Transcription
The WHO Regional Office for EuropeThe World Health Organization (WHO) is aspecialized agency of the United Nations created in1948 with the primary responsibility for internationalhealth matters and public health. The WHO RegionalOffice for Europe is one of six regional officesthroughout the world, each with its own programmegeared to the particular health conditions of thecountries it serves.Member sBelgiumBosnia and yPolandPortugalRepublic of MoldovaRomaniaRussian FederationSan TajikistanThe former YugoslavRepublic of MacedoniaTurkeyTurkmenistanUkraineUnited KingdomUzbekistanFacilitating evidence-based practicein nursing and midwifery in theWHO European RegionWorld Health OrganizationRegional Office for EuropeUN City, Marmorvej 51,DK-2100 Copenhagen Ø, DenmarkTel.: 45 33 70 00Fax: 45 33 70 01Email: euwhocontact@who.intWebsite: www.euro.who.int
Facilitating evidence-based practicein nursing and midwifery inthe WHO European RegionBy: Virpi Jylhä, Ashlee Oikarainen,Marja-Leena Perälä & Arja Holopainen
Facilitating evidence-based practice in nursing and midwifery in the WHO European Region is a guide for Member States, supportedby the WHO Regional Office for Europe, to enable and enhance the contribution of nurses and midwives to promoting evidencebased practice and innovation in nursing and midwifery. It aims to promote a shared understanding of evidence-based practicein nursing and midwifery and strengthen its foundations in the Region to support health policy-makers, health-care professionalsand others in facilitating the culture of evidence-based practice in nursing and midwifery. The guide provides examples tosupport nurses and midwives in applying evidence-based practice in their clinical roles.KeywordsEUROPEHEALTH SERVICESMIDWIFERYNURSINGWORLD HEALTH ORGANIZATIONAddress requests about publications of the WHO Regional Office for Europe to:PublicationsWHO Regional Office for EuropeUN City, Marmorvej 51DK-2100 Copenhagen Ø, DenmarkAlternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the RegionalOffice website (http://www.euro.who.int/pubrequest). World Health Organization 2017All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to reproduce or translateits publications, in part or in full.The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever onthe part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning thedelimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the WorldHealth Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietaryproducts are distinguished by initial capital letters.All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, thepublished material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use ofthe material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The views expressedby authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the World Health Organization.Text editing: Alex Mathieson, United Kingdom (Scotland).Design: Damian Mullan, So it begins , United Kingdom (Scotland).
iiiCONTENTSAcknowledgementsAcronymsiviv1. Introduction2. Evidence-based health care and practiceEvidence-based health careEvidence-based practice3. Benefits of EBPBenefits for the general populationBenefits for nurses and midwivesBenefits for health-care systemsBenefits for research and education4. Implementing EBPin nursing and midwifery5. Sustaining an evidence-based culturein health careOrganizational context and cultureThe continuous development of EBP6. Success ncesAnnex 1. International collaborators293413
ivACKNOWLEDGEMENTSThis document was commissioned by the technical Programme on Human Resources forHealth, Division of Health Systems and Public Health, WHO Regional Office for Europe. Itaims to support health policy-makers, managers, educators and health-service providersto develop and promote a culture of evidence-based practice in nursing and midwifery,and to accelerate progress in the implementation of European strategic directions forstrengthening nursing and midwifery towards Health 2020 at national and regionallevels.The WHO Regional Office for Europe offers its thanks and appreciation to the WHOCollaborating Centre for Nursing at the Nursing Research Foundation in Finland and theauthors of this publication: Virpi Jylhä, Ashlee Oikarainen, Marja-Leena Perälä and ArjaHolopainen.WHO also acknowledges and appreciates the support of the WHO collaborating centresfor nursing and midwifery and the Joanna Briggs Institute’s collaborating centres inthe WHO European Region for providing valuable comments and case examples for thedocument.Technical guidance and coordination of this project was provided by Galina Perfilieva,Programme Manager, Human Resources for Health, Division of Health Systems andPublic Health, WHO Regional Office for Europe.ACRONYMSAMEEBPEBHCEIPJBIPACESAction Model of Expertiseevidence-based practiceevidence-based health careevidence-informed practiceThe Joanna Briggs InstitutePractical Application of Clinical Evidence System (audit tool)
INTRODUCTION1. INTRODUCTIONNurses and midwives play an important role in tackling the public health challengespresent in health systems across the WHO European Region. These groups of healthcare professionals collectively form the largest component of the health workforce (1), andare key actors in delivering effective, efficient, accessible, acceptable, patient-centred,equitable and safe health-care services (2). Quality health-care services require thatclinical decision-making in nursing and midwifery and care coordination are basedon evidence. The best available evidence should be utilized when improving aspects ofquality in health care and enhancing evidence-based practice (EBP). The nursing andmidwifery professions remain central to the achievement of EBP in health-care settings,particularly in standardizing and aligning health-care practices with evidence at thepoint of care (3–5).The purpose of this guide is to promote a shared understanding of EBP in nursing andmidwifery and strengthen its foundations in the WHO European Region. The documentaims to support health policy-makers, managers, health-care professionals and otherrelevant stakeholders in facilitating the culture of EBP in nursing and midwifery. Thiscan in turn promote the effectiveness of health-care services, contribute to the utilizationof evidence in clinical care and strengthen the nursing and midwifery knowledge base.Examples are provided throughout the text to highlight key elements of EBP as it relatesto nursing and midwifery.The guide sets out to clarify the concept of EBP, identify its benefits, describefundamental elements of implementation and sustaining an evidence-based culturein health care, and summarize success factors for implementation in nursing andmidwifery. It provides examples of how EBP can be facilitated at national, regional,organizational and work-unit levels. The sharing of knowledge on innovations, strategiesor interventions related to EBP among countries can promote and strengthen EBP andinnovation in nursing and midwifery across the Region. Member States should striveto enable nurses and midwives to apply EBP in their clinical roles to promote health andprevent disease while providing the best possible care to patients and populations basedon their needs (1).Nurses and midwives should understand the meaning of EBP and facilitating factors forsuccessful implementation (6). They should acknowledge the rationale for implementingEBP and strive to develop the skills to engage with evidence and apply it to daily nursingand midwifery practice (6). To provide evidence-based care for patients consistently, policymakers, managers, health-care professionals, educators and researchers must identifytheir roles and responsibilities in the process (1). Only when all accountable stakeholdersassume their responsibilities can the goal of EBP as a standard of care be achieved (1).1
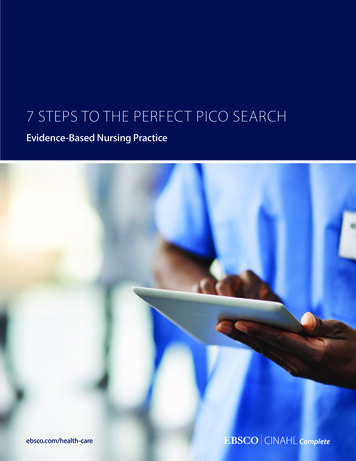
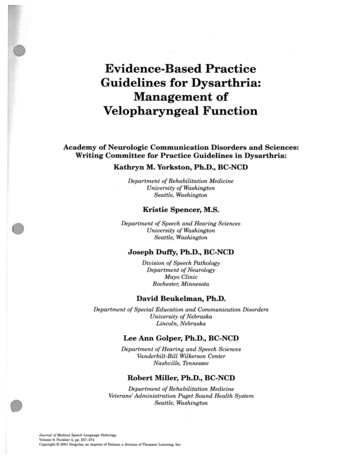
2FACILITATING EVIDENCE-BASED PRACTICE INNURSING AND MIDWIFERY IN THE WHO EUROPEAN REGION2. EVIDENCE-BASED HEALTH CARE AND PRACTICECore concepts related to EBP are often used interchangeably in health-care practiceand in the literature, stimulating the need for nurses and midwives to grasp a clearunderstanding of the concepts and recognize how they differ (6). This guide focuses on EBP,particularly on what it means to nursing and midwifery: it is nevertheless vital to promotea shared understanding of the broader concept of evidence-based health care (EBHC).Evidence-based health careEBHC is an umbrella concept of EBP that includes nursing, midwifery, medicine andallied health professions (7). It can be conceptualized as clinical decision-making thatconsiders the feasibility, appropriateness, meaningfulness and effectiveness of healthcare practices. This may be informed by the best available evidence, the context in whichcare is delivered, the individual patient, and the professional judgement and expertise ofthe health professional (8). To facilitate evidence-based decision-making, all professionsin health care are to be given the opportunity to be involved in developing EBP andembedding evidence into professional practice and education (7).The Joanna Briggs Institute (JBI), an international nursing research organization, hasdeveloped the JBI model of EBHC. This conceptualizes: the steps of the process to achievean evidence-based approach to clinical decision-making; how the component parts ofthe model are operationalized; and how they might be implemented in practice (8,9).EBHC is not a clean, linear process; at times, the process can be bi-directional, which isrepresented in Fig. 1 by the smaller arrows that indicate the feedback cycle.Fig. 1.JBI model of EBHCGlobal healthEvidenceimplementationEvidencebased health transferOverarching principlesCulture – Capacity – Communications – CollaborationSource: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.EvidencegenerationEvidencesynthesis
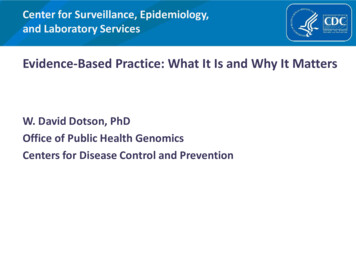
3EVIDENCE-BASED HEALTH CARE AND PRACTICEThe core phases of the JBI model of EBHC aredefined as evidence generation, evidencesynthesis, evidence transfer and evidenceutilization. Evidence generation (Fig. 3)includes discourse, professional expertiseand research (8). Research evidence isgenerated through original studies (primaryresearch) and systematic reviews (secondaryresearch). In this phase, systematicreviews might identify important gaps inresearch evidence. The gold standard ofevidence is recognized by many as being therandomized controlled trial, but other typeshave become increasingly significant ininforming nursing and midwifery practice.Research evidence does not always exist:nurses and midwives must make decisionsin care situations based on the best evidenceavailable at any particular time. It istherefore fundamental to recognize whatspecific evidence is required to answer aclinical question and identify which type ofevidence is available (research, experience ordiscourse) during the synthesis of generatedevidence (8).Current available evidence needs to besynthesized. Evidence synthesis is definedas: “the evaluation or analysis of researchSource: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.Evidencebased health careFeasibleAppropriateMeaningfulEffectiveFig. 3.Evidence generationGlobal healthSource: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.The feasibility, appropriateness,meaningfulness and effectiveness ofvarious treatment options or health-carepractices are to be considered in evidencebased decision-making (8). Global healthis the ultimate goal and endpoint of thecomponents of the model (8,9), whichincludes striving for a sustainable impact inchanges to health-care practices, increasedengagement and close multisectoralcollaboration, and assessment of localcommunities’ knowledge requirements (8).Fig. 2.The Pebble of KnowledgeFig. 4.Evidence synthesisEvidencesynthesisSource: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.The central component of the model isthe so-called Pebble of Knowledge (Fig. 2),with the core phases defined as evidencegeneration (Fig. 3), evidence synthesis (Fig.4), evidence transfer (Fig. 5) and evidenceimplementation (Fig. 6).
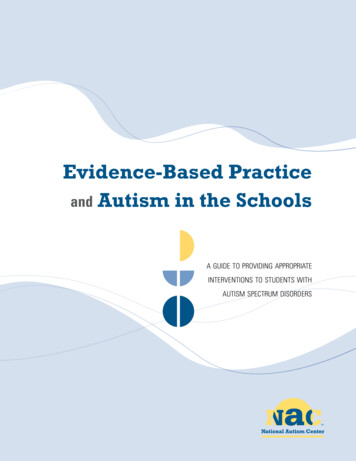
4FACILITATING EVIDENCE-BASED PRACTICE INNURSING AND MIDWIFERY IN THE WHO EUROPEAN REGIONevidence and opinion on a specific topic to aid in decision making in healthcare” (9).The three main pragmatic components of evidence synthesis include systematic reviews,evidence summaries and clinical guidelines (Fig. 4 and Infobox 1).Infobox 1. Components of evidence synthesisA systematic review is: “ essentially an analysis of all of the available literature (i.e. evidence) and ajudgement of the effectiveness or otherwise of a practice ” (9).An evidence summary is: an efficient approach to synthesize an overview of the available evidence in atimely fashion (8,10).A clinical guideline is: “statements that include recommendations intended to optimize patient carethat are informed by a systematic review of evidence and an assessment of the benefits and harms ofalternative care options” (11).Example 1. Cochrane Special Collection of Systematic ReviewsThe special collection brings together high-quality systematic reviews on breastfeeding tosupport the implementation of evidence into policy and practice. The purpose of the collectionis to promote effective breastfeeding for mothers and babies through the collection of the bestavailable evidence for use by decision-makers, health professionals, advocacy groups, and womenand families (12).Example 2. WHO guidelines to improve quality of antenatal careThis WHO guideline (13) includes comprehensive recommendations to reduce the risk of stillbirthsand pregnancy complications and aims to give women a positive pregnancy experience. Itincludes recommendations for health-system interventions to improve the quality of antenatalcare. The implementation of guideline recommendations can save lives, as antenatal care offersthe potential to make a positive contribution to health promotion, screening and diagnosis, anddisease prevention. The recommendations, which include evidence on harms and benefits, values,resources, equity, acceptability and feasibility, are based on different sources of evidence, such aseffectiveness reviews, qualitative evidence syntheses, test-accuracy reviews and mixed-methodreviews, that have been assessed and synthesized.Synthesized evidence (Fig. 5) must be transferred and shared to be implemented inpractice. Jordan et al. (8) clarify “transfer” as meaning “a coactive, participatory processto advance access to and uptake of evidence in local contexts”. Transfer enables uptakeof evidence and so enables, facilitates and supports evidence implementation. Essentialcomponents of evidence transfer include active dissemination, systems integrationand education. The JBI model highlights the importance of dissemination of evidenceusing active methods and human communication to spread information in a formatthat encourages utilization. Education programmes, include continuing professionaldevelopment or broader programmes, are recognized as an effective means of evidencetransfer. Embedding evidence into the system, policies and procedures is necessary fordecisions at all levels of organizations to be guided by evidence.
EVIDENCE-BASED HEALTH CARE AND PRACTICEEvidence implementation (Fig. 6) in the context of the JBI model is defined by Jordanet al. (8) as: “a purposeful and enabling set of activities designed to engage keystakeholders with research evidence to inform decision-making and generate sustainedimprovement in the quality of healthcare delivery”. The three main components of thisphase are context analysis, facilitation of practice change, and evaluation of the processand outcome.Fig. 5.Evidence transferFig. 6.Evidence onSource: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.Source: Jordan et al. (8). Reproduced by permission of The Joanna Briggs Institute.Prior to the adoption of an evidence-based intervention, it is necessary to design acomprehensive implementation plan (4) that takes into consideration the principlesof organizational culture, capacity, communication and collaboration (8). It is vitallyimportant to have a plan on how to monitor and evaluate, and to sustain changes madeto health-care practice (8). Health-care professionals, educators, researchers, leaders andpolicy-makers have specific roles and responsibilities in the phases of implementing EBP (1).Example 3. Improving patient safety through evidence-based hand-hygiene practicesGood hand hygiene improves patient safety and outcomes through reducing care-associatedinfections. The model for hand-hygiene practice evaluation and development provides evidencebased structure and guidance for systematic and consistent monitoring of hand-hygiene practices.Combining measurement of fidelity to guidelines with compliance rates reveals inconsistenciesbetween optimal and actual hand-hygiene behaviour. Korhonen et al. (14) evaluated hand-hygienepractices in a Finnish university hospital. Their observations suggested the compliance rate was ashigh as 78%, meaning that health professionals routinely used hand sanitizers. Fidelity measures,however, showed that hand-rubbing practices were followed according to the recommendation(which states that the overall duration of hand-rubbing should last 30 seconds or more) in only10% of cases. It is therefore necessary to measure fidelity to guidelines to gather more specificdata about the implementation of EBP (15).5
6FACILITATING EVIDENCE-BASED PRACTICE INNURSING AND MIDWIFERY IN THE WHO EUROPEAN REGIONEvidence-based practiceEBP is a generic term that originally arose from the field of medicine. It is universallydefined as: “the conscientious, explicit and judicious use of current best evidence inmaking decisions about the care of the individual patient” (16).EBP is an interdisciplinary approach to decision-making in clinical practice (17,18) thatincludes the best available evidence, the care context, client values and preferences, andthe professional judgement of the health professional (9). It is important for nurses andmidwives to recognize that a variety of external and clinical information is needed inevidence-based clinical decision-making. Further, clinical decision-making is affected bysocietal values and explicit and implicit values in the health system (19).The four aspects of evidence-based decision-making are shown in Infobox 2.Infobox 2. Aspects of evidence-based decision-makingThe four aspects of evidence-based decision-making are: integration of the best available evidence generated by quality research; clinical evidence and expertise; patient values and preferences; and relevant contextual knowledge, which includes available resources and acknowledgespotential resource barriers and enablers within the context of care (20–23).The EBP movement began with the identification of the research-to-practice gap (24)and developed into a movement in which the principles of EBP have been applied todecision-making at different levels of the health system and to other fields of professionalpractice in health and social care, such as dentistry, nursing, midwifery, psychology,public health, radiology, social work, and policy and management (25,26). Today, EBP isconsidered a key component of modern health care.The aim of evidence-based approaches to clinical practice is to deliver appropriate care inan efficient manner to the patient. EBP has been described as doing the right things rightand doing things efficiently to the best standard possible, while ensuring that what isdone is of known effectiveness (27). EBP results in quality patient outcomes when deliveredin a context of caring supported by an organizational culture that supports EBP (28).Currently, the concept of evidence-informed practice (EIP) is often used interchangeablywith EBP without consideration of the differences or similarities. It has been argued thatthe evidence-based approach is too restrictive and medicine-oriented, and that decisionmaking must rely on additional forms of evidence (29,30). Some researchers argue that EIPprovides more flexibility in the nature of the evidence used, and that EIP extends beyondthe early definitions of EBP (29). For this reason, international debate on the utilization ofthese two concepts is ongoing.
EVIDENCE-BASED HEALTH CARE AND PRACTICEThe definition of EIP contains similar components to that of EBP, such as evidence,patient preferences and actions, clinical state and circumstances, and health-careresources. These components are brought together by clinical expertise, through whichdecisions can be informed.The term evidence-informed practice has been used, especially in public health and socialcare. It is defined as: “a complex, multi-disciplinary process that occurs within dynamicand ever-changing communities and encompasses different sectors of society” (31). Laviset al. (32) emphasize the use of research to inform public policy-making, where a range ofevidence is needed to make decisions.Example 4. Evidence-informed Policy NetworkThis is a global WHO initiative that promotes the systematic use of health-research evidencein policy-making and aims to increase Member States’ capacity to develop health policy that isinformed by research evidence. The network is key in supporting implementation of the Europeanpolicy framework, Health 2020, and provides a good example of collaboration among countries onutilizing evidence to inform health policies (33).The evidence-informed approach continues to evolve as understanding and expertiseincrease (34). Some authors promote use of the term EIP to emphasize that the decisionmaking process is person-centred rather than solely focused on scientific research,which, it has been claimed, has taken the humanity out of clinical practice (35).Both approaches, however, recognize the importance of considering patients/clients’individual needs, unique values, preferences and circumstances in addition to thescientific evidence that supports and informs clinical decision-making.The real difference between these two approaches in health care remains open to debate.For this reason, the broader concept of EBP is used in this guide.7
8FACILITATING EVIDENCE-BASED PRACTICE INNURSING AND MIDWIFERY IN THE WHO EUROPEAN REGION3. BENEFITS OF EBPThe number of research studies that strive to describe the benefits of making evidencebased decision-making standard practice in health systems is vast. EBP is a complexphenomenon and it is difficult to prove direct causal relationships between the structureof EBP and outcomes in health care. Currently, research mainly focuses on specificinterventions and their outcomes. Evidence on the benefits of EBP consequently is mainlyindicative. EBP nevertheless has the potential to improve quality of care and producebenefits for patients, nurses and midwives, and the health-care system. It is imperativefor countries in the WHO European Region to consider the benefits of EBP and focus oncontinuous improvement in quality of care.The countries of the Region have a wide range of health-system structures and showsignificant variability in health-care expenditure (36). Regardless, the burden of unsafecare is a serious global health issue and a challenge in all countries, making it imperativethat policy-makers continue to critically evaluate the quality and safety of care (37).Health systems that achieve major gains in patient safety, effectiveness of health-carepractices, timeliness of treatment, efficiency and equitability of health-care services, andprovide patient-centred care can improve the quality of health care and ultimately bettermeet patients’ needs (38).Issues around quality and safety in health care are discussed in Infobox 3.Infobox 3. Quality and safety in health careThe concepts quality and safety in health care cannot be separated. According to the Agency forHealthcare Research and Quality (39), safety is a component of quality.Quality of care is: “the degree to which health services for individuals and populations increase thelikelihood of desired health outcomes and are consistent with current professional knowledge” (38).Patient safety is defined as the absence of preventable harm to a patient during the process ofhealth care (40).Benefits of EBP have been divided into benefits for the general population, nurses andmidwives, health-care systems, and research and education. They are synthesized inTable 1 and described briefly below.Benefits for the general populationImplementing EBP creates the conditions for patient-centred care, which is defined byBerwick (41) as:the experience (to the extent the informed, individual patient desires it) of transparency,individualization, recognition, respect, dignity, and choice in all matters, without exception,related to one’s person, circumstances, and relationships in health care.Patient preferences and values are essential cornerstones of EBP, requiring patientinvolvement and sharing of the information they need to make informed decisions
BENEFITS OF EBPTable 1. Benefits of EBPBeneficiaryBenefitsGeneral population Improved conditions for patient-centred carePatient preferences included in decision-makingConsistent health services leading to better equityReduction in geographic variationReduction in patients’ length of stayBetter patient outcomesQuality health-care servicesIncreased patient safetyNurses and midwives Increased job satisfactionEmpowermentImproved skills to integrate patient preferences into practiceSupport for professional growthContinuous career development through expert rolesHealth-care systems Improvement in the quality of careBetter outcomes for patientsIncreased patient safetyReduced costsStronger basis for health-care investment decisionsCapacity-building through collaborationResearch and education Increased need for production and synthesis of robust evidence Competence development Integration of nursing and midwifery expert roles in healthsystemsSource: Nursing Research Foundation.about their care and promote their health (42). Carter et al. (43) propose a framework forhealth promotion that combines the domains of evidence, ethics and values in healthpromotion-related decision-making. This approach may enable EBP to be more ethical,and ethically sensitive practice to be more effective (43).Including patient preferences in the decision-making process ultimately has a positiveimpact on the outcomes of care and health promotion (44). Successful implementation ofEBP enables patients to experience quality health-care services with better outcomes andincreased safety (45–51).Example 5. Involving patients in decision-makingSwift & Callahan’s (44) meta-analysis summarizing data from over 2300 clients across 26 clinicaltrials and other quantitative studies found that patients who were matched to their preferredpsychological treatment had a 58% chance of showing greater outcome improvement and werehalf-less likely to discontinue treatment compared to those who were not matched. The qualityof the included studies in this meta-analysis is nevertheless unclear, so the results are mainlyindicative.9
10FACILITATING EVIDENCE-BASED PRACTICE INNURSING AND MIDWIFERY IN THE WHO EUROPEAN REGIONConsistency and the standardization of health-care practices enable patients to receivethe best possible care regardless of where they live. Consistency can be promoted through,for instance, evidence-based clinical-practice guidelines, the use of which can realizebenefits such as reduction in patients’ length of stay in health-care facilities (52) andreduction in geographic variation in health-care delivery (45,53).Example 6. Evidence-based guidelines to promote patient safetyHealth-care-associated infections represent the most frequent adverse event affecting patientsafety worldwide. WHO has published a global evidence-based guideline on preventing surgicalsite infections that is suitable for local adaptation in all countries (54). The guideline includes29 recommendations for prevention and guidance on how to disseminate and implement theguideline.Benefits for nurses and midwivesHealth professionals’ strong belief in the value of EBP correlates with increased levels ofEBP implementation, job satisfaction (55) and group cohesion (28). Nurses and midwiveswho believe in their ability to deliver high-quality care may feel more empowered in theirroles and may experience increased cohesion in team stru
based practice and innovation in nursing and midwifery. It aims to promote a shared understanding of evidence-based practice in nursing and midwifery and strengthen its foundations in the Region to support health policy-makers, health-care professionals and others in facilitating the culture of evidence-based practice in nursing and midwifery.