Transcription
Welcome toCape Fear Valley Health SystemProvider Orientation
Instructions to ApplicantAll new applicants will be required to review this on-lineorientation as part of their application process. Afterreviewing the slides, please print and sign the confirmationof completion statement at the end of this presentation andinclude it with your application. If you did not complete theorientation prior to submitting your application, pleasereturn the signed statement to he Medical Staff Office to beincluded with your application (by fax to 615-5959 or by email to aennis@capefearvalley.com). An electronic record ofyour completion of this on-line orientation will also bemaintained.
Additional Orientation Requirements Please note that prior to beginning to function at CFVHS there will beadditional on-site orientation steps that will need to be completed.These include, but are not limited to: Computer orientationObtaining ID badgeObtaining parking informationFacility tourPlease contact the Medical Staff Office following review and approvalof your application to schedule this additional orientation. Employed Practitioners – you will need to complete additionalorientation steps through Human Resources. Please contact yourOffice Manager/recruiter following review and approval of yourapplication to schedule this additional orientation.
Purpose and Target AudienceTo provide new providers joining themedical/allied health staff of Cape Fear ValleyHealth (CFVH) information on CFVH policies, ordersets, procedures and peer review practices. Alsoincluded is patient safety information, JointCommission requirements, National Patient SafetyGoals and how CFVH builds a culture of patientsafety. This knowledge will assist you to betteroperate in the CFVHS
Overview of Cape Fear Valley HealthSystem8th Largest Health System in North CarolinaCURRENT FACILITIES: Cape Fear Valley Medical Center – 539 bedsCape Fear Valley Rehabilitation Center – 78 bedsHighsmith-Rainey Specialty Hospital (long term acute care)– 66 bedMelrose Behavioral Healthcare – 32 bedsHoke Hospital – 41 bedsBladen County Hospital (critical access) – 58 bedsPhysician Primary Care & Specialty Clinics – 25 officesEmergency Medical Services (EMS and Lifelink)Health Pavilion North – comprehensive multi-specialtyoutpatient facilityHarnett Health – management agreement
Certifications::AccreditationsAt CFVHS, we are proud to be nationally recognized in so many areas. Ouraccreditations and certifications demonstrate our commitment to quality care. Heart Attack Care: Chest Pain Center Accredited by the Society for CardiovascularPatient Care and Disease Specific Certification by The Joint Commission (TJC).Cancer Care: Accredited by the American College of Surgeons Commission on CancerBreast Care: Accredited by the National Accreditation Program for Breast CentersWeight Loss Surgery: Accredited by the American Society for Bariatric SurgeonsPhysical Rehabilitation: Accredited by Commission on Accreditation of RehabilitationFacilitiesSleep Medicine: Accredited by the American Academy of Sleep MedicineEmergency: Level III Trauma Designation by The NC Department of Health and HumanServicesDisease Specific Certification by The Joint Commission in: Heart Failure Advanced Stroke Care Pneumonia Sepsis (CFVH and Bladen) Hip & Knee Replacement Surgery Wound Care (HRSH)(NOTE: Details regarding Program Goals, PI Measures, Educational Resources and ClinicalPractice Guidelines for areas certified by TJC are available on the Physician Portal)
Building a Culture ofQuality Care and Patient Safety
Zero
Quality Definition :Doing the right thing,the right way,at the right time every time
Six Safe Behaviors with ToolsSafety Behavior ExpectationError Reduction Tool1- Pay Attention to DetailStop, Think, Act, Review (STAR)2- Communicate Clearlyand DirectlySBARRCheck Backs / Repeat BacksPhonetic/Numeric ClarificationsAsk Clarifying Questions3- Perform Effective HandoffsSBARR3 Ws (What? Why? Warnings?)4- Be Aware of Big Picture &Have a Questioning AttitudeStop and AskBriefs/Huddles/Debriefs5- Work Together withYour TeamsEscalation of ConcernsPeer Checking and Coaching6- Follow the RulesKnow the PoliciesFollow ProceduresUse Checklists
Opportunities for failure exist even whenwe practice safe behaviorsBreakdowns Most breakdowns are PROCESS related Breakdowns in BEHAVIOR occur when proceduresare not followed EQUIPMENT breakdowns are the least commonIn order to get better we need to report errors Submit a SIR!
Safety Culture at Cape Fear ValleyOur safety culture revolves around three principles:– Trust– Report– ImproveWe have to TRUST that in our system when we REPORToccurrences IMPROVEMENTS in processes and safety will occur.
What is a SIR? Cape Fear Valley Health’s mechanism toreport, identify, and analyze quality ofcare issues and potential threats forpatient and employee harm SIR stands for Safety Improvement Report SIRs are entered via the Physician Portal
Why are SIRs important? A health system our size should have 15,000-18,000 SIRs ayear Cape Fear Valley Health had over 15,000 SIRs reported in2015! A report of a singular incident may result in immediatesteps taken to protect our patients Each SIR is reviewed by a multidisciplinary team of peopleto gain insight from different perspectives Each SIR is categorized according to the level of harm
How to Enter a SIR1. Access the Physician Portal2. Click on the Feedback/SIR tab
3. Click on Submit a SIR4. Enter SIR information.
How Do We Improve Reliability? Increase the reporting of events We identify “Good Catches” when providersreport events that do not reach the patient We observe and hear providers using the 6Safe Behaviors and error prevention tools Reduce the number of harmful events andgrievances over time
Goal: Robustreporting leading todecreased harm
Fill out a SIR every time for: Delays in treatment Equipment failures, issues, orproblems Patient identification issues Patient injuries, falls Medication issues (orders, labeling,reactions, prescribing) Everyone’s Safety
2016 National Patient Safety Goals Goal #1 Patient identificationUse at least two patient identifiers when providing care, treatment,and services. Patient’s FULL name Including middle initial Including Jr., Sr., III, etc. as applicable Patient’s Date of Birth Goal # 2 CommunicationImprove the effectiveness of communication among caregivers Goal #3 Medication SafetyImprove the safety of using medications
2016 National Patient Safety Goals Goal #6 Clinical AlarmsImprove clinical alarm safety Goal #7 Healthcare Associated InfectionsReduce the risk of health-care associated infections Goal #15 Safety RisksIdentify patients at risk for suicide and take precautions
Keep Safe: Rapid Response What: The Rapid Response Team responds immediately when apatient’s condition is worsening. Rapid Response is also called ifvisitors or staff need medical assistance Who: Anyone can call Rapid Response- a patient, familymember, and any hospital staff member When: Always activate the Rapid Response to assess the patientif you feel the patient doesn’t look right .( i.e. not responding,chest pain, difficulty breathing, seizure) How: Dial 22 CiscoDial *22 NortelTell the operator Rapid Response is needed and yourlocation
Clinical PerformanceImprovement Committee(CPIC)
Clinical Performance ImprovementCommittee (CPIC) To improve the quality of care rendered by theindividual physician and LIP Although Peer Review is a Joint Commissionrequirement, our goal is to share lessons learnedwith Medical Staff to avoid errors Drive true performance improvement Identify operational issues and identify solutions Engage the Medical Staff in improvements fortheir respective departmentsThis document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
Internal Peer ReviewSources of Case Referrals Patient Relations (Patient/familycomplaints/grievances) SIR Safety Improvement Report Hospital department referrals (Infection Control,Case Management, Surgical Services, HealthInformation Management (HIM), Risk Management,etc.) Committee referral (Pharmacy & Therapeutics,Professional Well-Being Committee, etc.)This document is Privileged and Confidential inaccordance with North Carolina Gen. Stat §131E-95 &
Just Culture- CPIC Outcomes The Just Culture approach is helpful incommunicating Peer Review Findings to theindividual staff member and the Medical ExecutiveCommittee (MEC). It assists CPIC in drilling down further to addressbroader physician or hospital system issues. Identification of system/process opportunities.This document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
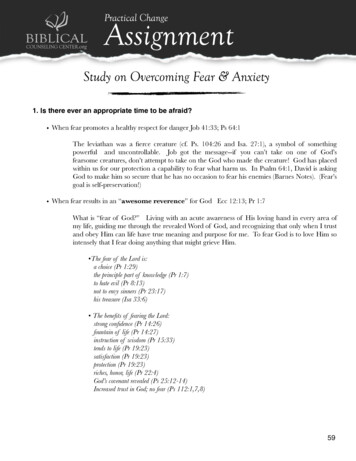
Issue:Were theActionsactions gly ViolatedSafe OperatingProcedures?YesNoWere theConsequencesas Intended?YesClinical Performance Improvement Committee (CPIC) PeerReview Algorithm**Adapted from James Reason “Managing the Risksof Organizational nce AbuseWithout MitigationNoNoCulpableHistory ofPriorErrors?YesGray AreaHumanError?NoNo ErrorNoYesSystem InducedErrorMedical ImpairmentYesDeficiencies inSelection, Training orExperience?Reckless BehaviorSabotage, MalevolentDamage, etc.YesNoWere ProceduresAvailable, Workable,Intelligible and Correct?YesPassSubstitutionTest?Repetitive Human ErrorsCorrective Training orCounseling IndicatedHuman andSystem InducedErrorIsolatedHumanErrorAvoidable MedicalErrorHuman ErrorNo ErrorDocumentation Issue: Specify:This document is Privileged and Confidential in accordancewith North Carolina Gen. Stat §131E-95 & §131E-76 (5)
Ongoing Professional PracticeEvaluation(OPPE)Focused Professional PracticeEvaluation(FPPE)This document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
Ongoing Professional PracticeGuidelines,(OPPE) Joint Commission Requirement to evaluateperformance of the medical staff OPPE – 6 month evaluation of key indicatorswithin the physician practice. Each physician meets with their section chair toreview their OPPE.This document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
Focused Professional Practice Review(FPPE)There are three reasons a FPPE may be conducted.1. Orientation to a new facility Medical Staff arranges this review.2. New credentials (Procedures etc.) Medical Staff arranges this review and may requireproctor.3. Trended Opportunities for Improvement This FPPE may be recommended by Medical ExecutiveCommittee from recommendation from CPIC. Qualityand Patient Safety will arrange for this review.This document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
PhysicianProfiles
Patient Safety and QualityEvidence-Based Care:CFVHS believes the use of evidence-based care allowsus to provide the highest quality care for our patients.CFV evidence based care order sets include: Heart Failure (CHF) Heart Attack (AMI) Community Acquired Pneumonia (CAP) Surgical Care Improvement Project (SCIP) Sepsis Stroke(NOTE: A copy of all order sets are available through Form Fast. Recently adopted/updatedorder sets will be available on the Physician Portal for a period of two months afterimplementation)
The Joint CommissionDisease Specific CertifiedProgramsat Cape Fear Valley Health
Joint Commission Certified - Acute Myocardial InfarctionProgramProgram Goals:Provide Evidence Based Care from admission all the way to post discharge care.Promote Self Management through education.Performance Improvement Measures:Troponin collect to result time 60 minsDoor to Balloon TimeAMI All Cause ReadmissionsAMI LOSWe also Track (not for Joint Commission Purposes):Meds at D/C: ASA, Statin, Beta Blocker, ACE/ARB for EF 40%ASA on arrivalEducational Resources:AMI HQI Packet on FormFastCardiac Health Education BookDischarge InstructionsCare NotesUp-To-DateMosby’s Nursing Skills and ConsultAMI Coordinator- (910) 615-7083Clinical Practice Guidelines:Can be found on the infoweb- References- Clinical Practice Guidelines- AMI GuidelinesAmerican Heart AssociationAmerican College of CardiologySociety for Cardiovascular Angiography and Interventions
Joint Commission Certified -Advanced Stroke ProgramProgram Goals:Improve use of evidence based careIncrease patient satisfactionReduce length of hospital stayReduce 30 day readmissionsReduce mortalityPerformance Improvement Measures:Thrombolytic AdministrationAntithrombotics by Day of stay 2VTE Prophylaxis by Day of stay 2Stroke EducationAnticoagulation for A-FibAssessed for RehabDischarge on StatinsAntithrombotics @ D/CEducational Resources:Stroke HQI PacketStroke Education BookletDischarge InstructionsInfoWeb: Care Notes, Up-To-Date, Mosby’s Nursing Skills & Consult, Stroke References- Found Under the“Reference” TabStroke Coordinator (x7077)Clinical Practice Guidelines:*Available from any computer terminal; on the InfoWeb, under the reference tabAHA/ASA 2015- Guidelines for Early Management of Patients with Acute Ischemic StrokeAHA/ASA 2015- Guidelines for the Management of Aneurysmal Subarachnoid HemorrhageAHA/ASA 2011- Racial-Ethnic Disparities in Stroke Care: The American ExperienceAHA/ASA 2015- Guidelines for the Management of Spontaneous Intracerebral HemorrhageAmerican Academy of Neurology 2014- Guidelines for the Early Management of Adults with Ischemic Stroke
Certified Joint Commission- Heart Failure Care ProgramProgram Goals:Improve use of evidence based careIncrease patient satisfactionReduce length of hospital stayReduce 30 day readmissionsReduce mortalityPerformance Improvement Measures:Follow Up Appointment within 7 Days of DischargeSystolic BP 140 and Diastolic BP 90 by DischargeEvidence Based Beta Blocker if EF 40%Lipid Lowering Medication Ordered at Discharge if Co-morbid:CAD or CVA or PVD or DiabetesEducational Resources:CHF HQI PacketCHF Education BookDischarge InstructionsInfoWeb: Care-notes, Up-To-Date, Mosby’s Nursing Skills & ConsultHeart Failure Coordinator (x4809)Clinical Practice Guidelines:*Available from any computer terminal; on the InfoWeb, under the reference tab2013 ACCF/AHA Guideline for the Management of Heart Failure: Executive Summary: A Report of the AmericanCollege of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.
Joint Commission Certified- Pneumonia ProgramProgram Goals:Improve use of evidence based careIncrease patient satisfactionReduce length of hospital stayReduce 30 day readmissionsReduce mortalityPerformance Improvement Measures:Influenza Vaccination RatesPneumococcal screening/vaccination rate30 day all cause readmissionsAppropriate Antibiotic Selection for Pneumonia PatientsWe also track the following Measures:Blood cultures, ICU patientsMortalityHealthcare Associated PneumoniaLength of StayEducational Resources:Pneumonia HQI PacketDischarge InstructionsInfoWeb: Care Notes, Up-To-Date, Mosby’s Nursing Skills & ConsultPneumonia Coordinator (x7015)Clinical Practice Guidelines:Can be found on the infoweb- References- Clinical Practice Guidelines- Pnuemonia ClinicalPractice GuidelinesInfectious Diseases Society of America/American Thoracic Society Consensus Guidelines on theManagement of Community-Acquired Pneumonia in Adults (2007) andGuidelines for Management of Adults with Hospital-acquired, Ventilator-associated, andHealthcare-associated Pneumonia (2005)
Joint Commission Certified -Race 2 RecoveryElective Hip/Knee ReplacementProgram Goals:Improve the quality of patient careIncrease patient satisfactionImprove outcomesIncrease patient knowledge of events to comeDecrease Blood TransfusionsPrevent infectionsPerformance Improvement Measures:Pre-op class attendance30-day All-Cause ReadmissionsReduction of Nausea and Vomiting in Post Operative Hip and Knee PatientsFunctional Ambulation Status Improvement for Hips to ambulate / 250 feetAnd Knees to have a zero degree extensionEducational Resources:Race 2 Recovery GuidebookRace 2 Recovery Patient Education SeminarDischarge InstructionsCare NotesUp-To-DateMosby’s Nursing Skills and ConsultClinical Practice Guidelines:*Available from any computer terminal: infoweb, Reference tab, Clinical Practice Guidelines*The American Academy of Orthopedic Surgeons (AAOS):The Clinical Practice Guideline on Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hipand Knee Arthroplasty – September 2011*American Society of Health System Pharmacists (ASHP):Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery – 2013
Joint Commission Certified- Sepsis ProgramProgram Goals:Early Identification of signs and symptoms of sepsis through screeningDevelop and sustain a smooth orchestration of care in the Emergency Department from triage to earlyidentification and implementation of goal directed therapy.Develop and sustain a smooth orchestration of care within the adult inpatient population from earlyidentification to implementation of goal directed therapy.Initiation of medical treatment with the use of order sets (CPOE and EMSTAT) based on positive screening.Education to the patient/family or caregiver to assist with self-management of their disease process byreducing the risk factorsCommunity awareness: ImmunizationsEducation to clinical staff to include physicians, mid-level providers, and nursing staff.Performance Improvement Measures:Lactate CollectedFluid Resuscitation (30ml/kg)Appropriate ScreeningComposite ScoreWe also track the following Measures:Blood culturesMortalityLength of StayReadmissionsEducational Resources:Sepsis Educational HandoutDischarge InstructionsInfo Web: Care Notes, Up-To-Date, Mosby’s Nursing Skills & ConsultPneumonia/Sepsis Coordinator (x7015)Clinical Practice Guidelines:Can be found on the info web- References- Clinical Practice Guidelines- “Surviving Sepsis Campaign:International Guidelines for Management of Severe Sepsis and Septic Shock: 2012”
Joint Commission Certified- Wound Care ProgramProgram Goals:Improve use of evidence based careIncrease patient satisfactionIdentify risk for skin breakdownImplement strategies to prevent and/or manage pressure ulcersReduce pain and minimize infectionReduce and mitigate the overall incidence of pressure ulcersReduce risk factors that contribute to the development of pressure ulcersMonitor the incidence and severity of pressure ulcersPromote an optimal level of function, comfort and quality of lifeMonitor and evaluate outcomesPerformance Improvement Measures:Nutritional Supplements Implementation during HospitalizationReduce Hospital Acquired Pressure UlcersWound Treatment Orders Initiation on AdmissionEvidence of Self-management Knowledge Prior to DischargeEducational Resources:Wound Care HQI PacketDischarge InstructionsInfoWeb: Care Notes, Up-To-Date, Mosby’s Nursing Skills & ConsultWound Care Coordinator (x1106)Clinical Practice Guidelines:Nutritional information can be found on the InfoWeb- References- Clinical Practice Guidelines- Prevention and Treatment ofPressure Ulcers Clinical Practice GuidelinesNational Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Paneland Pan Pacific Pressure Injury Alliance (2014)
Surgical Care Improvement Project (SCIP) Prophylactic antibiotics given within 1 hour prior to surgical incision (2 hrs for vanco)Prophylactic antibiotic selection consistent with current guidelinesProphylactic antibiotics DC’d within 24 hours of anesthesia end time (48 hrs for cardiac)Clippers for hair removalControlled post-op serum glucose (cardiac patients, POD 1&2 180)Recommended VTE prophylaxis within 24 hours of anesthesia end timeBeta Blocker given the day before surgery and/or the day of surgery and POD 1 and/orPOD2Urinary Catheter Removed by POD 1 or 2 an order to utilize he urinary catheter removaljustification protocol will allow nursing documentation to be acceptableSurgery patients with Perioperative Temperature ManagementBe Sure to Document:--Document therapeutic reason for continuing antibiotics beyond approved time frame--Contraindications to VTE prophylactics if not ordered--Document valid reason for not removing urinary catheter (must be documented on POD 1 or 2)
Mandatory Order SetsThe Medical Executive Committee has mandated thatphysicians use the following order sets: AMI, HF, PneumoniaThe use of the following order sets is highlyencouraged: Stroke, Sepsis, DVT Central Line Bundles Ventilator Associated Bundle Blood OrderOrder sets can be found in CPOE
Infection Prevention and ControlProvider OrientationThis document is Privileged and Confidential in accordance withNorth Carolina Gen. Stat §131E-95 & §131E-76 (5)
Hand Hygiene Use alcohol waterless hand wash as primary means to sanitizehands Use soap and water if:– Visible contamination is present on hands or gloves– Questionable contact with fecal material occurs. You mustwash your hands with soap and water. Alcohol base hand rubs are ineffective against Clostridium difficile. When to perform hand hygiene:–––––––Before & after workBefore & after contact with each patientAfter contact with soiled materialBefore & after using bathroomBefore handling food or medicationsBefore donning gloves & After removing glovesBefore entering AND when exiting a patient’s room
Isolation Practices at CFVHS When indicated, isolation is used in addition to Standard Precautions– For Inpatient Settings, CDC’s Transmission Based Isolation Categoriesare used. Airborne Special Airborne Contact Contact Contact Special Enteric Droplet Protective– For Outpatient Settings, CDC’s Syndrome Based Precautions are used. The CDC HICPAC Isolation Table is available on the Infowebunder References Compliance regarding protective personal equipment isnecessary to reduce risk of transmission to other patients.
MDRO: Methicillin ResistantStaphylococcus Aureus (MRSA) More severe, life threatening MRSA infections occur mostfrequently among patients in health care settings– Patients at risk – weakened immune systems, wounds, cathetersinserted, procedures make it easier for MRSA to enter body– Contact Isolation Precautions– Hand Hygiene with alcohol foam or soap and water The most common body site colonized is thenose– Clearance Protocol FormFast 0856 Two swabs of the nares: One swab taken, upon returnof negative result collect second l
MDRO: Clostridium Difficile (c.diff) Linked to 14,000 American Deaths each year Most at risk – patients receiving antibiotics, PPI, GI surgery,long length of stay, elderly, immunocompromised, Shed in feces – c.diff spores transferred via healthcarepersonnel’s hands– Soap and Water for Hand Hygiene– Contact Special Enteric CFVHS Lab Specimen– Must be loose/liquid stool (Bristol Stool Type 7)– NOT recommended to retest within 7 days of positive No test for clearance Treatment –metronidazole, PO vanc, fidaxomicin– Refer to Fecal Microbiata Transplant Policy for persistent c.diff1. http://www.cdc.gov/
CAUTI Prevention MeasuresCore MeasuresSupplemental Measures Insert catheters only forappropriate indications Leave catheters in place only aslong as needed Only properly trained personsinsert and maintain catheters Insert catheters using aseptictechnique and sterile equipment Maintain a closed drainagesystem Maintain unobstructed urine flow Hand hygiene and standard (orappropriate isolation)precautions Alternatives to indwellingurinary catheterization Portable ultrasound devicesto reduce ac/cauti/001 cauti.html
CLABSI Prevention MeasuresCore Measures Removing unnecessary CL Following proper insertionpractices Facilitating proper insertionpractices* Complying with hand hygienerecommendations Performing adequate skincleaning Choosing proper CL insertionsites Performing adequatehub/access port cleaning Providing education on CLmaintenance and insertionSupplemental Measures Implementing chlorhexidinebathing* Biopatch*Not part of 2002 HICPAC Guidelines for the Prevention of Intravascular CatheterRelated Infections
Infection Control DepartmentBusiness Hours: Monday to Friday 8:00 to 4:30Phone Number: 615-4792After Hours for urgent issues use Chain ofCommand – Nursing Supervisor.Nursing Supervisor can reach Infection Controlafter hours
Why Antibiotic Stewardship? Evidence shows antimicrobial use is:– Over 50% of the time inappropriate– The 2nd most common cause of adverse events– Frequently associated with prescribing errors– Associated with super infection such asClostridium difficile infection Goal: Optimize antimicrobial therapy whileminimizing resistance and adverse reactionsClinical Infectious Diseases 2007;44:159-77
Antimicrobial Stewardship at CFV Inter-professional subcommittee of P&T Responsible for antimicrobial formulary,policies, and education Utilizes a pharmacist to review antibiotic useand provide prospective feedback to optimizetherapy including:– Bug/Drug mismatch– De-escalation and Duration of therapy– IV to PO and dose optimization changes
KEY POLICIES/PROCEDURES
Medical Staff Bylaws and Related Documents/HealthSystem Policies and ProceduresMembers of the staff are expected to be familiar and complywith the Medical Staff Bylaws, Rules and Regulations andCredentials Policies and Procedures as well as related medicalstaff policies. In addition, staff members are expected to beaware of and comply with Health System policies. The MedicalStaff Bylaws and related documents are accessible through thePhysician Portal and a summary was provided with yourapplication to the staff. Health System policies are availableelectronically through PolicyTech and key policies are availableon the Physician Portal for ease of access.
Do Not Write or UsePlease note the following key points: “Resume or Continue” such as “resume pre-op orders” or“resume home medications” – these orders must be writtenout. DNR/DNI simultaneously – must specify only one or order isinvalid and staff will call for clarification U for units – write out units QD – write out “daily” or “every other day”(NOTE: A complete list of unapproved abbreviations is availableon the Physician Dashboard).
Telephone Order Read BacksThe preference is that you write orders inpatient records yourself. If this is not possibleyou are required to authenticate your orderwithin 96 hours. You and your colleagues thatcover for you can sign these orders for eachother. This is both a patient safety and qualityof care issue. In addition, this is a regulation ofthe Centers for Medicare and Medicaid and TheJoint Commission.
Legibility*Legibility of your documentation can have a significantimpact on patient safety and quality of care.*Legibility of your documentation is important tofacilitate timely and accurate reimbursement andreduce potential liability for you and the health system.*Legibility – to assist staff in following up shouldillegible orders be identified, you are to include yourphysician ID/dictation number with your signature onall orders.
Writing Medication Orders Use CPOE or approved order form Sign, date and time order; include IDnumber in compliance with legibilitypolicy Include drug name, dose, frequency androute of administration Weight based dosing is required forpediatric orders Place prescriptions in the chart, do notgive to the patient or family
Restraint/Seclusion Orders Medical/Surgical Restraint orders are active up toone calendar day (order expires at 11:59 pm the nextday). Orders require a face-to-face assessmentwithin a calendar day of the order. Behavioral Restraint orders are active for a limitedamount of time (based on patient’s age). Ordersrequire a face-to-face assessment within one hour ofa new restraint order.NOTE: The complete “Restraints, Seclusion and Safety Devices” policy isavailable via the Physician Dashboard. The Restraint/Seclusion order set isavailable through Form Fast)
Blood Utilization(being reviewed by April Maroschak)Products available throughTransfusion Services: Packed Red Blood Cells (PRBC)Frozen PlasmaCryoprecipitateSingle Donor Apheresis PlateletsRh Immune Globulin (Rhogam)Micro Dose Rh Immune GlobulinComponet AlliquotsIrradiated Blood ProductsLeukoreduced Blood ProductsServices Offered by TransfusionServices: Autologous Transfusion andDirected Blood Donation(coordinated through the BloodDonor Center Therapeutic Phlebotomy(coordinated through the Infusionand Injection Series Clinic) Blood Conservation Program –available to patients seekingalternatives that limit the use ofblood or blood products.(NOTE: Additional detail regarding transfusionservices is available on the physician portal)
CPOE- A Brief IntroductionWith health care reform underway, the importance of increasing patientsafety daily using an electronic order entry system supports Cape FearValley’s mission of: “Improving the quality of every life we touchthrough commitment of excellence by our providers.” Reduced medication errors and adverse drug eventsStandardization and improvement of careImproved efficiency of care deliveryStatistics show a direct correlation between consistent use of CPOE and improvements inquality and safety:– efficiency of patient care; reduction of health disparities, increased engagement with patients andfamilies;– Improved care coordination; adequate privacy and security of personal health information; andpublic health61
Helpful Tips: Please ensure patient is in a bed in ValleyLink before order entry! On admission- Perform the Admission Medication ReconciliationBEFORE you enter you
Meds at D/C: ASA, Statin, Beta Blocker, ACE/ARB for EF 40% ASA on arrival Educational Resources: AMI HQI Packet on FormFast Cardiac Health Education Book Discharge Instructions Care Notes Up-To-Date Mosby's Nursing Skills and Consult AMI Coordinator- (910) 615-7083 Clinical Practice Guidelines: