Transcription
European Review for Medical and Pharmacological Sciences2016; 20: 4930-4942Sleeve gastrectomy: have we finallyfound the holy grail of bariatric surgery?A review of the literatureI. KEHAGIAS¹, A. ZYGOMALAS¹, D. KARAVIAS¹, S. KARAMANAKOS²¹Department of General Surgery, Nutrition Support and Morbid Obesity Unit,University Hospital of Patras, Greece²Department of General Surgery, Basildon and Thurrock University Hospitals, Essex, UKAbstract. – OBJECTIVE: Laparoscopic sleevegastrectomy has become one of the most commonly performed bariatric operations. It is essentially a restrictive bariatric operation; however, a series of hormonal changes occurringpostoperatively contribute to decreased appetite and reduced food intake.PATIENTS AND METHODS: This is a literaturereview of recent articles published on Pubmed,Medline and Google Scholar databases in English.RESULTS: Although, laparoscopic sleeve gastrectomy is commonly performed worldwide,there is still a lack of standardization regardingthe surgical technique. Standardizing the surgical technique is essential in order to minimizepostoperative complications and offer patientsthe best long-term weight loss.CONCLUSIONS: Laparoscopic sleeve gastrectomy appears to be an effective bariatric operation. It is relatively easy to perform, well tolerated by the patients and very effective regarding long-term excessive weight loss and resolution of the comorbidities, with minimum nutritional deficiencies.Key WordsBariatric surgery, Sleeve gastrectomy, Laparoscopyic surgery, Morbid obesity, Gastric sleeve.IntroductionLaparoscopic sleeve gastrectomy (LSG) hasbecome one of the most commonly performedbariatric operations over the last years1. Withmore than 94.000 procedures performed in 2011,LSG has not only gained popularity, but also became the second most commonly bariatric operation performed after gastric bypass1. With morethan 1.9 billion overweight and over 600 millionobese people worldwide in 2014, obesity is right4930fully classified as a disease by WHO. Bariatricsurgery can effectively treat obesity and alsoimprove or even resolve a number of related comorbidities, offering patients a better life. Basedon recent studies, LSG is not only a safe, but alsoan effective bariatric procedure with long-lastingresults2. The aim of this report is to approach therole of sleeve gastrectomy as a contemporarybariatric procedure through a comprehensive andconcise review regarding various aspects of thispromising technique. Articles on sleeve gastrectomy, published on Pubmed, Medline and GoogleScholar databases in English were thoroughlyrevised and included in the discussion.Historical evolutionSleeve gastrectomy was first performed byHess in 1988 as part of his biliopancreatic diversion with the duodenal switch (BPD-DS) procedure, adapted from Scopinaro’s biliopancreatic diversion (BPD) and DeMeester’s duodenalswitch (DS) procedures3-5. Later in 1991 and1993 Marceau also proposed his modifications onScopinaro’s biliopancreatic diversion that effectively included early forms of sleeve gastrectomyvariations6,7. With the evolution of laparoscopicsurgery during the 1990s, Gagner performed essentially the first laparoscopic sleeve gastrectomyas part of BPD-DS in 19998. As a less demanding technique, sleeve gastrectomy quickly gainedpopularity early in the 21st century. Initially, itwas performed as a first step intervention forsuper-obese patients (BMI 60 kg/m2), beforedefinite intervention was undertaken with eithergastric bypass or biliopancreatic diversion procedures9,10. Nowadays laparoscopic sleeve gastrec-Corresponding Author: Ioannis Kehagias, MD, Ph.D; e-mail: ikehag@yahoo.gr
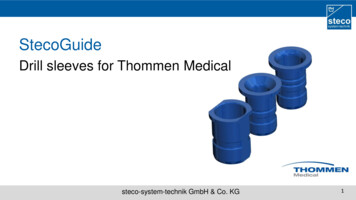
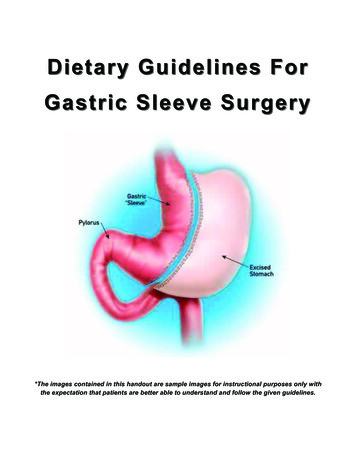
Sleeve gastrectomy, a reviewtomy (LSG) is considered a principal laparoscopic bariatric procedure, mainly due to the manyadvantages it possesses.Mechanisms of actionThe LSG is essentially a restrictive bariatricoperation. Weight loss is achieved by drasticallyreducing the gastric volume, which in turn leadsto reduced food intake. In addition, a series ofhormonal changes occurring postoperatively inbariatric patients, contribute to decreased appetite, reduced food intake and long-term weightloss (Figure 1)11, 12. Ghrelin, a hormone producedprimarily by the oxyntic cells of the fundus ofthe stomach during fasting, stimulates appetite byincreasing the expression of the orexigenic hypothalamic neuropeptide Y (NPY)11. By removingthe gastric fundus, patients undergoing sleevegastrectomy have markedly decreased levels ofghrelin and suppressed appetite respectively13.Peptide YY (PYY), a hormone produced postprandially from the gut, inhibits the release ofNPY and has an anorectic effect14. PYY is notably increased after sleeve gastrectomy, leadingto prolonged satiety and reduced food intake13.Glucagon-like peptide-1 (GLP-1) is secreted fromthe enteroendocrine L-cells in the intestine as aresponse to food indigestion. GLP-1 stimulatesinsulin release, inhibits glucagon secretion andhas a satiating effect. Both rapid gastric emptyingand postprandial hyperglucagonemia observedafter sleeve gastrectomy lead to increased GLP-1levels15, 16.Weight loss after LSGA major advantage of LSG is that despitebeing an easy, quick and safe bariatric procedure, it is also an effective surgical technique,Figure 1. Hormonal changes occurring postoperatively after LSG.offering patients considerable excess weight loss(%EWL)17-19. Boza et al20 reported, after 1000consecutive cases, that the %EWL at 1, 2 and 3years had been 86.6%, 84.1% and 84.5% respectively. Similarly, Rawlins et al21 found a %EWLof 86% at 5 years. In contrast to these verypromising results, most publications agree thatpatients undergoing LSG achieve a 60%EWL at5 years22-27. After an initial high %EWL, mostseries report some weight regain after the secondyear19. Respectively, Himpens et al25 and D’Hondtet al28 observed that patients regain weight after5 years, with the % EWL dropping below 60%.However, Sarela et al29 reported a %EWL of 69%at 9 years, the longest follow-up to date.Nutrient deficienciesIt is well documented that obese patients aregenerally malnourished, mainly due to a non-varied diet high in fats and carbohydrates and lowin quality protein products, dairy and vegetables.Most nutrient and micronutrient deficiencies persist postoperatively in patients undergoing bariatric surgery and as a result multivitamin supplementation is necessary for these patients30,31.However, nutritional deficiencies vary greatlybetween different bariatric operations, with LSGhaving only a minimal impact on the nutrientstatus22,32,33. Similarly to other types of bariatricprocedures, most commonly observed nutrientdeficiencies like iron, folate and thiamine persistpostoperatively, but can be easily resolved witha daily multivitamin supplementation22,32-35. Irondeficiency and anemia in particular, commonlyseen in bariatric patients, are also present afterLSG. However, the risk for anemia after LSG islower compared to the other type of procedures,when the iron supplement is administered postoperatively33,36. Vitamin D deficiency is commonamong obese patients due to malnutrition andlimited sun exposure. Postoperative hypovitaminosis D, however, is not common after LSGdue to loss of adipose tissue and adequate supplementation22,32. Respectively vitamin B12 deficiency is also not common after LSG as compared togastric bypass and BPD22,32,34,36,37. Vitamin B12 isabsorbed in the terminal ileum when banded tointrinsic factor, which is produced from the parietal cells in the antrum and duodenum. As compared to other malabsorptive bariatric operations,where the duodenum is bypassed, the uptake ofvitamin B12 is not disturbed in LSG32,36.4931
I. Kehagias, A. Zygomalas, D. Karavias, S. KaramanakosImprovement in metabolic changes(diabetes)Besides excess weight loss (%EWL), LSGhas a positive effect on diabetes. Several studies report that type 2 diabetes mellitus (T2DM)resolves in a significant percentage of patientsundergoing LSG19,38,39. Improvement and resolution rates as high as 86% of patients are reported,which are similar to those seen after RYGB andsuperior to LAGB22,40-44. Control of T2DM afterLSG is achieved, as in other bariatric operations, with the rapid excess weight loss. However,glycemic control without diabetic medication,normalization of hemoglobin A1c and improvement or even resolution of T2DM are seen earlyafter LSG45. A reason for the early improvementof T2DM after LSG is the notable low levels ofghrelin. Ghrelin not only suppresses appetite, butalso has a diabetogenic effect46. Also, Shah et al47documented that the faster gastric emptying andsmall bowel transit time observed after LSG havean additive effect on the control of T2DM.Improvement in systematic diseases(comorbidities)Apart from diabetes mellitus, LSG offers improvement and even resolution for a series ofcomorbidities48. Various studies report improvement or remission of hypertension, dyslipidemia,obstructive sleep apnea and degenerative jointdisease after LSG18,49. Weiner et al50 reported thathypertension either improved or resolved in 97%of the patients, whereas dyslipidemia improvedin 77% of the cases. Long-term results presented, show a resolution in hypertension in half ofthe patients undergoing LSG22, 23. Obstructivesleep apnea, commonly seen in morbidly obesepatients, can also be improved in 80% of patientsafter surgical intervention51.Improvement in quality of life (QoL)Laparoscopic SG results in considerable improvement in the quality of life (QoL) and psychosocial functioning52-55. First and foremost, LSG isa pill and food friendly bariatric operation. Pillsare generally well tolerated, as well as drugs likeaspirin and NSAIDS. In addition, food toleranceis very good, especially in the long-term55,56. Themajority of patients report high rates of satis4932faction postoperatively and a significant numberof them change their eating habits to a healthierdiet over time56. Furthermore, due to the quickrehabilitation and the adequate weight loss, physical activity, sexual life and self-esteem are alsoimproved postoperatively52. Additionally, in contrast to laparoscopic adjustable gastric banding(LAGB) procedure, which is also considered tobe safe and one of the least invasive bariatricoperations, no foreign bodies are used duringLSG57. As a result, long-term complications likegastric erosion and infections are not seen afterLSG57. However, the extended gastric resectionperformed during LSG has a significant impacton gastric acid secretion and motility. Many patients experience a series of gastrointestinal (GI)symptoms postprandial, like heartburn, epigastric pain, distress and dysphagia. Nevertheless,the impact of all these GI symptoms on QoL islimited58.How to SleeveSleeve gastrectomy (SG) is essentially a bariatric procedure consisting of a left partial gastrectomy of the fundus and the body in order tocreate a long, tubular formation along the lessercurvature of the stomach59. Although open SGhas been used for high-risk patients in the past,nowadays LSG is considered a primary bariatricprocedure60,61. Sleeve gastrectomy can be safelyperformed even with other minimally invasivesurgical techniques like single access surgery orrobotic surgery, with comparable results62-65. Thepreoperative management of the patients undergoing LSG does not differ from other laparoscopic bariatric procedures. Therefore, preoperativerisk assessment and evaluation to exclude othercauses of obesity should be performed in everypatient.To date there is a lack of standardizationregarding the surgical technique of LSG, whichmay affect the long-term outcome of the patients.However, in 2012 the first international expertpanel consensus statement regarding the “bestpractice guidelines” was published, based on theexperience of more than 12,000 cases of LSG61.The first step of LSG is the identification ofthe Crow’s foot, the pylorus and the antrum.Following this, a window in the greater omentumis made, laterally of the antrum66. Most expertsagree that it is important to mobilize the fundusbefore transection and to resect the short gastric
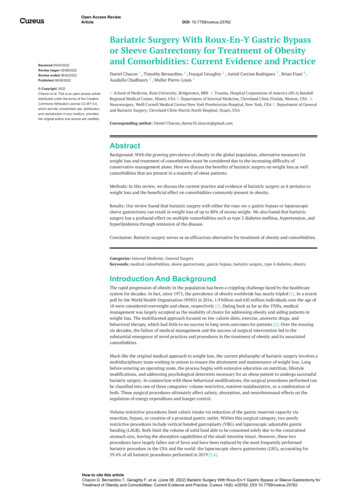
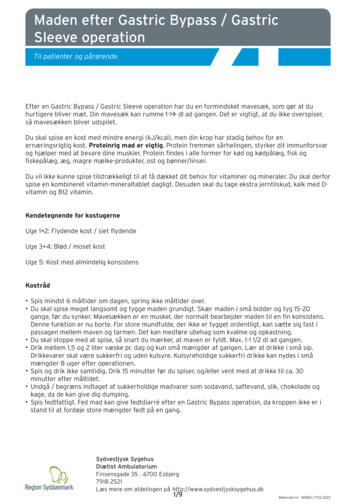
Sleeve gastrectomy, a reviewFigure 2. Surgical technique of LSG, showing how the sizeof the final gastric pouch changes in regard to the usage ofdifferent bougie sizes and different starting and ending transection points.vessels before stomach division. This will assistthe creation of a small gastric pouch and allowthe identification of any hiatal hernia61. If a hiatalhernia is present, it should be repaired at the sametime by posterior crural approximation19.One of the most controversial points in LSG isthe distance from the pylorus at which the gastricdivision should begin. The aim of the surgeon isto perform a restrictive bariatric operation, withimproved gastric emptying and decreased intraluminal pressure, in order to avoid a leak. The 2012expert panel agreed that the transection shouldbegin 2-6 cm from the pylorus61. Although mostauthors start the resection at these distances, thereare some that prefer the limits. Baltasar et al67 andMognol et al68 begin their resection at 2 cm fromthe pylorus in order to create a very small gastricpouch, since LSG is mainly a restrictive bariatricprocedure. Others, like Givon-Madhala et al69and Silecchia et al70 begin their division at 6-8cm from the pylorus, thus, preserving the gastricantrum and its contractile function. However, thebariatric surgeon should always consider the factthat a smaller gastric pouch with intact gastricantrum, leads to increased intraluminal pressuresand gastric emptying difficulties, that could placepatients at higher risk for leaks and proximal fistula formation at the gastroesophageal junction71.Furthermore, another controversy in LSG iswhere to end the gastric division. It seems thatmost experts agree on the importance to stayaway from the gastroesophageal junction duringthe last staple firing61. Soricelli et al73 tried to explain the vascular anatomy of this area, becauseone of the best supported theories of proximalfistula formation is the vascular-ischemic theory72. A “critical area” of vascularization is createdat the angle of His and the resection on that areacould lead to an ischemic gastric remnant, withan increased likelihood for a leak. Therefore, itis important to avoid resection too close to theesophagus and avoid creating a stenosis at thelevel of the angular incisure71.In order to maintain a standardized gastric volume and allow the reproducibility of the techniquebetween different bariatric surgical teams a bougieis used during the gastric division to facilitate theresection. However, the size of the bougie is notstandard and various sizes have been used fromdifferent bariatric surgeons. The bougie size ismeasured in French (Fr) where 1 Fr equals 0.33mm. This means that a 36 Fr bougie equals 1.2 cmand a 40 Fr equals to 1.3 cm. Most surgeons usea bougie between 32-40 Fr and, considering theabove, we can safely assume that they practicallyuse the same bougie size61,74. Small size bougieshave been associated with a higher incidence ofstaple line leaks, longer hospital stay, tendencytoward increased nausea, more emergency department visits, and readmissions74-77. Using biggerthan 40 Fr bougies, reduces the relative risk fora leak up to 66%74,75. As a matter of fact, biggerbougies result in larger gastric pouches and thismay affect the long-term weight loss. However,several studies have shown that using bougieslarger or equal to 40 Fr does not impact %EWL, atleast for the first three years postoperatively75,77,78.In addition, different surgeons resect the stomachat a different distance in respect to the bougie.Some prefer to be very close to the bougie, whileothers keep a small distance, in order to performa subsequent reinforcement of the staple line withinvaginating sutures72.The experts seem to agree that staple line reinforcement may reduce bleeding along the stapleline, although many authors do not routinely perform this reinforcement61, 79. Another reason forreinforcing the staple line is the control of postoperative leaks. Fistulas on the staple line may be ofmechanical-tissular cause, when the intraluminalpressure exceeds the staple line strength, or ofischemic cause, as proposed in the vascular-ischemic theory. Ischemic leaks typically occur onthe fifth or sixth postoperative day, during theinflammatory-proliferation phase of wound healing. Respectively, if the cause is mechanical-tis4933
I. Kehagias, A. Zygomalas, D. Karavias, S. Karamanakossular, leaks present early on the first two postoperative days80. Based on this fact, some surgeonshave adapted their technique, in order to reducethe risk of a mechanical failure of the staplingline. A number of different reinforcing materialshave been introduced and many studies have triedto provide evidence for their use81-84. Yet, stapleline invagination with a simple running sero-serous suture, with or without the addition of anomental patch, could efficiently control bleedingand attempt to reduce postoperative leaks withoutincreasing the cost67,72,85. Choi et al86 and Glaysheret al87 have published important meta-analysesand review studies in order to answer the criticalquestion of staple line reinforcement. However,while current evidence suggests that staple-linereinforcement may reduce the incidence of postoperative leaks and other associated complications, it does not significantly reduce bleedingcomplications and cannot be recommended as astandard technique61,86.In order to identify potential leaks or defectsites of the staple line, many surgeons test theintegrity of the newly-formed gastric pouch byintroducing air or methylene blue at the end of theoperation. Nevertheless, a negative test does notexclude a postoperative leak and many authorsdo not perform these tests at all88,89. A simplertest to discover a potential staple line defect isto inflate the resected stomach with air using aregular syringe89.Some authors have proposed that the measurement of the resected gastric volume at the endof the procedure can safely predict the overall%EWL. A resected gastric volume of more than500-1100 ml has been associated with %EWLof 50%50,90. However, the resected gastric volume is greater in patients with high preoperativeBMI91. Finally, it is important to send for routinehistological examination all gastric specimens.In about 8% of the cases unanticipated findingswarranting further clinical follow-up may be revealed, like H. pylori gastritis, autoimmune gastritis with a microcarcinoid formation, intestinalmetaplasia or even neoplasia92.Indications and contraindicationsLaparoscopic SG should be considered a primary bariatric procedure or the first stage of a2-step approach for the management of morbidlyobese patients18,59,61,93. In the later, LSG has beenused to treat initially super obese or high-risk pa4934tients, before a prospective second-stage bariatricprocedure (mainly RYGB) is performed, withintwo years18.It is important that all patients undergo comprehensive interdisciplinary assessment by a teamof specialists experienced in obesity management and bariatric surgery. Sleeve gastrectomycandidates should undergo routine preoperativeassessment, like any other major abdominal surgery. Laparoscopic SG adheres to the indicationsand guidelines of all other bariatric procedures94.Therefore, it should be offered to morbidly obesepatients with metabolic syndrome and to patientswith a BMI of 35 kg/m2 and associated co-morbidities61,94.Super obese patients, with BMI 50 kg/m2,can be offered LSG as this procedure seems to bealso effective for this group of patients95-97. However, super obese patients tend to regain weightafter the first 12 months of follow-up, while maintaining the improvement in co-morbidities98,99.Considering the above some authors believe thatLSG should be the first step of a 2-step procedurefor the management of super obese patients9,61.Laparoscopic SG seems to be a feasible andsafe procedure for high-risk surgical patients. Itcan be used as a safe first surgical procedure inorder to achieve rapid weight loss in high-risk patients who need to undergo a second non-bariatricprocedure such as knee replacement, nephrectomy or spine surgery100. Chaudhry et al101 andTariq et al102 have also published promising dataregarding morbidly obese patients with end-stageorgan failure who successfully underwent LSG.Laparoscopic SG has proved to be technicallyfeasible and effective in obese patients awaitingkidney transplantation, for adequate pre-transplantation weight loss, thus improving their access to transplantation103. Sleeve gastrectomy canbe also used as a post-transplantation bariatricprocedure in kidney recipients, because by retaining the intestinal continuity the uptake of immunosuppressants is not disturbed104. Obese compensated cirrhotic patients can also tolerate LSGwell. Laparoscopic SG can be safely performed incirrhotic patients, with low risk for postoperativecomplications, improving their metabolic syndrome and reducing hepatic steatosis105,106.Inflammatory bowel disease (IBD) is considered a contraindication for bariatric surgery.However, in a study from Steed et al107 morethan 18% of IBD population found to be obese.Furthermore, overexpessed obesity-related cytokines play a significant role in the development
Sleeve gastrectomy, a reviewof IBD108. Laparoscopic SG found to be safe andeffective for the management of obese patientswith IBD78,109,110.Regarding the age of the patients LSG there aremany studies that have published positive resultsfor pediatric, adolescent and geriatric patients whounderwent LSG. Alqahtani et al111 reported theirexperience with LSG in children and adolescents(5-21 years of age) with a follow-up of 24 monthswith very promising results. They reported noserious postoperative complications, resolution ofco-morbidities and acceptable %EWL. However,it is impossible at this time to estimate the overalllong-term consequences. Therefore, these patientsshould be managed in bariatric centers of excellence that offer all available surgical options and astrict long-term follow-up112.Morbid obesity in elderly patients is a substantial health problem. Perioperative managementof medical complications is crucial. Qin et al113in their recent multi-institutional study showedthat LSG may be a preferable option for elderlypatients. Furthermore, LSG can be safely performed in elderly patients, with low long-termreoperation and readmission risk. The perioperative risk of LSG in this patient population ispredominantly associated with the anticipatedmorbidity of advanced age113. Other studies havealso confirmed the safety and effectiveness ofLSG in the geriatric population114-116.Other indications may include cases that thesmall bowel is inaccessible due to adhesions fromprior operations and patients in whom repeatedendoscopy of the duodenum is necessary110.The only absolute contraindication for performing LSG is Barrett’s esophagus. The progression from erosive reflux disease to Barrett’sesophagus and gastric and esophageal cancer iswell established19, 61. Yet, the preoperative presence of gastroesophageal reflux disease (GERD)is only a relative contraindication, mainly dueto the fact that reflux symptoms may worsenafter LSG22, 28, 61. The long-term effect of LSGin GERD is controversial. Chiu et al117 in theirsystematic review concluded that there is notenough evidence to consolidate to a consensusregarding the effects of LSG on GERD. From thestudies they reviewed, some showed an increasein the incidence of GERD, while other reporteda decrease. Himpens et al28 reported a biphasicpattern of GERD after LSG. Reflux symptomsinitially present in the first postoperative year,they gradually improve and reappear after thesixth year postoperatively.Complications and theirmanagementLaparoscopic sleeve gastrectomy has beenconsidered to be a technically simple bariatricprocedure with acceptable weight loss, resolutionof comorbidities and low postoperative complications. Compared to laparoscopic gastric bypassand biliopancreatic diversion, LSG is easier toperform and thus involves less risk. However, itscomplications can be more severe than those ofother bariatric surgical techniques72. The complication rates after LSG vary among studies from0% to 18%, with a 30-day postoperative mortalityranging from 0%-0.4%118-120. The postoperativecomplications can be distinguished in early andlate.Early complications generally involve bleeding, gastric leak, obstruction, abscess formation,wound infection as well as all the other possiblepostoperative complications of major laparoscopic surgical procedures27. Late complications specific to LSG are the development of a fistula,GERD, stenosis, neofundus, spiral sleeve andintathoracic sleeve migration, weight loss failureand nutritional deficits37,72.The most common and major early complication is certainly the postoperative bleeding whichcan occur in up to 16% of patients with a reportedaverage of 3.6%120-122. Usually, it occurs duringthe first or second postoperative day and generally originates from the stapling line or the dividedgastroepiploic vessels. Other sources of bleedinginclude trocar site, splenic injury or liver laceration119. Intraluminal bleeding has been reportedto occur in 2% of cases19. Reinforcing the stapleline seems to be associated with a decreased riskof staple line hemorrhage86,123. In addition, in arecent randomized trial, Sroka et al124 proposedroutine elevation of the systolic blood pressure to140mmHg before termination of the procedurein order to identify possible bleeding sites. Thetreatment can be conservative, with blood transfusion and patient resuscitation, but there arecases for which reoperation is necessary for thedefinite control of the bleeding119.The gastric leak is a serious complicationof LSG with an incidence ranging from 0% to3.7%61,72,77. Proximal staple line leaks are morecommon than distal ones59. The basic conceptis that a leak happens when the intraluminal pressure exceeds the staple line or tissularstrength125. This situation usually occurs whenlocal factors like poor blood supply, stapling4935
I. Kehagias, A. Zygomalas, D. Karavias, S. Karamanakosissues or infection acutely impair the gastricwall healing72. In order to avoid leaks, tissuesshould be handled carefully and devices likestaples, electrocautery or other surgical equipment should be used rationally72,126. A numberof studies investigated the use of staple linereinforcing materials81-84. Recent studies suggestthat staple-line reinforcement may reduce the incidence of postoperative leaks86,87. Nevertheless,a running sero-serous suture that invaginatesthe staple line from the angle of Hiss to themidpoint of the transection, and a second continuous suture from this point to the end, withor without an omental patch may be adequate inorder to reduce leak rate67,72,85. During stappling,it is also very important to compress the gastrictissue carefully for a prolonged time (e.g. 30 sec)before firing in order to reduce tissue edema127.Additionally, a nasogastric tube can be left inthe newly-formed gastric pouch for 24 hours toreduce intraluminal gastric pressure128.Many authors routinely perform upper gastrointestinal swallow studies postoperatively inorder to evaluate the presence of an early leak,between the first and third postoperative day.However, the sensitivity of these studies is lowand a negative test does not exclude the presence of a leak126,128-130. Although gastric leakscan be accurately diagnosed with computed tomography, CT scans should only be performedwhen the clinical suspicion is high and not forscreening129,130. If a leak occurs, the managementis crucial for the outcome. The clinical presentation can vary greatly between patients andwhile most patients are completely asymptomatic, complications like peritonitis, septic shock,multi organ failure and death have been reported.Burgos et al126 observed that tachycardia canbe the initial sign of a leak. Patients with hemodynamic instability or those who cannot becontrolled using conservative measures requireintervention. Postoperative leaks can be categorized into acute (within 7 days), early (within 1-6weeks), late (after 6 weeks) and chronic (after 12weeks) in regard to the time of presentation61.An acute fistula can be repaired surgically if thedefect can be identified126. However, primaryrepair of a fistula is associated with high ratesof recurrence. In late fistulas simple primaryrepair of the defect is not possible due to chronic inflammation and concomitant presence ofan abscess128. Stable patients can benefit fromconservative treatment, like nothing by mouth,intravenous antibiotics and total parental nutri4936tion with or without CT-guided percutaneousdrainage of the abscess131. Endoscopic stentingafter percutaneous drainage of an abscess is avalid treatment option for a proximal leak61,128,131.The endoscopic use of fibrin glues, plugs or clipshas also been reported, although their efficacyis not proven72,131. The surgeon should wait forat least 12 weeks with conservative therapy before considering a reoperation to address a leak.Revision of the procedure and conversion toanother operation are possible options61. In thecase of a re-intervention, conversion to gastricbypass, Roux-en-Y, or total gastrectomy can beperformed61,132,133.The development of GERD or the worseningof reflux symptoms has been reported by someauthors as a late complication of LSG. Kehagiaset al22 and Himpens et al28 reported a peak ofGERD symptoms in the first year which declined during the first triennium. Himpens et al28observed a second peak after the sixth year28.The intact pylorus, the removal of the antrum,the severely restricted gastric capacity and thedisrupted motility could create stasis and induceor exacerbate reflux symptoms119. When the resection is not close e
Bariatric surgery, Sleeve gastrectomy, Laparoscopy - ic surgery, Morbid obesity, Gastric sleeve. Introduction Laparoscopic sleeve gastrectomy (LSG) has become one of the most commonly performed bariatric operations over the last years1. With more than 94.000 procedures performed in 2011, LSG has not only gained popularity, but also be-