Transcription
Th e Ro le o f th e Ac u te Ca reNu rs e P ra c titio n e r:Ne w Mo d e ls fo r Ac u te Ca reDe live ry in a n Ac a d e m icMe d ic a l Ce n te rMa rc h 22, 2012Ba rb a ra Ca s h a ve lly MS , RN, AOCNMa ria Win n e MS , RN, NE-BCMa s s a c h u s e tts Ge n e ra l Ho s p ita l
Ob je c tive s Identify current events that expandedopportunities for nurse practitioners to practicein acute care settings Describe two acute care nurse practitioner(ACNP) models
In s titu te o f Me d ic in e (IOM) Fu tu re o fNu rs in g Re c o m m e n d a tio n s Advanced Practice Nursesshould be able to practice tothe full extent of theireducation Expand opportunities fornurses to lead and managecollaborative efforts withphysicians and others toredesign and improve practiceenvironments and healthsystems.In s titu te o f Me d ic in e (IOM), 2011
Exp a n d in gOp p o rtu n itie s WHY? Acute Care Nurse Practitioners (ACNPs) play significantrole toward improving quality and enhancing efficiency. Surge in acuity levels of hospitalized patients leading toadvanced practitioners managing complex patients Regulations set forth by Accreditation Council forGraduate Medical Education (ACGME) Restricted residents to work an average of only80hours/week Challenges of decreasing LOS
We a re th e Fu tu re o f Nu rs in g Nu rs e le a d e rs a t MGH to o k le a d in g ro le s in d e s ig na n d c re a tio n o f 2 c o lla b o ra tive in p a tie n t ACNP h e a lthc a re m o d e ls : The Academic Hospitalist Service The Oncology Inpatient Nurse Practitioner Service
Ba c kg ro u n d De ve lo p m e n t a n d Im p le m e n ta tio n o f th e s e twom o d e ls a re a lig n e d with th e re c o m m e n d a tio n s p u tfo rth b y IOM “Th e Fu tu re o f Nu rs in g : Le a d in gCh a n g e , Ad va n c in g He a lth ” Th e two ACNP c a re d e live ry m o d e ls a ls o a lig n withth e AONE Gu id in g P rin c ip le s a d d re s s in g :“The Role of the Nurs e in Future P a tie nt Ca reDe live ry” http://www.aone.org/resources/PDFs/AONE GP Future Patient Care Delivery 2010.pdf
Ba c kg ro u n dWh a t is in th e lite ra tu re ? Two c o m m o n th e m e s a b o u t ACNP s– continuity of ca re– easy a cce s s ibility of ACNPs to the staffnurses due their constant presence on theunits.
Ba c kg ro u n dLite ra tu re c o n t’d Im p ro ve d e ffic ie n c y a n d q u a lity o f c a rewh e n ACNP s a t UCS F a d m itte d a n dm a n a g e d a n a c u te m e d ic a l p o p u la tio np re vio u s ly c a re d fo r b y h o u s e s ta ff– Positively impacted quality of care due tocontinuity of care and availability of NPsthroughout the day to interact with patients,families and nursing staffHowie & Erickson, 2002
Ba c kg ro u n dLite ra tu re c o n t’d ACNPs improved patient flow and continuity ofcare to pediatric ICU patients and familiesBrown et al, 2008
Ba c kg ro u n dLite ra tu re c o n t’d n 145 Integrating NPs in ICU setting positively impactedpatient care by enhancing workflow Having more time to discuss patient care issues w/nurses and interact more with patients' families thanphysician colleaguesKleinpell et al, 2008
Ac a d e m ic Ho s p ita lis t S e rvic e(AHS ) Spring of 2010, department of medicine incollaboration with medical nursing servicedeveloped a new model of care called theAcademic Hospitalist Service (AHS) Goal: expedite admissions of acutely ill medicalpatients from our ED Collaborative Care Team – hospitalists, ACNPs,medical students
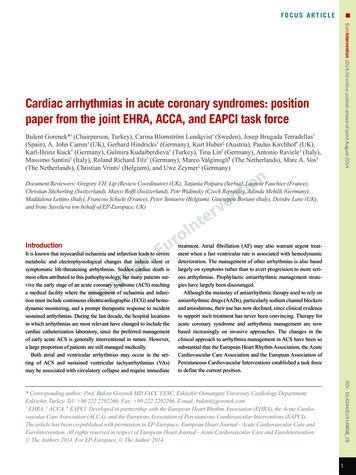
AHS ModelHospitalistMedical DirectorACNPNursing Director2 Sub-InternsMedical/Progressive CareUnitGeneral MedicalUnitBed #1Bed #2Bed #3Bed #4Bed #9Bed #10Bed #5Bed #6Bed #7Bed #8Bed #12Bed #13Bed #11Figure 1. AHS Model
Ac a d e m ic Ho s p ita lis t S e rvic eCa re De live ry Te a m7am-7pm: one hospitalist one ACNP, two 4th yearsub-interns. The physician andACNP care for 13patients7pm-7am: one hospitalist for 13patients
Ac a d e m ic Ho s p ita lis t S e rvic eQ: Wh a t a re th e d e s ire d e xp e rie n c e s a n dq u a litie s re q u ire d b y th e ro le o f th eACNP s ?A: NP s s h o u ld h a ve : experience caring for acutely ill patientson a general medical inpatient unit or inan ICU pioneering mindset be flexible, adapt well to change and beproactive in the ongoing development of anewly formed service.
Ac a d e m ic Ho s p ita lis t S e rvic e By May 2010, 2.5 part-time acute care nursepractitioners were hired (two 36 hrs/wk, one24hrs/wk) Two NPs were novice to the advanced practicerole– Both were experienced medical ICU nurses One NP had several years NP experience in asimilar model and worked as a staff nurse at ourinstitution.
Ac a d e m ic Ho s p ita lis t S e rvic eACNP Orie n ta tio nEssential ElementsClinical education, socialization, networking andmentorshipAchieved by .
Ac a d e m ic Ho s p ita lis t S e rvic eACNP Orie n ta tio n A 4-week orientation for the two novice ACNPs and a 3week orientation for the experienced ACNP. S h a d o w d a ys with experienced ACNPs and physicianswithin the medical, oncology and cardiac services –learned organizational culture, informatics, consultationprocess, clinical assessment, care management as wellas role development
Ac a d e m ic Ho s p ita lis t S e rvic eACNP Orie n ta tio n c o n t’dS h a d o w Da ys with AHS Hospitalists Each ACNP worked with the AHSHospitalists for 4-7 days prior tohaving full responsibility for patientcare The ACNPs were able to cocoordinate plans of care with AHSHospitalists, an experience which wasdescribed as an invaluable part of theorientation
Ac a d e m ic Ho s p ita lis t S e rvic eACNP Orie n ta tio n c o n t’d Clinical Simulations– 4 hour clinical simulation program– Developed by the nursing simulation staff inthe Norman Knight Center for Clinical &Professional Development and the ClinicalDirectors of the NP teams– 4 scenarios: pulmonary embolism, urosepsis,gastrointestinal bleed and hypercalcemia
Ac a d e m ic Ho s p ita lis t S e rvic eS ta ffin g ACNP is scheduled to work 7am-7pm sevendays/week ACNPs rotate responsibility in devising their 8 weekschedulesRe p o rtin g S tru c tu re : ACNPs report operationally to the nursing director A medical director serves as their supervisoryphysician ACNP is the responding clinician (works in lieu of anintern)
Ac a d e m ic Ho s p ita lis t S e rvic eMu ltid is c ip lin a ry Co lla b o ra tio n Collaborates daily with multiple disciplinesnecessary to provide seamless care Participates in patient rounds along with staffnurses, attendings, case managers, physicaltherapist, nutritionist and social workers Provides more opportunities for timelydiscussion and resolution of patient care issuesand staff education
Ac a d e m ic Ho s p ita lis t S e rvic eMultidisciplinary Rounds
Ac a d e m ic Ho s p ita lis t S e rvic eCo n tin u in g Ed u c a tio n AHS Hospitalist is available to provide ACNPswith input, mentorship and assistance withemergencies Clinical simulations are offered every fewmonths – work in progress ACNP continuing education programs areoffered on a monthly basis
Ac a d e m ic Ho s p ita lis t S e rvic eSummary New service opened July 2010Comprised of 13 bedsAdmit house and private patientsED access unit7am-7pm Hospitalist, NP & 4th year sub interns 7pm - 7am a Hospitalist cares for all patients
Ac a d e m ic Ho s p ita lis t S e rvic eS u m m a ry c o n t’dACNP P ra c tic e Mo d e l ACNPs manage care of their patients incollaboration with the attendings ACNPs are the responding clinician (practicein lieu of residents)
Ac a d e m ic Ho s p ita lis t S e rvic eDa ta Co lle c te d Compared data between AHS and 2 othermedical teams that do not have an NP on theircare teams. LOS Pre-noon Discharges Readmission Rates
On c o lo g y In p a tie n t NP S e rvic e 2009 Cancer Center charged with developingan inpatient service in response to ACGMErequirements. Goal: provide inpatient coverage for 14 medicaloncology inpatient beds Cancer Center team in collaboration with theOncology Nursing service developed a newinpatient NP service
On c o lo g y In p a tie n t NP S e rvic eEva lu a te d 3 m o d e ls o f p ra c tic e : Hospitalist Model–Physician whose primary practiceis hospital medicine Moonlighter Model–Physician who has a primary joband works extra shifts as asecondary job Nurse Practitioner Model–Dedicated inpatient NP providinginpatient care.
On c o lo g y In p a tie n t NP S e rvic e Ad va n ta g e s o f a n In p a tie n t NP s e rvic e :Collaboration and continuity with oncologyAttendings and outpatient NP’sDedicated to an identified oncology unitPatient satisfactionQuality and safetyAbility to decrease LOSEnhancement of multidisciplinary practice
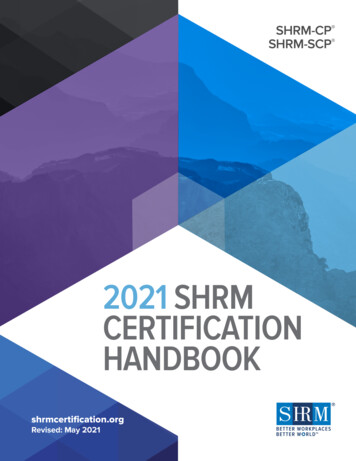
OINPS ModelClinical DirectorOINPS ModelNursing DirectorMedical/Surgical UnitMedical/Surgical UnitBed #1Bed #2Bed #3Bed #4Bed #5Bed #6Bed #7Bed #8Bed # 9Bed #10Bed #11Figure 2. OINPS ModelBed #12
On c o lo g y In p a tie n t NP S e rvic e P a tie n t P o p u la tio nSolid tumor, lymphoma and sarcoma patientsAdmitted for acute care symptoms or medicalmanagement related to disease progression,treatment or end of life.Required to have a stable cardiopulmonarystatus.Admitted from outpatient practices, oncologyinfusion unit, emergency department, home oroutside hospital
On c o lo g y In p a tie n t NP S e rvic eJ u n e 2010 14 medical oncology beds (2 units) 12 hour shifts, 24/7 service 9.5 FTE’s approved Staffing: 7a-7p two NPs 7p-7a one NP 3p-3a one NP
On c o lo g y In p a tie n t NP S e rvic eWo rke d c lo s e ly with HR Re c ru ite r Master’s degree in nursing NP certification, preparation in either adult,family or acute care educational track Oncology experience preferred Acute care inpatient experience required ACLS required
On c o lo g y In p a tie n t NP S e rvic eCh a ra c te ris tic s o f NP Ca n d id a te s Motivated Self-directed, ability to grow and developtheir role Flexible Ambitious Leadership skills Resilient, ability to adapt to change Collaborative team player
On c o lo g y In p a tie n t NP S e rvic e By Ap ril 2010, 9.5 fu ll-tim e a n d p a rt-tim e NP s we reh ire d 39 hr work week 36 hr work week 24 hr work week Dive rs e NP a n d n u rs in g e xp e rie n c e : Oncology, acute care medicine, emergency, neuroICU, primary care Experienced NPs Novice NP with solid nursing experience
On c o lo g y In p a tie n t NP S e rvic eOrie n ta tio n10-12 week orientation Developed in collaboration with Clinical Director andOncology Nursing Director of NP service Orientation started before service “went live” NP Credentialing Shadow experiences with OncologyAttendings, NPs and resident teams Operations of inpatient processes Educational Curriculum Simulation Lab Education of new service to Cancer CenterClinicians, DOM, Admitting, ED, other services.
On c o lo g y In p a tie n t NP S e rvic eOrie n ta tio nOrg a n iza tio n a l a n d Op e ra tio n a l P ro c e s s e s Admissions/Discharges Clinical Assessments Multidisciplinary Rounds Daily plan of care Daily documentation Order writing Consults Billing procedures
On c o lo g y In p a tie n t NP S e rvic eOrie n ta tio n De ve lo p m e n t a n d re c o g n itio n o fin p a tie n t NP Ro leImportant new member of the teamIntegrated into the unit and staffCollaborates with Multidisciplinary team:MD Attendings, Nurses, Case Managers,Social worker and other disciplines
On c o lo g y In p a tie n t NP S e rvic eOrie n ta tio nEd u c a tio n a l Cu rric u lu m , we e kly c la s s e s Infectious disease Renal disease Oncologic emergencies Chemotherapy overview Pulmonary diagnoses Cardiac diagnoses
On c o lo g y In p a tie n t NP S e rvic e On g o in g Ed u c a tio nClinical Director meets with NP team twice aweek to review patients or discuss specifictopicsDaily Multidisciplinary Rounds provideseducationSimulations every 4-6 monthsNP educational programs offered monthly
On c o lo g y In p a tie n t NP S e rvic e SummaryJune 2010, continues to evolveInitially 14 NP Beds, expanded to 28 BedsSeptember 20112 oncology units: Medical Oncology andBMT/LeukemiaCurrently 15.5 FTEs4 NPs 7a-7p, 1 NP 11a-11p
On c o lo g y NP Da ta Co lle c tio nCo m p a ris o n to Re s id e n t Te a m 3 LOS Readmission Rate
Nu rs e P ra c titio n e r S u rve y Informal Survey of AHS and Oncology NursePractitionersn 16 NPsDemographics 9.41 Years as a RN 5.22 Years as a NP 1.82 Years in current role
Nu rs e P ra c titio n e r S u rve yHo w s a tis fie d a re yo u with th e NP m o d e l inwh ic h yo u wo rk?Overall satisfaction was excellent (n 16) 0% very dissatisfied or dissatisfied 6% (1) somewhat dissatisfied 19% (3) somewhat satisfied 63% (10) satisfied 13% (2) very satisfied
Nu rs e P ra c titio n e r S u rve yWh a t a re yo u r fa vo rite a s p e c ts o f yo u r ro le ? The patients Autonomy Part of a strong team Continuity of care Critical thinking and decision making
Nu rs e P ra c titio n e r S u rve yFa vo rite As p e c ts o f th e ro le “Always connecting with patients and families. This is the nursingpart of nurse practitioner” “Love inpatient medicine, the autonomy and the varied clinicaldiagnoses we see” “Team atmosphere, direct patient interaction and care” “Constantly changing patients, medical conditions, working withother disciplines and learning how to care for new diagnoses” Collaboration between attendings & NPs – immediatecoverage/backup if patient decompensate
Nu rs e P ra c titio n e r S u rve yWh a t a re th e le a s t fa vo rite a s p e c ts o f yo u rro le ? Change in expectations Night shifts Numerous admissions and discharges Assignment load Sporadic education
Nu rs e P ra c titio n e r S u rve yLe a s t Fa vo rite As p e c ts o f th e ro le Limited coverage from other NPs for sickness andvacations due to the small size of our team Difficult to be part of hospital-wide committees due toour irregular schedule Challenge of caring for private patients only versuscaring for both house and private patients
Nu rs e P ra c titio n e r S u rve yP le a s e ra te yo u r s a tis fa c tio n with yo u rre la tio n s h ip s with s ta ff n u rs e s (ra tin g s c a le e xc e lle n t to p o o r)94% ACNPs rated relationships with staffnurses as good to excellent
S u m m a ry The opportunity to develop and implement 2ACNP models of care helped create and shapethe direction of innovative models of patientcare These models were intended to Improve patient satisfaction Positively impact the patients LOS Facilitate meeting ACGME requirements
S u m m a ry c o n t’d We are well aligned with the IOM report on theFuture of Nursing Two areas that this report focuses on include: How nurses can best contribute tohealthcare delivery Nurses should be full partners, withphysicians and other health professionals
We fe e l th a t we a re we ll o n o u r wa y tore a c h in g th o s e g o a ls
Re fe re n c e s IOM (Institute of Medicine). (2011). The future ofnurs ing: Le a ding cha nge , a dva ncing he a lth.Washington, DC: The National Academies Press. Howie JN, Erickson M. Acute care nurse practitioners:Creating and implementing a model of care for aninpatient general medical service. Am J Crit Ca re .2002;11(5):448-458.
Re fe re n c e s c o n t’d Brown A, Besunder J, Bachman M. Development of apediatric intensive care unit nurse practitioner program.J Nurs Admin. 2008;38(7/8):355-359. Kleinpell R, Ely W, Grabenkort R. Nurse practitionersand physician assistants in the intensive care unit: anevidence-based review. Crit Ca re Me d.2008;36(10):2888-2897.
Nurse Practitioner: New Models for Acute Care Delivery in an Academic Medical Center March 22, 2012 . when ACNPs at UCSF admitted and managed an acute medical population . - 4 hour clinical simulation program - Developed by the nursing simulation staff in