Transcription
15 TH EDITION 20131Letter from the Editor2Bench-to-Bedside: Translating Medicine, Motivating Patients & Sustaining Environments10Opportunities for Sustainable Designing in Skilled-Nursing Culture Change20Evolution of the ED
Please visit the Academy’s Web site, www.aia.org/aah,for more information on the Academy’s activities.Questions?Please direct inquiries to AAH@aia.org.About the AcademyThe Academy of Architecture for Health (AAH) is one of 21 member communities of the American Institute of Architects.The AAH is unique in the depth of its collaboration with professionals from all sectors of the healthcare community, includingphysicians, nurses, hospital administrators, facility planners, engineers, managers, healthcare educators, industry and governmentrepresentatives, product manufacturers, healthcare contractors, specialty subcontractors, allied design professionals, andhealthcare consultants.The AAH currently consists of approximately 6,893 members. The Academy improves the quality of healthcare through design bydeveloping, documenting, and disseminating knowledge; educating healthcare architects and other related constituencies; advancingthe practice of healthcare architecture; improving the design of healthcare environments; and affiliating and advocating with othersthat share our vision and promoting research.Please visit the Academy’s Web site, www.aia.org/aah, for more information on the Academy’s activities.Please direct inquiries to aah@aia.org.AIA Academy of Architecture for Health Board of Directors 2013PresidentDirector of OperationsIndustry Liaison/Regional InitiativesRoger Call, AIA, ACHA, LEED APHerman Miller for Healthcareroger call@hermanmiller.comOrlando T. Maione, FAIAMaione Associatesomaione@optonline.netR. David Frum, AIAClark/Kjos Architects LLCdavidfrum@ckarch.comPresident-Elect 2014/AAHF /EventsFernando L. Rodrigues, AIAHOK–Houston TXfernando.rodrigues@hok.comCharles H. Griffin, AIA, FACHA, EDACWHR Architects, Inc.cgriffin@whrarchitects.comDesign Awards/Initiatives/Emerging ProfessionalsPast President/Vision and StrategyEducationWilliam L. Schlein, AIA, LEED APAnthrotects Architects, Inc.wschlein@whrarchitects.comTatiana Guimeres, Assoc. AIAHKS Architects, Inc.tguimaraes@hksinc.comCharles H. Griffin, AIA, FACHA, EDACWHR Architects, Inc.cgriffin@whrarchitects.comResearch/Codes and StandardsMarc Marchant, AIA, ACHA, LEED APHerman Miller for Healthcareroger call@hermanmiller.comDan H. Noble, FAIA, FACHA, LEED APHKS Inc.dnoble@hksinc.com
Letter from the EditorThis is the 15th edition of the Academy Journal, published by the AIA Academy of Architecture for Health(AAH) knowledge community. As the official publication of the Academy, the Journal electronicallypublishes articles of particular interest to AIA members and the interested public involved in the fields ofhealthcare architecture, planning, design, research, and construction. Since 2005 we have also publisheda hard copy version of the Journal that has expanded our distribution worldwide. The goal has alwaysbeen to promote awareness and educational exchange between architects and healthcare providers and tobroaden our base of understanding about our clients.Articles are submitted to, and reviewed by, an experienced nationally diverse Editorial Review Committee(ERC). Over the years, the committee has reviewed over 183 submitted articles and responded to countlesswriters’ inquiries, and encouraged and assisted numerous writers in achieving publication. The Journalhas provided valuable opportunities for new and seasoned authors from the architecture and healthcareprofessions. With this issue, three articles have been selected and printed supporting the enhancement ofthe built environment for healthcare. Throughout the 14-year historyof the Journal, the authors have included architects, physicians,Mission of the Academy Journalnurses, other healthcare providers, academics, research scientists,As the official journal of the AIA Academy of Architectureand students from the United States and many foreign countries.for Health (AAH), this publication explores subjects ofinterest to AAH members and others involved in thePublished articles have explored a broad range of medical topics,fields of healthcare architecture, planning, design,including trends and the future of healthcare architecture, cardiacand construction. The goal is to promote awareness,care, future and evolving technology, patient rooms and patientsafety, lighting design for healthcare, psychology, workplace design,educational exchange, and advancement of the overallcancer care environments, emergency care, women’s and children’sproject-delivery process and building products.care, and various healthcare project delivery methods. Visit theAcademy Journal archives at www.aia.org/practicing/groups/kc for earlier articles you may have missed.We would like to encourage more graduates who have received healthcare research scholarships and othersinvolved with research within the architecture for healthcare fields to submit their research to the Journalfor publication consideration. We will continue to develop a cross-referenced article index and a broaderbase of writers and readers. The deadline for the 2014 Call for Papers is May 30, 2014.My special thanks to the AIA for its continued support and hard-working staff, and to the many volunteerswho have contributed to our growing and continued success. I would especially like to thank the othermembers of the 2013 ERC: James G. Easter Jr., FAAMA, Assoc. AIA (Tenn.); Ed Jakmauh, ACHA, LEEDAP (Pa.); Joyce Redden (Tenn.); John Sealander, AIA, ACHA (Calif.); Professor Kent Spreckelmeyer,PhD, FAIA (Kan.) and Janice Stanton, RN, MBA, EDAC, LEED Certified (Ill.).As always, we appreciate your feedback, comments, and suggestions by calling AIA KnowledgeCommunities Manager Susan Parrish at 202-626-7332 or me at 631-246-5660.Orlando T. Maione, FAIA, ACHA, NCARBEditor, Academy JournalNovember 2013A I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A H 1
ACADEMY JOURNALBench-to-Bedside: Translating Medicine, Motivating Patients & Sustaining EnvironmentsBy Sharon E. Woodworth, AIA, ACHAAbstractDesigning environmentsfor the treatmentand cure of chronicneurological disordersis among the greatestchallenges in healthcarearchitectureVancouver’s University of British ColumbiaCentre for Brain Health is a 135,000-squarefoot clinical research facility containing wetand dry labs in addition to patient clinics, allof which are dedicated to neurological andpsychiatric diseases ranging from Lou Gehrig’sdisease, Multiple Sclerosis, Parkinson’s,and Alzheimer’s to resistive Psychosis.Designing environments for the treatmentand cure of chronic neurological disorders isamong the greatest challenges in healthcarearchitecture, made even more so when thedriving vision for this institution was to have100% patient participation in research. Threeaspects aligned to support that vision andadvance a new building typology: TranslatingMedicine, Motivating Patients, and SustainingEnvironments. This paper addresses eachaspect with the belief that when the fields ofeducation and healthcare architecture overlap,this triad must be considered in order toachieve true design excellence. TranslatingMedicine provides an overview of the history,challenges, and architectural motif inherent ina translational medicine facility; MotivatingPatients describes the specifics of how a neuropsychiatric environment can be supportive, thevalue of a supportive environment for patientsof any clinical diagnosis, and the interiordesign motif intrinsic to translational medicinefacilities; and Sustaining Environments offersa summary of what a translational medicinefacility can achieve for the environment andsociety in general.ArticleA University Teaching Hospital’sNeuro-Psychiatric VisionDesigning environments for the treatmentand cure of chronic neurological disordersis among the greatest challenges inhealthcare architecture—case in point: The135,000-square-foot Djavad MowafaghianCentre for Brain Health is a clinical research2 A I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A Hfacility containing wet and dry labs in additionto patient clinics, all of which are dedicated toneurological and psychiatric diseases rangingfrom Lou Gehrig’s disease, Multiple Sclerosis,Parkinson’s, and Alzheimer’s to resistivePsychosis. This soon-to-be-completed facilitywas conceived over 10 years ago by Dr. MaxCynader, along with a host of research faculty,neuroscientists, psychiatrists, nurses, andclinical staff. The site provided for this longawaited project is the gateway to the HealthScience departments on the University ofBritish Columbia campus in Vancouver with adirect adjacency to Vancouver Coastal Hospital.For the architectural team, both entities areclients: Cynader is procuring the constructionfunds for the facility and Vancouver CoastalHealth Research Institute will operate thebuilding upon its completion.The driving vision for this institution isCynader’s objective to have 100% patientparticipation in research. Three aspectsaligned to support that vision and advancea new building typology: TranslatingMedicine, Motivating Patients, and SustainingEnvironments. This paper addresses eachaspect, as outlined below, with the beliefthat when the fields of education andhealthcare architecture overlap, this triadmust be considered in order to achieve truedesign excellence.Translating Medicine—provides anoverview of the history, challenges, andarchitectural motif inherent in a translationalmedicine facility.nMotivating Patients—describes the specificsof how a neuro-psychiatric environmentcan be supportive, the value of a supportiveenvironment for patients of any clinicaldiagnosis, and the interior design motif intrinsicto translational medicine facilities.n
Sustaining Environments—offers a summary to intermingle students and faculty amongof what a translational medicine facility candisciplines, allowing for the exchange (andachieve for the environment and societycreation) of new ideas and philosophies.in general.This university campus dynamic ofTranslating Medicinecollaborative environments was soon becomingIn the field of medicine, “caring” and “curing” apparent in the healthcare arena as well.are two different disciplines: the formerSeveral industry leaders attribute the idea ofinvolves clinicians focused on a patient’s needs, collaborative healthcare to cancer centers;while the latter involves researchers dedicatedover the past decade, these institutionsto conquering a disease. As modern medicinediscovered if they could not cure everyone, thehas evolved, these two branches of healthcareleast they could do is care for the individualhave grown in parallel directions with less and with a terminal illness. To this end, cancerless crossing of the two disciplines, but in thecenters developed a multi-faceted focus onlast decade medical professionals have begunproviding patient care while continuing toseeking a new breed of medicine that blendsadvance progressive insights on treatmentthe art of caring with the science of curing.and life-saving cures. This natural blendingThis blended typology is commonly referredof resources, bringing together clinical andto as “translational medicine” where healingresearch space, was soon supported financially.and learning are meant to intertwine, with theinsights of one discipline informing the other.Government agencies that provide researchfunds—such as the National Institutes ofAs architects who specialize in eitherHealth (NIH)— discovered the value ofhealthcare or research labs, how do we graftblending caring with curing; incentivesthese separate building typologies? Successful were established to motivate the industry totranslational medicine design requires a thought consider alternative research approaches byprocess that sees not the radical differencesmandating interdisciplinary strategies. Theseof each typology but the best features ofinterdisciplinary research operations wereboth environments. To blend the realm ofquickly followed by building designs thatexam tables with the domain of lab benchesmirrored the blended aspects of caring andrequires “translational thinking”—that is ancuring, where clinician and scientist could seeunderstanding of healthcare and researcheach other on a daily basis with the possibilityfacility design with enough insight to discover that sightings of the other might stimulatewhere the two parts can come together ina conversation leading to an otherwisesupport of a new whole.unrealized discovery.nDiscovering this new whole begins withunderstanding the original purposes for whichthe philosophy was developed. The divergentroots of translational design stem from boththe healthcare industry and natural science’sobservation that healing capabilities andresearch achievements had reached a veritableceiling with current facility templates. The firsttranslational facilities were seen in the fieldof natural science education, and today multidisciplinary department buildings are becomingstandard fixtures in the collegiate setting.Simply stated, few institutions erect biologydepartment buildings any more. Administratorsnow invest in “life science” buildings designedSuccessful translationalmedicine designrequires a thoughtprocess that sees not theradical differences ofeach typology but thebest features of bothenvironments.The parallel aspect of life sciences’ focus on“wholeness” and cancer centers’ attention to“caring despite a cure” can set the stage for apowerful blending of the best minds and peopleall in one place. And this place, as a new wholethat retains the best features of their originalparts—that is environments that are conduciveto multi-faceted learning and environments thatare favorable to comprehensive care—is thefoundation for translational thinking.Proceeding from this “translational” thoughtprocess to successful design requiresanticipating the inherent challenges oftranslational design. Quite simply, the vastlyA I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A H 3
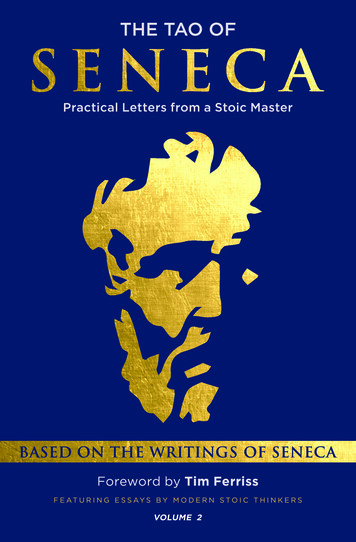
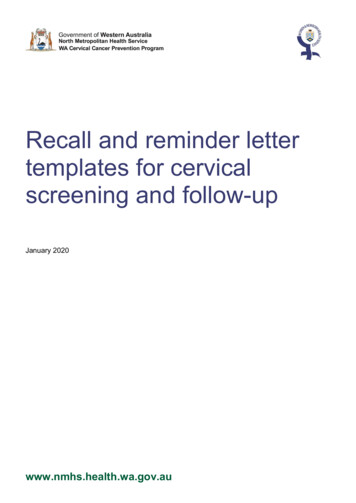
ACADEMY JOURNALFigure 1: Diagram of Lab Boxgeneric population that allows any and allresearchers to function as research grantschange over time, whereas clinical architectscustomize a standard module to ensure designsmeet the specific needs of a patient specialtywhile allowing any and all practitioners tofunction in the module despite future medicalevolutions. Both designs achieve flexibility,yet both are arrived at by engaging usersdifferently. Translational medicine designrequires thinking simultaneously aboutdifferent user processes while discovering thecommon features of flexibility and efficiencythat will benefit both.From the perspective of healthcareadministrators and/or principal investigators,the facility systems can be a challenge withpotential for no-one-wins conflicts. Standalonehospitals and research facilities typically haveprecise structural grids and mechanical systemsthat do not align when in a single structure.Even the diverse building codes associated witheach facility type can create conflicts when asingle building is desired.Figure 2: Diagram of Clinic Boxdifferent needs of research labs and healthcareenvironments should not undermine the bestthat both worlds can offer.In its purest form, translational means“bringing all parties together” which, as designpractitioners quickly recognize, requires theblended discussion of parties that seldomshare the same conference room table. Asarchitects specializing in either research labsor healthcare, an inherent challenge stemsfrom the “poles apart" mentalities involvedin designing space for two disparate uses.Architects associated with research buildingsare typically accustomed to designing for a4 A I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A HThe Centre for Brain Health addressed thesepotentially conflicting architectural differencesby first challenging the design assumptionthat a single-building volume is the mostefficient and economical. The project literallysplit the program into two boxes separatingthe disciplines, each with a structural andmechanical system appropriate for therespective lab or clinic needs; these boxes thenrotate and interlock such that the slender labbox is suspended above half of the very broadclinic box.The clinic box is divided by an atriumbifurcating staff zones separate from patientzones, with the later free from lab systemconstraints. By rotating the research labs’ threeupper floors away from the patient zones,each service has the appropriate structuralgrid and mechanical service; the portion of thetwo floors directly under the research labs areconfigured as clinic staff support spaces, whichtolerate the lab grid and simultaneously offers apure clinic-staff to research-staff vertical zone.
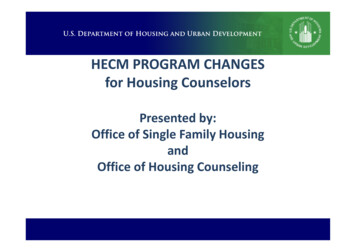
Figure 3: Five-Story AtriumOnce conflicts between architectural systemsare addressed, the clients’ contradictoryoperational needs must be considered. Thismay entail vastly different hours of operationand carry over into the overall arrangement ofpublic versus private spaces. Research facilitiesoften feature discrete, staff-only entries as wellas back-of-house access for research animalsor autopsy samples whereas, conversely,clinical environments usually encourage openspace and a sense of entrance/arrival, fosteringclinician and patient interaction as well asvisitor engagement.can benefit from seeing each other; atriums alsofoster physical opportunities for interactingon a random basis and exchanging either newfindings or new care paths.The Centre for Brain Health’s two programboxes interlock with a five-story atrium asthe connective tissue literally joining allbuilding activities so patients and researcherscan meet by chance “in a single space formutual benefit,” says David Martin, AIA,the project designer and principal for theLondon office of Anshen Allen, now a part ofStantec Architecture.Motivating PatientsAtriums, as a building concept, bring diverseparties together, but in translational medicinea strong design concept that succeeds at“chance meetings for patient and staff” doesnot guarantee that those patients will participatein research. It takes more than a randominteraction or chance encounter to motivatepatients to participate in finding their cure.Even having unlimited research funds availablewill still result in little research if there are nopatients upon which studies can be conducted.In order for patients to feel motivated—motivated enough to give time, donate tissue ororgans, and risk not receiving a miracle drug—they must first have felt cared for, and thatmeans the architectural environment must meettheir physical and emotional needs.Ultimately, translational medicine facilitiesmust seek ways to create visual and physicalopportunities for collaboration, and atriumshave proven to be an inherent architecturalmotif for this new building typology. Atriumsallow visual access into and from research labsso that both research investigator and patientThe needs of neuro-psychiatric patients arewholly unique. Patients with neurologicaldiseases most often have movement disordersranging from the simple need to rest or thecontradictory inability to start walking only tothen be unable to stop walking as their rhythmis literally off balance. Patients with psychiatricA I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A H 5
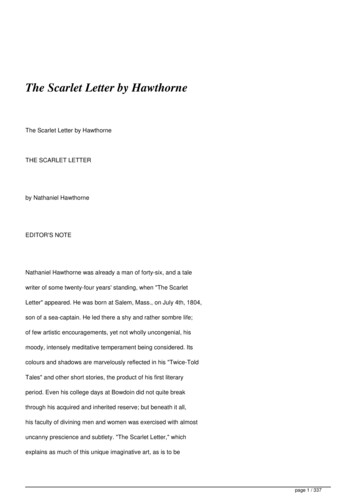
ACADEMY JOURNALFigure 4: Public Atriumdisorders need shielding from overstimulationbut simultaneously need to visually scan allthat the environment may pose for them.Lack of spatial clarity stresses both patientpopulations for different reasons: neurologicalpatients are easily distracted because their focusis on the physical effort it takes to navigateeven simple environments, while psychiatricpatients are easily confused because their focusis on the mental effort it takes to navigateunfamiliar environments.And atriums can be either over stimulating orineffective for the distracted or confused neuropsychiatric patient population. To support theCentre for Brain Health’s patient population,the atrium was modified from a five-storyspace to step down as a two-story space overthe clinic waiting areas; patients don’t feeloverwhelmed and are still connected to thescientists on upper levels as the atrium steps upinto the research floors.Figure 5: Detweiller Gallery6 A I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A HFor any patient population connecting atriumscan be a social challenge; the complexities ofmixing clinics’ very ill patients and distractedfamilies with casual and carefree researchassistants who are likely to be young adults in
T-shirts or lab coats is a challenge made evengreater when aiming for an encounter betweenpatient and researcher. For the Centre for BrainHealth, Interior Architect Lynn Befu utilizedthe multi-stepped atrium as an opportunityto address the differing ambience of twodissimilar environments—lab versus exam,staff versus patient; she fashioned an interiorwith smooth “calming” materials for the clinicseen from the entry on the right, and textured“engaging” materials for the lab seen fromthe entry on the left. This right-side/left-sidetreatment subtly and respectfully references theneuro-psychiatric patients’ often right-brain,left-brain entanglement, in addition to cueingall who enter which zone is their destination.mental stress of way finding by reinforcing theexit as the same way you entered.All patient populations should be greeted withentry cues that identify discrete patient zonesfrom staff zones. The Centre for Brain Healthfurthers this concept with the previously notedgeometric rotation that allows for two separatebut integrated structural grids throughout bothsides of the clinic floor; one grid creates a“clinic core,” where patients receive care, whilethe other grid creates a “collaboration core,”where staff can gather in private. The cliniccore is rotated free of the research labs to fosterexam room efficiency, while the collaborationcore housing open staff workstations is aligneddirectly under the research labs to encouragevertical connectivity between clinicians andresearchers. Separating the staff workstationsin the “collaboration core” creates an “offstage” environment protecting the patient fromunintended research activities.Stopping & starting opportunities. Corridorscan be hazardous traffic zones for neuropsychiatric patients, some of whom travel atdifferent speeds while others are disturbed byperceived congestion. Programming a widerprimary corridor to include alcoves for eitherstaff touch-down zones, patient sub-waitingareas, or simple benches for anyone allow thetired patient to rest or the overstimulated patientto take a break; the Parkinson’s patient will useany sort of visual cue from a mark on the floorto a small waiting nook to pace himself, theMultiple Sclerosis patient will use that nook asa place to rest, and the psychiatric patient willtake advantage of a brief moment of “escape”as he or she pulls away from the traffic.Short and simple corridors. Racetrackcorridors that loop back create pathways thatare disorienting and often longer than theneuro-psychiatric population can tolerate.Ideally, clinics should be compressed to onlypatient-destination rooms located off of one,short corridor; from this primary corridorpatients then need only turn left or right toaccess exam and treatment rooms. The simple“left or right” decision point eases mentalstress, and the shorter path acknowledgespatients who have difficulty walkingany distance.All patient populationsshould be greeted withentry cues that identifydiscrete patient zonesfrom staff zones.The Centre for Brain Health’s clinic coreachieves all of these attributes to support theirparticular patient population, which in turnGrouping the primary patient destination spaces sends the message that they are cared for; theninto a compact “clinic core” sets up threeand only then will the patient be receptive totherapeutic needs important to the neurological considering participation in neuro-psychiatricand psychiatric patient population:research. Cynader’s objective to have 100%patient participation in research is a highlySingle point of entry and exit. Multipleoptimistic but potentially attainable vision; as aentries can be extremely taxing for patientsbenchmark, patient participation in research haswith limited physical and/or mental resources.been known to range from as low as 2 percentA typical clinic floor arrangement laid out inbased on a 2007 study of U.S. cancer clinicala large “U” configuration where patients entertrials, to as high as 67 percent accordingon one end and exit on another end can createto a 2007 study of Canadians volunteeringa potential obstacle for confusion as well as afor randomized, controlled trials (1) (2).longer path for both patient and staff. Creating Participation in research is always a patienta clinic entry that is also the clinic exit eases the dilemma. For the neurological patient, he orA I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A H 7
ACADEMY JOURNALFigure 6: Staff-OnlyCollaboration Coreshe may feel “untreated” in a controlled study,and donating brain tissue post-mortem requiressensitive ethical considerations; clinicaltrials for cancer patients carry similar risksas there is always a chance a new treatmentmay be ineffective or worse than their currenttreatment. Architecturally, for patients ofany clinical diagnosis, the environment mustfirst meet the specific needs of that patientpopulation; a supportive setting allows themto consider these dilemmas and prepares themto participate in research fully motivated andcommitted to a helping find a cure.Transparency, either through the use of interiorglazing or open visual sightlines, furthers thedesign goal of allowing the scientist to be seenand the patient to view research in action, but asan interior motif transparency is a fundamentalelement ensuring a positive patient experiencein translational medicine facilities.Sustaining EnvironmentsFor a neuroscience facility, utilizingtransparency to experience a two-wayconnection is symbolic of the healthy brain’sfunctioning where synapses connect right-brainthoughts to left-brain actions. The Centre forBrain Health was inspired by the idea of anBeyond meeting the patient’s particularintact brain synapse: “There is a therapeuticphysical and emotional needs, translationalgain when there is a sense [that patients] aremedicine facilities must also seek ways tooffer patients a “preview” of spaces they might part of something bigger than themselves The whole point was to institute a dynamicencounter, thus allowing them an opportunitywhere more academic researchers, whoto anticipate what is ahead. Providing interiorwindows or glazed panes into spaces wherever typically have little interaction with patients,appropriate eases the unknown for patients and are put into direct contact with doctors andfamilies, and in some instances, simultaneously patients,” says Martin.allows the staff to monitor patient needs.8 A I A A C A D E M Y O F A R C H I T E C T U R E F O R H E A LT H W W W. A I A . O R G / A A H
And with both interior and exteriortransparency, the potential for heat buildup canbe extreme. The Centre’s large glass atriumwas the focus of energy-saving strategies.Mandated to construct the building to LEEDGold standards, heat recovery in the atriumwas maximized by running exhaust air througha manifold and reusing the heat to pre-temperincoming air. While the exhaust requirementsof the research areas ruled out a naturalventilation strategy, separate zone systems foreach area to maximize energy savings werecreated. “Some research areas need 10 to 12air changes an hour, but the patient areas havea much lower draw, around four air changesan hour,” Martin says. “Only 60 percent ofthe building needs to be at a higher rate, sothe building systems were designed for thepopulations within them, rather than the lowestcommon denominator.”The upper-level lab floors are full-height glasswalls incorporating insulated clear glass panelswith interior materials that are highly visibleabove the tree line, and when illuminated inthe early evening, highlight the translationalresearch mission of the Centre. In keeping withthe campus’ broader goals for environmentalsustainability, the lab design incorporates solarshading. Extensive high-performance glazing“puts science on display” to patients andpublic, while light-colored block walls encloseclinical areas to maintain patient privacy; bothtreatments offer a continual balance of patientneeds, transparency between science and care,and sustainability of resources.With or without the clinical componentcommon to translational medicine, labfacilities benefit society as a whole whenresources are conserved. Research labs’ energyconsumption per square foot exceeds hospitals’energy consumption by a factor of two; labsalso use disproportionate amounts of waterand have a substantial waste stream, some of ittoxic. With these concerns in mind, the Centrefor Brain Health also has reflective surfacesfor both roof and landscape, automatic lightingcontrols, and a gray water-harvesting system;the Centre will be 50 to 60 percent moreenergy efficient than a baseline building, andhalf of the savings will be achieved throughair-side heat recovery.In addition to architectural sustainability,carbon footprint reductions were alsoconsidered; the project was a collaborationbetween teams in two cities—San Franciscoand Vancouver—and the design took placein both cities simultaneously. From
The driving vision for this institution is Cynader's objective to have 100% patient participation in research. Three aspects aligned to support that vision and advance a new building typology: Translating Medicine, Motivating Patients, and Sustaining Environments. This paper addresses each aspect, as outlined below, with the belief