equina syndrome
Physical Exam Spine and lower limb inspection- Standing Gait- Standing Range of motion- Standing Palpation- Standing Strength- Sitting Sensation- Sitting Reflexes and muscle tone- Sitting Special tests- Lying
Inspection: Patient standing, inshorts with shoes and socks offNote body habitus: Weak correlation between obesity andlow back pain.Assess spinal posture:Kyphosis/lordosisScoliosis: Observe flexion from behindRib hump on convex side of curvePelvis level?If not, estimate lift needed to level
Inspection, continued: Gross contractures in lower limbs Ankle/foot deformities: High arches, anklepronation Muscle mass in lower limbs Color of feet
Gait: Standard walking Walk on heels Walk on toes Single leg stance Low risk of falls if able to stand on each single leg10 seconds or more
Range of motion: Patient standing Flex forward at waist with knees extended.Measure distance from finger tips to ground Extend at waist. Estimate degrees Note any pain provocation ROM not particularly useful, except to assessprogress of a specific patient. ROM is NOTcorrelated with functional disability.
Palpation Have patient put one non-moving finger where thepain is the worst Touch whatever hurts Push on muscles and bones of spine and pelvis Push on greater trochanters of femur, ischialtuberosities, sacrum, piriformis muscles Percuss sacrum, lumbar spinous processes Feel for inguinal adenopathy if appropriate If diffuse muscle tenderness, palpate shoulders also
Strength Testing: Seated Test all available nerve roots and peripheral nerves Test smaller muscles if possible. Look for patterns of weakness: Proximal vs. distal Muscles supplied by a single vs. multiple nerve roots Muscles supplied by a specific nerve vs. multiple nerves Note pain provocation or any give-way weakness
Strength Testing: Hand held dynamometers are tremendouslyhelpful at accurately quantifying weakness. Easier on your back if patient is seated on araised exam table. Assess most of strength in seated positionExceptions: Ankle plantar flexors assessedwalking on toes. Trunk assessed supine.
Hip Flexion:IliopsoasL2-4 RootsFemoral nerve andbranches from plexusLift knee againstresistance
HipAdduction:L2-L4 RootsObturator NerveHave patientspread legs andyou push oninside of knees asthey adduct
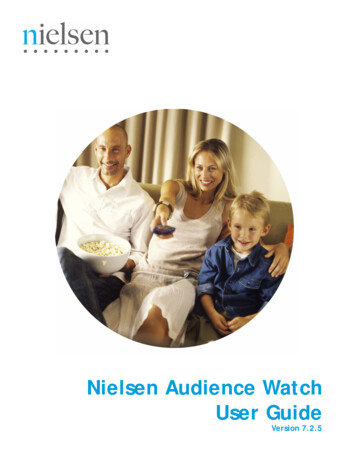
HipAbduction:Glut MediusL4-S1 nerve roots, especiallyL5Superior gluteal nervePatient spreads kneesagainst your hands placed onouter kneesCan test in side lyingPain provocation suggestsgreater trochanter “bursitis”Good way to differentiate L5radiculopathy from peronealneuropathy in foot drops
KneeExtension:QuadsL2, L3, L4 rootsFemoral NerveExaminer tries toflex bent knee aspatient attempts tostraightenVery strong muscle
Knee Flexion:HamstringsL5-S2 RootsSciatic NerveYou straightenknee from flexionas patient resists.
AnkleDorsiflexion:Anterior Tib.L4, L5 RootsPeroneal NerveRaise foot againstresistance
AnkleInversion:Posterior TibL5, S1 RootsTibial NervePush againstmedial foot aspatient plantarflexes and inverts
AnkleEversion:PeronealsL5, S1 RootsPeroneal NervePush against lateralfoot as patienteverts andplantarflexes
Great ToeExtension:EHLL5, S1 RootsPeroneal NerveYou push down aspatient pulls greattoe upwards.
Touch Sensation: Test seatedSharp, broken wooden Q Tip. Single useOther modalities if neededCheck each dermatome: Right vs. left,medial vs. lateral, proximal vs. distalAsk “Which is sharper?”Particular attention to anterior lateral thighs
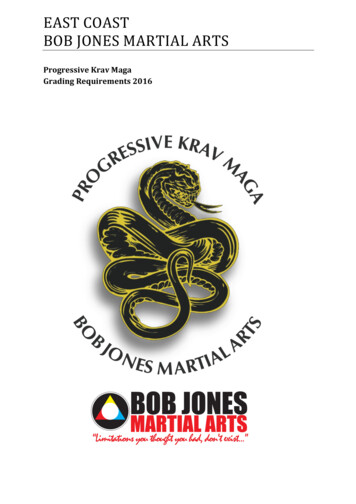
TouchL2- Mid thigh,anteriorL3- Medial kneeL4- Medial ankleL5- Base of D2S1- Lateral Ankle
MeralgiaParestheticaBurning painand/or numbnessin anterior lateralthigh.Edges discreteObese, pregnant,tight belts, etc.Really common
Reflexes: Still sittingAssess L4, L5 and S1 nerve rootsCompare right vs. left, proximal vs. distalIf lower limb abnormal, check upper limbsIf absent, possible lower motor neuron injuryto anterior horn cell, root, plexus, nerveIf increased, possible upper motor neuroninjury to brain or spinal cordWide range of normal
PatellartendonQuadriceps, L4See kneeextend/quadstwitchDo not sit in frontof patient
MedialHamstringsL5 reflexGrasp medialhamstring tendonsjust above kneewith index andmiddle fingers andstrike your fingers.Look and feel forcontraction
Ankle ReflexS1 rootTap Achillestendon and lookand feel for footto plantarflex
BabinskiStroke bottom offoot with end ofreflex hammer.Initial movement ofbig toe should bedown. If not,suggests uppermotor neuroninjury
Clonus?Do while at feetRapidly push up onbottom of foot withone hand whileholding ankle withthe other. 2-3 downbeats normal.If abnormal, checkquads, hip adductorsand upper limbs
Check feet:ColorTemperatureHair growthMuscleatrophy:EDBPulses
Non-organicbehavior:Documentthroughout exam:Purple inkGive way weaknessOver-reactionCaution re: use ofWaddell signs
Special Tests: Patient lying downAbdominal strengthStraight leg raiseHamstring stretchHip rotation/compressionSacroiliac joint tests?Femoral nerve stretch test?
AbdominalsThoracic nerverootsHave patient liedown and do onesit up.
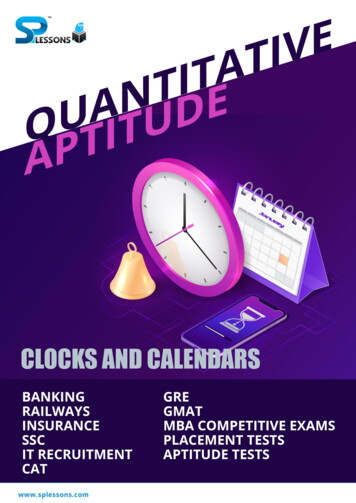
Straight LegRaiseStretches L4, L5, S1rootsLift leg. Note if andwhere pain is feltand at what degrees.Nerve root painincreases with ankledorsiflexion.Check both sides.
Straight legraise validity:Ipsilateral SLR:High sensitivity,widely variablespecificityCrossed SLR:Specific, but notvery sensitive
HamstringlengthHow far can youlift leg with kneestraight?Estimate indegrees.Reproduction ofpain?
Hip Rotation/CompressionDifferentiate hipfrom spinalpathologyHip and knee at90 degrees, pushdown on kneewhile rotating. Ispain reproduced?
SacroliliacTestsPhysical examinaccurate atdiagnosing SIjoint pain.
Femoralstretch testStretches L2, L3,L4 roots.These areuncommon nerveroots to causepain so test isn’ttoo helpful.
Bibliography Gjherbison.com “Physical examination for lumbar radiculopathy dueto disc herniation in patients with low back pain”Cochrane Back Group, Van Der Windt, et al.,Published online Feb, 2010 “Diagnosis and treatment of low back pain: a jointclinical practice guideline from the American Collegeof Physicians and the American Pain Society” Chou,et al, Ann Intern Med, 2007: 147: 478-491
to disc herniation in patients with low back pain" Cochrane Back Group, Van Der Windt, et al., Published online Feb, 2010 "Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society" Chou, et al, Ann Intern Med, 2007: 147: 478-491