Transcription
California HospiceLicensure and OversightThe State’s Weak Oversight of Hospice AgenciesHas Created Opportunities for Large-Scale Fraudand AbuseMarch 2022REPORT 2021-123
CALIFORNIA STATE AUDITOR621 Capitol Mall, Suite 1200 Sacramento CA 95814916.445.0255 TTY 916.445.0033For complaints of state employee misconduct,contact us through the Whistleblower Hotline:1.800.952.5665Don’t want to miss any of our reports? Subscribe to our email list atauditor.ca.govFor questions regarding the contents of this report, please contact our Public Affairs Office at 916.445.0255This report is also available online at www.auditor.ca.gov Alternative format reports available upon request Permission is granted to reproduce reports
Michael S. Tilden Acting State AuditorMarch 29, 20222021‑123The Governor of CaliforniaPresident pro Tempore of the SenateSpeaker of the AssemblyState CapitolSacramento, California 95814Dear Governor and Legislative Leaders:As directed by the Joint Legislative Audit Committee, my office conducted an audit of the State’slicensure and oversight of hospice agencies and found that the State’s weak controls have createdthe opportunity for large-scale fraud and abuse. We identified numerous indicators of such fraudand abuse by hospice agencies, which typically offer palliative end-of-life care to individuals withmedical diagnoses of fewer than six months to live. The fraud indicators we found particularly inLos Angeles County include the following: A rapid increase in the number of hospice agencies with no clear correlation toincreased need. Excessive geographic clustering of hospices with sometimes dozens of separately licensedagencies located in the same building. Unusually long durations of hospice services provided to individual patients. Abnormally high rates of still-living patients discharged from hospice care. Hospice agencies using possibly stolen identities of medical personnel.These indicators strongly suggest that a network or networks of individual perpetrators inLos Angeles County are engaging in a large and organized effort to defraud the Medicare andMedi-Cal hospice programs. Such fraud places at risk the extremely vulnerable population ofhospice patients.The California Department of Public Health’s (Public Health) inadequate performance of itslicensing and investigative functions has enabled this suspected fraud. Without regulations toguide its oversight, its initial licensing site visits and ongoing monitoring do not adequatelysafeguard patient care or prevent fraud. Its investigation of complaints involving hospice agenciesis often incomplete and slow, which increases the risk that patients may receive substandard careor that hospice agencies may engage in fraudulent activity. Public Health has not sought statutoryenforcement measures to address problems that it identifies through its oversight, and PublicHealth and the California Department of Health Care Services do not coordinate with each otherto comprehensively assess fraud risks.Respectfully submitted,MICHAEL S. TILDEN, CPAActing California State Auditor621 Capitol Mall, Suite 1200 Sacramento, CA 95814 916.445.0255 916.327.0019 fax w w w. a u d i t o r. c a . g o v
ivCalifornia State Auditor Report 2021-123March 2022Selected Abbreviations Used in This ReportCal Health FindCalifornia Health Facility Information DatabaseCMSCenters for Medicare and Medicaid ServicesDOJCalifornia Department of JusticeMedPACMedicare Payment Advisory CommissionOIGOffice of the Inspector General of the U.S. Department of Health and Human Services
California State Auditor Report 2021-123March 2022ContentsSummary1Introduction5Chapter 1Numerous Indicators Suggest Large-Scale Hospice Fraud and Abuse inLos Angeles County17Chapter 2Public Health Has Failed to Provide the Level of Oversight Necessary toPrevent Fraud and Abuse by Hospice Agencies31Chapter 3State Agencies Have Not Adequately Coordinated Their FraudPrevention Efforts or Developed Meaningful Enforcement MeasuresFor the Medi-Cal Hospice Program43Conclusions and Recommendations49AppendixScope and Methodology55Responses to the AuditCalifornia Department of Justice59California Department of Health Care Services63California Department of Public Health67California State Auditor’s Comments on the Response Fromthe California Department of Public HealthCalifornia Department of Social ServicesCalifornia State Auditor’s Comments on the Response Fromthe California Department of Social Services777981v
viCalifornia State Auditor Report 2021-123March 2022
California State Auditor Report 2021-123March 2022SummaryResults in BriefIn the past 10 years, growth in the number of hospice agenciesin Los Angeles County has vastly outpaced the need for hospiceservices. Hospice agencies provide end‑of‑life care for individualswho are terminally ill—patients who are extremely vulnerable andheavily reliant on caregivers. Although the majority of hospiceservices were provided by nonprofit organizations in the past, thisrecent wave of growth is almost exclusively in for‑profit companies.Further, numerous indicators suggest that many of these hospiceagencies may have been created to fraudulently bill Medicare andMedi‑Cal for services rendered to ineligible patients or services notprovided at all. This type of fraud can be lucrative. For example,a hospice agency that bills for 20 patients at the most commonrate can collect about 122,000 per month. Nonetheless, the stateagencies responsible for overseeing hospice care in California havefailed to take adequate measures to prevent such fraud or to protectpatients from unqualified and unscrupulous providers.The prevalence and number of fraud indicators in Los AngelesCounty suggest a large‑scale, targeted effort to defraud Medicareand Medi‑Cal. For example, we identified several areas withinLos Angeles County with extremely high concentrations of hospiceagencies, including individual buildings supposedly housing dozensof hospice agencies. In fact, the California Department of PublicHealth (Public Health) reported a single building in the communityof Van Nuys as having more than 150 licensed hospice and homehealth agencies—a number that exceeds the structure’s apparentphysical capacity. Further, in 2019 Los Angeles County had morethan six times the national average number of hospice agenciesrelative to its aged population. Consequently, each hospice agencyin the county had an estimated average of fewer than five patientsper day, as opposed to the average for the rest of the State of56 patients per hospice agency per day.Because of the interrelationship between fraud and patient abuse,the prevalence of fraud indicators raises significant concerns aboutpatient care quality. Los Angeles County hospice agencies haveunusually long durations of patient care and high rates of patientsbeing discharged alive. Given that hospice patients are by definitionin the last stages of their life, these trends seemingly indicate thatat least some hospice agencies are enrolling patients who are noteligible for hospice services because they are not actually sufferingfrom terminal illnesses; at the same time, those patients mayexperience being deprived of the curative care that they need.We also found cases where hospice agencies appear to be usingthe names of medical professionals without their knowledge orAudit Highlights Our audit of the State’s licensure andoversight of hospice agencies highlightedthe following:» Los Angeles County has experienced a1,500 percent increase in its number ofhospice agencies since 2010. It had more than six-and-a-half timesthe nationwide average number ofhospice agencies relative to its agedpopulation in 2019.» We found indicators of large-scale fraudthat include likely fraudulent billing toMedicare and Medi-Cal and the apparentuse of stolen identities of medicalpersonnel to obtain licenses.» Public Health’s perfunctory hospiceagency licensing process does little toverify that personnel are qualified orprevent fraud. Its limited monitoring does notadequately protect patients. It has failed to performinvestigations promptly.» State agencies have notadequately coordinated their fraudprevention efforts. Public Health, Health Care Services, andDOJ have not comprehensively assessedfraud risks related to hospice agencies.1
2California State Auditor Report 2021-123March 2022consent, thereby obtaining hospice licenses under false pretenses.In these instances, it is not clear who—if anyone—is providing careto patients.Public Health—the state agency primarily responsible for thelicensing and oversight of hospice agencies—has failed to takeadequate action in the face of such widespread problems. Mostcritically, it has yet to issue regulations for its hospice licensingprocesses, despite having had the authority to do so since 1991.For example, its current initial licensing process does not requireadequate screening to ensure that hospice employees are qualifiedto provide services to patients. Moreover, we reviewed cases inwhich Public Health became aware of possible fraud during thelicensing process and instead of denying the licenses, it grantedlicenses to these hospice agencies. In these instances, it essentiallyenabled hospice agency operators who are possibly fraudulentto continue functioning, placing patients at serious risk of notreceiving appropriate care.In addition, we found that Public Health does not always adequatelyinvestigate complaints of patient abuse. Public Health frequentlytakes significant time to conclude complaint investigations,despite the short period hospice patients are likely to remainalive. In fact, the average time Public Health takes to complete acomplaint investigation is more than five months—near the upperlimit of a Medicare or Medi-Cal hospice patient’s expected lifespan. Moreover, Public Health does not always conduct thoroughinvestigations. We found instances in which it failed to interviewpertinent witnesses or gather complete information, potentiallyendangering both the patients involved and future patients whomight face abuse from the same agencies. Even when Public Healthfinds instances of wrongdoing, it has limited recourse to sanctionhospice agencies under current state law. At the same time, it hasfailed to use the most powerful tools currently available to it asa means to curb violations: since 2015 it has never suspended ahospice license and has revoked a hospice license only once.Despite these widespread problems in the hospice program,Public Health and the two state agencies primarily responsiblefor identifying and investigating hospice fraud in Medi‑Cal—theCalifornia Department of Health Care Services (Health CareServices) and the California Department of Justice (DOJ)—have not sufficiently coordinated their efforts. The lack ofsuch coordination has resulted in gaps in the system, which isdesigned to protect hospice patients from harm and to guard theState’s Medi‑Cal system against fraud. For example, Health CareServices and Public Health do not coordinate with each other tocomprehensively assess fraud risks, such as those we found in
California State Auditor Report 2021-123March 2022Los Angeles County. These siloed and disjointed efforts by stateagencies are not sufficient to address the large‑scale fraud that islikely occurring in the hospice industry.Selected RecommendationsLegislatureTo address the fraud that is likely occurring in Los AngelesCounty, the Legislature should require Public Health, Health CareServices, and DOJ to immediately convene a task force to identify,investigate, and prosecute fraud and abuse by hospice agencies inthat county. It should also require these departments to establisha working group for conducting an annual risk assessment ofthe Medi‑Cal hospice program statewide, including performinganalyses similar to those we conducted during this audit regardinggrowth in the number of hospice agencies and clustering ofhospice agencies.To protect the health and safety of current and prospectivehospice patients, the Legislature should require Public Health toimmediately begin the process of developing emergency regulationsfor its hospice licensing process. The regulations should specificallyinclude a process for verifying the identity and qualifications ofhospice agency management personnel among other items.To ensure that hospice agencies comply with licensing requirements,the Legislature should revise state law to include a system ofsanctions for Public Health to levy, including monetary fines.We present the complete list of our recommendations starting onpage 49.Agency CommentsThe Health and Human Services Agency did not provide aconsolidated response to the report, but instead allowed eachof its departments (Public Health, Health Care Services, andSocial Services) to respond to the conclusions and recommendationsthat were directed to each entity. Public Health agreed with mostof our recommendations but indicated that some may requireadditional legislation. Health Care Services, Social Services, andDOJ agreed with our recommendations to them.3
4California State Auditor Report 2021-123March 2022
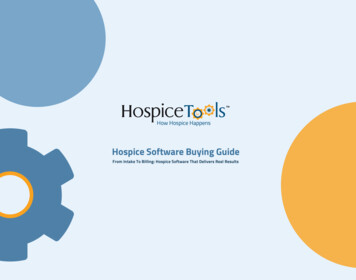
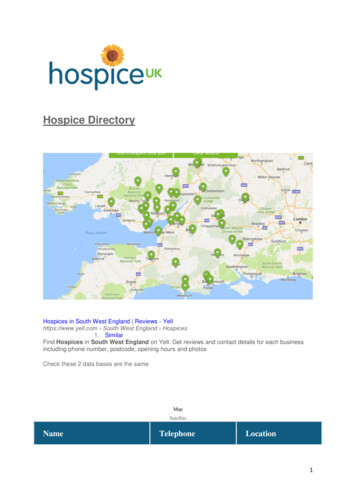
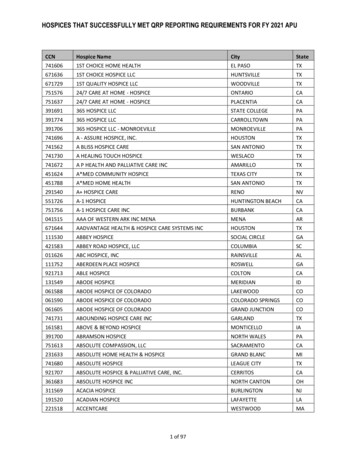
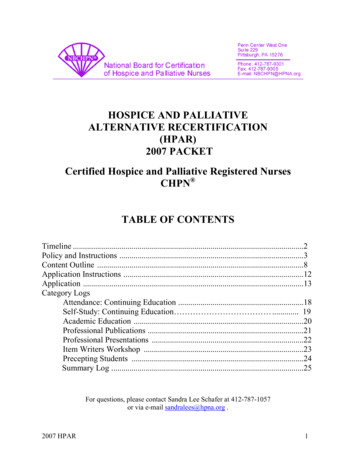
California State Auditor Report 2021-123March 2022IntroductionBackgroundHospice is a specialized form of interdisciplinary health careprimarily designed to provide palliative care and alleviate thephysical, emotional, social, and spiritual discomforts of a person whois experiencing the last phases of life because of a terminal disease.Palliative care optimizes the quality of life of a patient with a terminalillness by anticipating, preventing, and treating suffering. Hospicecare treats pain and other symptoms associated with a terminaldisease, rather than attempting to cure the disease when a cure is nolonger possible or when the burdens of curative treatment outweighthe benefits. Individuals who receive hospice care are commonlyfacing terminal cancer, heart disease, or neurological diagnoses, suchas Alzheimer’s disease. Often bedridden and cognitively impaired,hospice patients rely heavily on caregivers and are consequently one ofthe State’s most vulnerable populations.Hospice care is provided in the patient’s home when appropriate.However, as Figure 1 describes, hospice care can also be providedin other settings, such as a hospital or skilled nursing facility, and asmall number of health facilities in California specialize exclusively ininpatient hospice care. Hospice agencies use interdisciplinary teamsto assess the physical, emotional, social, and spiritual needs of patientsand their families. The interdisciplinary team must then develop anoverall plan of care that includes the services listed in Figure 1.More than 2,800 hospice agencies were licensed to operate in theState as of January 2022. Figure 2 shows the locations of the businessoffices of these licensed hospice agencies, the majority of which are inLos Angeles County. Until 2007 California had more nonprofit hospiceagencies than for‑profit ones. However, as of January 2022, about94 percent of hospice agencies in California were for‑profit companies.According to federal data as of August 2021, California had the highestpercentage of for‑profit hospice agencies of all 50 states. Federal dataalso indicate approximately 162,000 individuals in California used theMedicare hospice benefit at some point during 2020.1Licensure and Oversight of Hospice AgenciesUnder the California Hospice Licensure Act of 1990 (Licensure Act), theCalifornia Department of Public Health (Public Health) is responsiblefor licensing hospice agencies in the State. Licensing consists of twomain components to ensure that hospice agencies comply with state1 Public Health does not track the number of hospice patients in the State.5
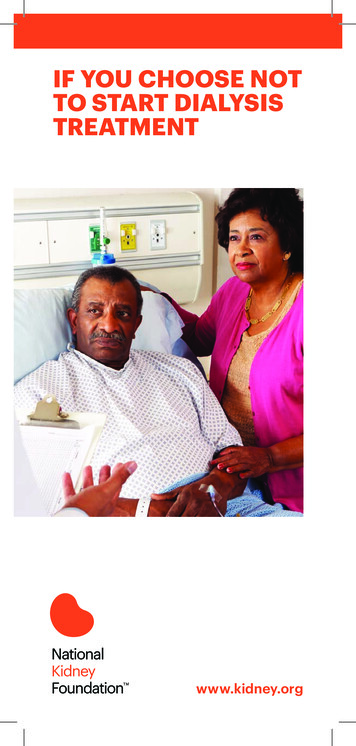
6California State Auditor Report 2021-123March 2022Figure 1Hospice Agencies Provide Palliative Services to Individuals Who Are Terminally IllIn California, 94 percent of hospice agencies are for-profit companies.Each must have an administrator who manages the day-to-day operations as well as abusiness office where patient medical files and other documentation are kept.A hospice agency uses aninterdisciplinary team that includes: The patient and patient’s family.A physician.A registered nurse.A social worker.A volunteer.A spiritual caregiver.Hospice care consists ofservices and supplies, such as: Nursing services. Medical supplies, including drugsfor pain management. Homemaker services. Spiritual and grief counseling.When appropriate, hospice agencies providecare in the patient’s home.But a patient can also receivehospice care in other settings, such as askilled nursing facility or hospital.Source: Federal and state law, hospice standards, and Public Health’s licensing data.requirements: an application and an initial site visit.2 State lawspecifies that to qualify for a license, an applicant must submit acompleted application, be of good moral character, demonstratethe ability to comply with state law governing hospice care, andpay a fee of 2,971. Figure 3 illustrates the key documentation thata prospective hospice agency must submit to Public Health todemonstrate that it meets licensure requirements. Public Health’sCentral Application Branch reported in December 2021 having sevenstaff who review applications for completeness.2 We refer to Public Health’s initial visit to a hospice agency’s office before it is licensed as an initialsite visit and all subsequent visits as inspections. We do so to differentiate between the initialvisit, which occurs when the hospice agency is not yet operating, and subsequent visits when thehospice agency is serving patients and Public Health can assess the quality of care it is providing.
California State Auditor Report 2021-123March 2022Figure 2Hospice Agencies Are Located Throughout the StateCount3 1011 5051 100101 25042 10002,8361total statewide3111212744ALAMEDA54431162312Counties without numbers do not have anylicensed hospice agencies. County totalsinclude hospice facilities.711114915419121225151423SAN BERNARDINO22012VENTURA80LOS ANGELES1,841ORANGE189RIVERSIDE82SAN DIEGO874Source: Public Health’s data visualization website.The license to operate as a hospice agency is valid for 24 months,after which the hospice agency must submit an application forrenewal and a renewal fee of 2,971. Although the LicensureAct permits Public Health to inspect hospice agencies, it doesnot require Public Health to conduct an inspection as part oflicense renewal.As part of the licensing requirements, state law requires thathospice agencies provide services in compliance with the 2003version of the Standards of Quality Hospice Care developed bythe California Hospice and Palliative Care Association (hospicestandards). The hospice standards establish requirements forseveral aspects of hospice care, including the services an agencymust provide, an agency’s use of plans of care and interdisciplinaryteams, and a hospice agency’s staffing and administration.7
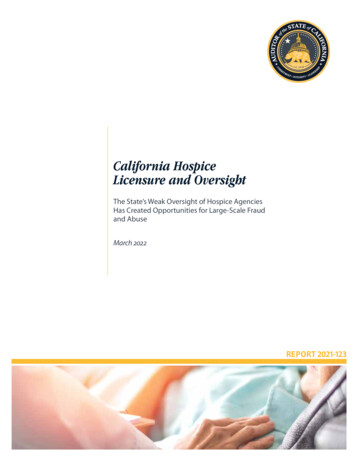
8California State Auditor Report 2021-123March 2022Figure 3Prospective Hospice Agencies Must Submit Specific Documentation toPublic Health Demonstrating That They Meet Licensure RequirementsKey Required DocumentationApplication formHospice agency bylawsResume/experience ofkey personnelMedical licenses ofproposed medical staffGeographic service areaEvidence of a physical office location,such as a lease and floor plan ofhospice agency’s business office spaceOrganization chart that identifies key personnel, including: Administrator (manages day-to-day operations) Medical director (physician responsible for overallmedical direction; position can be contracted) Director of patient care services (managing nurse) Individuals designated to act in the temporary absence ofthe administrator and director of patient care servicesSource: State law, hospice standards, and Public Health license application.Public Health’s 14 district offices perform the initial site visits forhospice agencies located in their jurisdictions, during which theyare responsible for touring each hospice agency’s office, reviewingits personnel records, and verifying that it complies with thehospice standards.
California State Auditor Report 2021-123March 2022Public Health is also responsible for investigating complaintsagainst licensed hospice agencies. It receives complaints througha variety of channels, including telephone, mail, email, its website,and referrals from other entities. When Public Health receives acomplaint, it assigns it to one of its district offices based on thelocation of the hospice agency. District office staff review andprioritize the complaint based on its urgency. Public Health thenassigns one of its staff members to complete the investigationaccording to a plan that identifies the necessary record reviews,interviews, and observations to attempt to substantiate thecomplaint’s allegations. Once it completes the investigation,Public Health notifies the person who submitted the complaint ofthe results in writing.Public Health contracts with the Los Angeles County Departmentof Public Health to conduct licensing and certificationresponsibilities in that county, whereas Public Health maintainsresponsibility for all other counties in the State. Public Healthcharges license applicants an additional supplemental fee of 3,850 in Los Angeles County to cover the cost of its contractwith the county. Because the Los Angeles County Departmentof Public Health carries out Public Health’s policies and operatesprograms as requested by Public Health in performing itscontractual licensing and certification responsibilities and becauseit operates under the oversight of Public Health, we do not draw adistinction in this report between the two entities.Other federal and state entities also oversee components ofhospice care, as we show in Figure 4. For example, the CaliforniaDepartment of Social Services (Social Services) licenses andinspects residential care facilities, which may house patientswho are receiving hospice services. It also assists counties in theoperation of their adult protective services programs, which mayreceive complaints from mandated reporters for elder abuse.Federal and State Payments for Hospice ServicesTo be eligible for payment from Medicare, hospice agencies mustmeet federal requirements for hospice care, known as conditionsof participation. The Centers for Medicare and Medicaid Services(CMS)—the federal agency that administers Medicare—mustverify that hospice agencies meet these conditions, includingthose listed in the text box. The Social Security Act of 1935establishes a framework that allows state agencies to performthe Medicare certification process to determine whether hospiceagencies meet federal standards, including performing certificationinspections at least every three years. In California, Public Healthcompletes these certification inspections on behalf of CMS. In9
10California State Auditor Report 2021-123March 2022Figure 4Various Public and Private Entities Play a Role in Hospice Oversight in CaliforniaFEDERALCenters for Medicare &Medicaid Services Administers the Medicare andMedicaid programs at the federal level. Certifies hospice agencies toreceive payment from Medicare.U.S. Department of Health andHuman ServicesOffice of Inspector GeneralandU.S. Department of Justice Investigate Medicare fraud.STATECalifornia Department ofPublic HealthCalifornia Department of JusticeOffice of the Attorney General Licenses hospice agencies in California. May perform inspections to ensurecompliance with requirements. Investigates complaints. Receives reports from mandatedreporters regarding elder abuse incertain long-term care facilities. Investigates and prosecutes Medi-Calprovider fraud, as well as abuse orneglect of patients in health carefacilities receiving Medi-Cal payments.Contracting withCounty of Los Angeles Public Health Contracted by California Departmentof Public Health to perform licensingand certification services inLos Angeles County.California Department ofHealth Care Services Determines Medi-Cal eligibility of patients. Processes Medi-Cal payments. Investigates suspected Medi-Cal fraud.California Department of Social ServicesACCREDITORS Perform certification/recertification for Medicare. Perform licensing initial site visits aspart of Medicare certification. Licenses residential care facilities for the elderly, which can house patients who arereceiving hospice care. Receives reports from mandated reporters regarding elder abuse occurring inresidential care facilities. Assists counties in the operation of their adult protective services programs, which mayreceive complaints from mandated reporters for elder abuse occurring outsidelong-term care facilities.Source: Federal and state law, CMS State Operations Manual, OIG website, U.S. Department of Justice website, and Public Health and Los AngelesCounty’s licensing and certification contract.addition, hospice agencies in California can elect to have theircertification inspections performed by one of three state‑contractedaccreditation organizations (accreditors) instead of Public Health.We discuss in the next section the process through which hospiceagencies are certified by accreditors.Medicare is the largest payer of hospice services; in particular,it covered the costs of nearly 92 percent of hospice patientdays nationally in 2018. Patients must meet certain eligibilityrequirements to qualify for hospice care under Medicare, includingbeing certified as terminally ill, meaning that a hospice agencyphysician and the patient’s attending physician, if there is one, havedetermined that the patient’s life expectancy is likely six months orless if the illness runs its normal course. This certification covers an
California State Auditor Report 2021-123March 2022initial 90‑day period, after which the patient mustbe recertified. The hospice agency must obtain suchwritten certification for each patient. By electingto receive hospice care, patients forgo curativetreatment of the terminal illness, which Medicarewill no longer cover.In 2020 Medicare paid more than 3 billionfor hospice services to 162,000 patients in theState. Medicare pays for each day a patient is inthe hospice agency’s care based on one of fourcategories, as Table 1 shows. The most commoncategory of care is called routine home care. Ahospice agency receives the routine home care dailypayment rate regardless of the amount of service itprovides to the patient on that day. This paymentmodel can generate substantial revenue for ahospice agency. For example, for 20 patients billedat the routine home care rate that applies to the first60 days, a hospice agency can collect more than 122,000 per month.Although Medicare pays for the majority of hospiceservices in California, the State also pays for theseservices through Medi‑Cal, the State’s Medicaidprogram administered by the Department of HealthCare Services (Health Care Services). WhereasMedicare is generally for individuals who are age65 or over, Medi‑Cal generally serves low‑incomeindividuals. Similar to the rules under Medicare,patients must meet certain requirements to electto receive hospice care through Medi‑Cal. Themajority of Medi‑Cal enrollees have their coverageprovided by a Medi‑Cal managed care plan, whichpays for services through a monthly lump sum perpatient. Other Medi‑Cal enrollees receive theircare through a fee‑for‑service delivery system,where providers render services and then submitclaims for payment. Medi‑Cal had more than27,000 enrollees receiving hospice services in2020. Health Care Services does not readily haveinformation on the total Medi‑Cal managed‑careexpenditures related to hospice services, but itprovided data indicating that payments for hospiceservices for the fee‑for‑service enrollees totalednearly 150 million in 2020.Examples of MedicareHospice Conditions of Participation Patient’s rights: The patient has the right to be informedof his or her rights, and the hospice must protect andpromote the exercise of these rights. Initial and comprehensive assessment: The hospicemust document in writing a comprehensive assessmentthat identifies the patient’s need for hospice careand services. Interdisciplinary group, care planning, andcoordination of services: The hospice must designate aninterdisciplinary group, which must prepare a written planof care for each patient, specifying the hospice care andservices necessary to meet the patient and family-specificneeds identified in the comprehensive assessment. Core services: A hospice must routinely providesubstantially all core services (physician services, nursingservices, medical social services, and counseling) directlyby hospice employees in a manner consistent withacceptable standards of practice. Medical director: The hospice must designate aphysician to serve as medical director. The medicaldirector must be a doctor of medicine or osteopathy whois an employee or is under contract with the hospice. Clinical records: A clinical record containing pastand current findings must be maintained for eachhospice patient, must be available to the patient’sattending physician and hospice staff, and may bemaintained electronically. Drugs and biologicals, medical supplies, and durablemedical equipment: Those related to the palliationand management of the terminal illness and relatedconditions, as identified in the hospice plan of care, mustbe provided by the hospice while the patient is underhospice care. Personnel qualifications: With limited exceptions, allprofessionals who furnish services directly must belegally authorized (licensed, certified, or registered) andmust act only within the scope of his or her state license,certification, or registration. All personnel qualificationsmust be kept current at all times.Source: Federal and state law.Note: The conditions of
of Van Nuys as having more than 150 licensed hospice and home health agencies—a number that exceeds the structure's apparent physical capacity. Further, in 2019 Los Angeles County had more than six times the national average number of hospice agencies relative to its aged population. Consequently, each hospice agency