Transcription
PEI PAP SCREENINGPROGRAM2001 ReportMay 2002Epidemiology Unit
PEI PAP SCREENINGPROGRAM2001 ReportEpidemiology Unit, DHSSPEI Pap Screening Program Advisory CommitteeHealth andSocial ServicesMay 2002
AcknowledgmentsThe PEI Pap Screening Program would like to thank its partners, the PEI Divisionof the Canadian Cancer Society, the Medical Society of PEI, PEI Women’sNetwork and the PEI Department of Health & Social Services, who have supportedand contributed to this program.The success of the PEI Pap Screening Program also depends on an integratedsystem of health professionals taking the Pap smears, dedicated and trained staffto process and read the slides as well as medical specialists to provide colposcopyand treatment follow-up. Thank you.Thanks also to the NS Gynaecological Cancer Screening Programme for supportduring the development of the program, including the use of the “Pap Screeningfor Life” logo. Also thanks to Western Newfoundland for their input and sharing ofinformation.
Executive SummaryOver 90% of cervical cancer can be prevented by regular screening with the Pap test.In spite of access to the Pap test since the 1960's, the incidence of cervical cancerhas been increasing in PEI, in contrast to the declining Canadian rate. Most cases ofcervical cancer occur in women not regularly screened. This highlights the need for amore organized approach to cervical cancer screening in PEI.Prior to the formal establishment of the PEI Pap Screening Program in 2001, mucheffort had gone into developing the groundwork for an organized screening program.This work was a prelude to the January 16, 2001 inaugural meeting of the PapScreening Advisory Committee, a multi-disciplinary group to oversee the diverseresponsibilities and interests in cervical cancer. The PEI Pap Screening Program’sgoal is to reduce the incidence and mortality from cervical cancer among Islandwomen.Highlights of the activities in the PEI Pap Screening Program’s first year include thePap Screening Clinic, Pap Awareness Week, and reporting on program indicators.The Pap Screening Clinic was launched September 6, 2001 in Cornwall, PEI. Thegoal of the clinic is to increase the number of women regularly screened with a Paptest by providing an alternative service to increase accessibility. The clinic’s trainedregistered nurse provides Pap tests under the supervision of Dr. DI Stewart. Overthe period September to December 2001, 477 women had a Pap at the clinic.The majority of the women attending the Clinic were overdue for Pap screening: 75%of the women attending had their last Pap two or more years ago.PEI’s second Pap Awareness Week campaign was held October 20 to 27, 2001.This campaign resulted from coordinated efforts with campaigns in Nova Scotia andNewfoundland, the implementation of a PEI marketing strategy, and the evaluation ofPEI’s 2000 campaign. The main focus of this campaign was to increase awarenessthat cervical cancer can be prevented by regular Pap tests. The key messages weredelivered using a media blitz and promotional materials that maintained the visualidentity of PEI’s 2000 campaign.The program indicators available in this report are statistical measures of programperformance that can be used to inform policy decisions, and to assess programeffectiveness. The PEI Pap Screening Program encourages regular screening atleast every two years. PEI’s overall two year screening rate during 2000-2001 forwomen aged 20 to 69 was 58%.Future challenges for the PEI Pap Screening Program include continuing thedevelopment towards an organized provincial screening program, with an emphasison increasing regular Pap screening.
Table of Contents1.Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21.1Cervical Cancer1.2National Background1.3PEI Background2.Organized Cervical Cancer Screening Programs . . . . . . . . . . . . . . . . . . . . . . . 52.1International Programs2.2National Recommendations2.3Provincial Screening Activity3.PEI Pap Screening Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83.1Program Structure3.2Program Goals4.Program Indicators for PEI Pap Screening . . . . . . . . . . . . . . . . . . . . . . . . . . . 104.1Participation Rates for PEI4.2Specimen Adequacy4.3Cytology Results4.4Follow-up Recommendations4.5Incidence of Cervical Cancer4.6Mortality of Cervical Cancer5.Program Activities in 2001 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165.1Pap Awareness Week5.2Pap Screening Clinic5.3Cytology Laboratory5.4Screening Guidelines5.5Performance Indicators6.Future Challenges7.Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21ARecruitment StrategiesBLiability for Follow-upCProfile of Unscreened WomenDWell Woman ClinicsEUnderstanding the Barriers to Cervical Cancer Screening in PEIF2000 PEI Pap Awareness CampaignGTerms of Reference - Advisory Committee, Working GroupsHDetailed Data for Program IndicatorsIMinimum Data for Cytology RegistryJCytology Registry UpgradesKPap Screening Clinic. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20PEI Pap Screening Program, 2001 Report1
1.INTRODUCTIONThe purpose of this report is two-fold: to document the activities leading up to theestablishment of a provincial Pap Screening Program; and to provide a report on theactivities occurring in the first year of the program from January 1, 2001 to December31, 2001.The PEI Pap Screening Program’s goal is to reduce the incidence and mortality fromcervical cancer among Island women. The Program encourages regular screening forcervical cancer.1.1Cervical CancerThe cervix is the lower part of the uterus, and is found at the top of the vagina. Thecells covering the cervix can become malignant (uncontrolled cell growth), causingcervical cancer. Cervical cancer is slow to develop. It generally develops before theage of 70; the average age of diagnosis is 45 years. The cells of the cervix gothrough mild to severe changes over a period of years before the cells change tocancer. At the early stages of these changes, there are no signs or symptoms.However, the early cell changes can be detected and treated before cancer develops.Over 90% of cervical cancer can be prevented by regular Papanicolaou (Pap) tests.The Pap test is a simple and effective procedure for detecting precancerousconditions. Since the Pap test was introduced 40 years ago, deaths from cervicalcancer have declined. In Canada, the incidence of cervical cancer declined 50%between 1969 and 1990; deaths dropped by two-thirds. However, in the last tenyears, the decline has leveled off, suggesting that the current ad hoc approach toscreening which is termed opportunistic, has reached its potential.Currently in Canada, most Pap tests are performed in physician offices. Accessrelies on the individual woman’s and/or her health practitioner’s initiative.Opportunistic screening has a number of limitations including limited ability to identifyand recruit women who are at highest risk of developing cervical cancer - those whohave never had a Pap smear or do not have them regularly. Another limitation is thelack of coordinated efforts for public and professional education about cervical cancerscreening. Coordinated efforts are also conducive to quality improvement in thecollection of Pap smears, laboratory activities, and follow-up and treatment ofabnormalities.A reduction in mortality from cervical cancer is best achieved through an organizedprovincial screening program. Efforts to develop province-wide screening programshave been underway for several decades.PEI Pap Screening Program, 2001 Report2
1.2National BackgroundIn Canada, numerous recommendations have been made over the past 25 years todevelop organized approaches to cervical cancer screening. This includes theCanadian Task Forces in 1973, 1982, and 1989.In 1995 the Cervical Cancer Prevention Network (CCPN) was formed. This is aninformal network of federal, provincial/territorial and professional societies establishedto foster the development of organized provincial cervical cancer screening programsin Canada. CCPN has hosted meetings for information exchange, and producedresources including a summary of recruitment strategies (see Appendix A), guidelinesfor screening1, and a surveillance report not yet released.Interest in organized screening programs was also inspired in the spring of 2000 bypublicity of a Manitoba woman who died with cervical cancer. The woman had a paptest that indicated severe cellular changes. The follow-up biopsy and treatmentoccurred more than one year later when the patient returned with symptoms. Boththe hospital and the doctor were found legally liable for not having a system in placeto monitor cytology results (details in Appendix B).Over the past 25 years, pap screening has been a successful public health measure,with a 50% decline in the mortality from cervical cancer in Canada. However, in thelast ten years, the decline has leveled off, suggesting that the current approach toscreening has reached its potential.1.3Prince Edward Island BackgroundIn spite of some national success with cervical cancer, Prince Edward Island has notdemonstrated any declines. PEI consistently has one of the highest rates of cervicalcancer in Canada (see Sections 4.5, 4.6). Most cases occurred in unscreened orinadequately screened women2.In October 2000, Minister of Health and Social Services, Honorable Jamie Ballem,announced the establishment of the PEI Pap Screening Program, with the primarygoal of reducing the incidence and mortality rates associated with cervical cancer inPEI.1Programmatic Guidelines for Screening for Cancer of the Cervix in Canada. Quality ManagementWorking Group, CCPN. Health Canada: 1998.2Sweet et al. Review of Cervical Screening History of PEI Women. Chronic Dis Can 1991; 12(1):1-3.PEI Pap Screening Program, 2001 Report3
Prior to the formal establishment of the PEI Pap Screening Program in January 2001,much effort had gone into developing the groundwork for an organized screeningprogram. Following is the PEI activity prior to 2001:C1967 PEI physicians provide pap screening to womenC1991 Review of 54 cervical cancer cases showed the majority had not beenscreened in three or more years prior to their cancer diagnosisC1993 Survey of women (2,000 WI members) indicate 90% considered anotification letter an acceptable invasion of their privacyC1996 QEH Laboratory implemented LCMS software to capture all cytologyand histology dataC1997 Research to describe unscreened women (see Appendix C) found: 60% of Island women are screened every 3 years 40% of Island women are screened every yearC1998 Well Woman Clinics were piloted across PEI by the Well Women’sHealth Coalition (see Appendix D).C1999 A Social Marketing Plan was developed to seek provincial support fora major public education program to increase the number of womenaware of the importance of regular screeningC2000 Research on the barriers to screening (see Appendix E) found: Resistance to request a pap test Low value for preventive care Misconceptions of preventability of cervical cancer, role offamily history, recommended ages for screeningC2000 Pap Awareness Campaign in 4th week of October, along with NS andNF. The campaign included a media blitz and promotional materials(see Appendix F). The key messages for this campaign: cervical cancer can be prevented a pap test every 2 years can save your life call your family physician for an appointment todayPEI Pap Screening Program, 2001 Report4
2.ORGANIZED CERVICAL CANCERSCREENING PROGRAMS2.1International ProgramsSeveral countries provide existing examples of organized screening programs.The Australian program uses a recall period of every 2 years. The program sendsletters of recall directly to women who registered at time of their previous pap. Theprogram recorded 64% of women (20-69) screened in the 2 year interval 1997-98.The program in the United Kingdom uses a recall period of every five years. Theprogram sends letters of recall directly to women who register at the time of theirprevious pap. The program also provides doctors with incentives for collecting Paptests. The program recorded 85% of women (25-64) screened in the 5 year interval1993-97.The program in Iceland used a recall period of every 2 years, and is currentlyreviewing the use of longer recall periods. The program relied on the encouragementof physicians until 1997, when central coordination began to send letters of recalldirectly to women. The program recorded 37% of women (20-69) were screened in1996.Finland has had a program for the past 30 years that provides women aged 30 to 60years with an invitation to be screened every five years.2.2National RecommendationsIn Canada, numerous recommendations have been made over the past 25 years todevelop organized approaches to cervical cancer screening. Organized programs forcervical cancer screening would increase the efficiency of screening, and enhancethe management of abnormal tests. An organized screening programmeets the following criteria: 3 41. Organization Facilities for performing tests, diagnoses, and treatments Program structure and coordination Referral system Funding3Interchange 95 Cervical Cancer Screening Workshop, CMAJ 1996: 154(12) p. 1847-1853.4Hakama, Chamberlain, Day et al. Evaluation of screening programs for gynaecological cancer.British Journal Cancer 1985; 52: 669-6734PEI Pap Screening Program, 2001 Report5
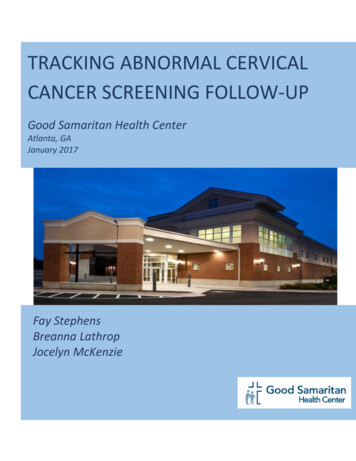
2. Information Systems Cytology database to provide screening history for each woman Histology database to provide diagnostic information Colposcopic database to provide follow-up information Recall system to doctors for overdue pap tests Linkage with population registry for recruitment3. Quality Assurance Guidelines for screening, identify target population Performance indicators for reports, ongoing evaluation and monitoring Program follow-up of abnormal pap tests (“failsafe” mechanism) Training standards, quality control Treatment options4. Education and Recruitment Pap Awareness Campaign Education for Professionals Educational Resources Recruitment initiatives for women not screened regularly,and for unscreened women2.3Provincial Screening ActivityOrganized screening programs, as described above, are in various stages ofdevelopment in the provinces. The well established programs are in BritishColumbia and Nova Scotia, with recent progress in many other provinces. Table 2.1highlights the progress toward implementation of the components of an organizedscreening program. No province has all of the components in place.In Prince Edward Island, some of the essential components in support of anorganized screening program have been put in place. PEI has a centralizedlaboratory system with a computerized information system, a network of familyphysicians that provide “opportunistic” access to screening, and recently a PapAwareness Campaign. The next step toward an organized screening program was toprovide a structure to coordinate these diverse responsibilities, and to oversee thefurther development toward an organized cervical cancer screening program.PEI Pap Screening Program, 2001 Report6
PEI Pap Screening Program, 2001 Report-peer educ.-minorities-Nurse pract. inN. Ontario-immigrant &-5 PHN trainedto provide paps-communityfacilitators-honorariumfor WWC-reg. resourcenetwork Recruitment initiativesSource: CCPN Meeting, January 2001TTTTT Educational Resources(Spring 2001)websiteT(Oct 1999)T WebsiteT(Oct 1997) Education for ProfessionalsEducation and Recruitment: Pap Awareness CampaignT(Oct 2000)MD Training Standards Treatment OptionsT Letters to-asian &-aboriginal &-correct. facilitywebsiteT BCCAgencyTMD since’96TT Letters toevery 2yrT(Walton)T(1976) Program follow-up of abnormalpapsannual1949Dr. JasenkaMatistic2000EileenBellTBCALTApilotevery 2yr(Bethesda)SASKTevery 2yr(2001pilot-letters MDs)(Bethesda)Use MDbilling2000BrennaShearerHood1998Maureen Cava1996-40% ofpaps2000-85% ofpapsMANONT Program Report includingperformance IndicatorsPilot inMontr(16labs)QUannualevery 2 yrQuality Assurance: Screening GuidelinesT(1999 pilotletters &)T1996-88%(3yr backlog)NBannualT(Walton)(Bethesda)TTT Population database(for individual recruitment) Recall system to MD’s foroverdue paps Colposcopy data(follow-up linked with cytology) Histology database(diagnosis linked with cytology)(1988)(1996)TTTInformation Systems: Cytology database(provides &’s screening history)2002 MillanOrganization:Program start date, CoordinatorNFNSPEISCREENING ACTIVITYTable 2.1Provincial Screening Activity, January 20017
3.PEI PAP SCREENING PROGRAMThe inaugural meeting of PEI Pap Screening Advisory Committee was held onJanuary 16, 2001. Structure of the program as recommended by the Committee wasapproved by the Hon. Jamie Ballem, Minister of Health and Social Services, onMarch 21, 2001.3.1Program StructureThe program structure described below was designed to provide coordination to thediverse responsibilities and interests in cervical cancer, and to provide accountability.PEI Pap Screening Program, 2001 Report8
The Pap Screening Advisory Committee provides recommendations in thedevelopment, implementation, and direction of the PEI Pap Screening Program.Members include representatives from the Department of Health and Social Services,the PEI Breast Screening Program, the Provincial Pathology Laboratory, the PEIDivision of the Canadian Cancer Society, the Medical Society of PEI, and theWomen’s Network. Program activities are carried out by many parts of the healthsystem, with additional initiatives developed by working groups and overseen by thePap Screening Advisory Committee.The working groups established initially include the Recruitment Working Group, PapAwareness Working Group, Screening Guidelines Working Group, Cytology RegistryWorking Group, and Performance Indicators Working Group. The Terms ofReference for the Advisory Committee and Working Groups are found in Appendix G.3.2Program GoalsAs approved by the Pap Screening Advisory Committee on January 16, 2001, thegoals of the PEI Pap Screening Program are:CTo reduce the incidence and mortality rates associated with cervical cancer inPrince Edward Island.CTo recommend appropriate practices covering all areas of an organized papscreening program which includes recruitment, screening guidelines,computerized cytology registry, quality assurance, evaluation, follow-upnotification and educational resources.CTo identify and overcome barriers which prevent regular Pap screening amongwomen in PEI and to identify and implement incentives which encourageregular screening.CTo increase public knowledge of the need for regular Pap tests as apreventative health care measure and ensure sustainability of Pap AwarenessWeek Campaign.CTo increase awareness among health professionals of the need for regular Papsmears as a preventative health care measure.PEI Pap Screening Program, 2001 Report9
4.PROGRAM INDICATORS forPEI PAP SCREENINGThe program indicators available for this report are statistical measures of programperformance. These indicators can be used to inform policy decisions, to assessprogram effectiveness, and to compare with other jurisdictions.The indicators presented in this first report include: Provincial participation rates for PEI Specimen adequacy Cytology results Follow-up recommendations Incidence of cervical cancer Mortality of cervical cancerAdditional detailed data on the indicators presented in this section are found inAppendix H. The primary source of laboratory data is described in Appendix I.4.1Provincial Participation Rates for PEIParticipation in Pap screening programs are traditionally reported on an annual basis,to correspond with most physician recommendations. However, as organizedscreening programs are developing in Canada, there is interest in participation ratesthat correspond with provincial recommendations of every two years, and withnational recommendations of every three years.Table 4.1 provides the most recent provincial screening rates for all three screeningintervals. These rates are monitored for women aged 20-69, since not all womenunder 20 or over 69 require screening. Table 4.1 also demonstrates that participationin Pap screening decreases with age, regardless of the screening interval.Table 4.1PEI Pap Screening Rates, periods ending 2001(Population percent by age group)Screening PeriodOne year(2001)Two years(2000-2001)Three years(1999-2001)20 to 3445 %62 %69 %35 to 4942 %60 %67 %50 to 6939 %53 %57 %Total 20 to 6942 %58 %65 %Age groupPEI Pap Screening Program, 2001 Report10
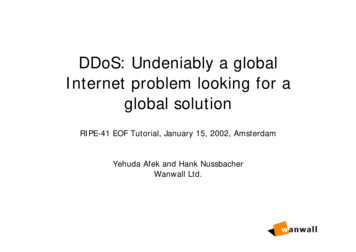
Figure 4.1PEI Pap Screening RatesFigure 4.1 demonstrates the stability of PEI’s annual screening rate. Each year,about 40% of PEI women between the ages of 20 and 69 were screened with a pap.This is similar to the rate described by Nova Scotia5, where a program to increasescreening was launched in 1991. British Columbia6 has the oldest establishedprogram, but publishes 30-month screening rates.Figure 4.1 also demonstrates the slight increasing trend in PEI’s three year screeningrates. In the most recent three year period, 65% of PEI women between the ages of20 and 69 were screened with a Pap. This is similar to the rate described by NovaScotia5 for 1995 to 1997. Participation rates described in this report tend to be moreaccurate than rates from surveys asking women to self-report their most recent paptest (see Appendix C). Most surveys of self-report provide socially desirableresponses that tend to over-report screening.Participation in Pap screening on PEI is far from complete. To improve this, theProgram will identify initiatives to increase regular screening of PEI women.5Statistical Report 1995 - 1997, NS Gynaecological Cancer Screening Programme, October 199962001 Annual Report, Cervical Cancer Screening Program, BCCA, 2001PEI Pap Screening Program, 2001 Report11
Table 4.2 demonstrates that participation in Pap screening varied by health region.The lower screening rates were seen in East Prince and West Prince. In all regions,the lowest screening rates are among women 50 and over. The screening rates inEast and West Prince also show low rates among women aged 35 to 49.Table 4.2PEI Pap Screening Rates, 3 year period ending 2001(by Health Region and age group)Health RegionAge groupWPEPQSKEK20 to 3470 %67 %70 %71 %74 %35 to 4959 %59 %70 %73 %70 %50 to 6944 %46 %63 %64 %64 %Total 20 to 6958 %58 %68 %69 %69 %# unscreenedwomen1,9714,5667,5801,442615Figure 4.2 provides a graphic depiction of the numbers of women eligible forscreening and actually screened, demonstrating the gap of unscreened women thatstill need to be encouraged in all health regions.Figure 4.2PEI Women eligible for Pap Screening68%58%58%PEI Pap Screening Program, 2001 Report69%69%12
4.2Specimen AdequacyCervical smears are classified in the laboratory on the basis of their adequacy forinterpretation: satisfactory, satisfactory but limited for interpretation, andunsatisfactory. Factors that limit the smear interpretation include blood, inflammation,poor fixation, contamination, or an inadequate number of cells. Table 4.3demonstrates that 0.2% of smears were unsatisfactory for interpretation in 2001.This is similar to the 0.3% in Nova Scotia5, and less than the 3% reported in BritishColumbia6.Table 4.3PEI Specimen Adequacy, by year(Rate per 1,000 Pap 3850872Satisfactory, but 121,73421,66221,99621,88522,995Total # Pap tests4.3Cytology ResultsThe diagnostic results of all satisfactory smears are presented in Table 4.4 Diagnosticcategories are based on the Bethesda classification. About 3% of Pap tests have aresult that involves low grade or high grade cellular changes. This is similar to the 2%in Nova Scotia5, and the 5% reported in British Columbia6 and Ontario7.Table 4.4PEI Cytology Results, 2001(Rate per 1,000 Pap tests, by age group)Age GroupCytology Result20 to 3435 to 4950 to 69Total 20 to 69946974986970432010249435Normal1Low Grade Changes2High Grade Changes1233includes changes within normal limits and benign cellular changesincludes LSIL, ASCUS, and AGUS non-suspiciousincludes HSIL, AGUS suspicious for malignancy, and carcinoma72000 CytoBase Report, Insctye Corp. 2001.PEI Pap Screening Program, 2001 Report13
4.4Follow-up RecommendationsThe laboratory report to the physician for each smear includes both the results and arecommended interval for follow-up. The follow-up may involve another pap test, orother investigations such as colposcopy, biopsy, or clinical treatment.Recommendations are based primarily on the current cytology result, but may also beinfluenced by the patient’s clinical condition and Pap test history. Table 4.5 presentsdetails of recommendations by cytology result.Table 4.5PEI Follow-up Recommendations, 2001Follow-up Recommendation(# of Pap tests)3 to 6 months12 months1.5 gh Grade Changes3120002Unsatisfactory291324Cytology ResultNormal1Low Grade Changes1232includes changes within normal limits and benign cellular changesincludes LSIL, ASCUS, and AGUS non-suspiciousincludes HSIL, AGUS suspicious for malignancy, and carcinomaOverall, the laboratory reports provided recommendations for 95% of the Pap tests.As expected, the majority of Pap tests with results of low or high grade changes hada recommended follow-up within 6 months. The majority of Pap tests with normalresults had a recommended follow-up interval of 12 months; this laboratory practiceshould be reviewed after the PEI Pap Screening Program adopts official screeningguidelines.PEI Pap Screening Program, 2001 Report14
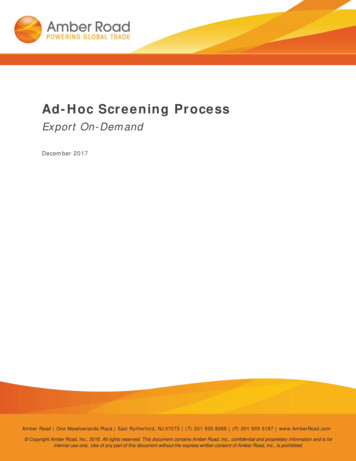
4.5Incidence of Cervical CancerTrends in Incidence - FemaleCervical CancerReduction of PEI’s incidence rate ofcervical cancer is a long-term goal ofthe program. However, in the next fiveyears, PEI can expect the rate tocontinue to increase as screeningfinds new cases.40Age-adjusted rate per 100,000In Canada, the incidence of new casesof cervical cancer has been declining.In PEI, however, the rate has beenincreasing, as shown in the figure tothe right. The most current estimate ofthe incidence rate is 13 new cases per100,000 PEI women,compared to 8 in Canada8. PEI hasconsistently had one of the highestrates of cervical cancer in Canada.302010083 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 OO OIYearPEIMortality of Cervical CancerIn Canada and PEI, the mortality rate forcervical cancer has been stable, asshown in the figure to the right. Themost current estimate of the mortalityrates are 3 deaths per 100,000 PEIwomen, compared to 2 in Canada8.The PEI program expects to maintainthe stable mortality rate, even asincidence increases, by ensuring followup. The long-term goal of the programis to reduce these preventable deaths.Trends in Mortality - FemaleCervical Cancer40Age-adjusted rate per 100,0004.6Canada302010083 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 OOO1Year8Canadian Cancer Statistics, Canadian Cancer Society & Health Canada, 2002PEI Pap Screening Program, 2001 Report15
5.PROGRAM ACTIVITIES IN 2001The activities of the PEI Pap Screening Program in 2001 were carried out by theProgram’s Working Groups (see section 3), and were coordinated by the PapScreening Advisory Committee.5.1Pap Awareness WeekPEI’s second Pap Awareness Week campaign was held October 20 to 27, 2001.This campaign was the result of a marketing strategy, coordination with campaigns inNova Scotia and Newfoundland, and evaluation of PEI’s 2000 campaign (seeAppendix F). The main focus of this campaign was a media blitz and promotionalmaterials with the key messages of: cervical cancer can be prevented a pap test every two years can save your life call your doctor or the Pap Screening Clinic for an appointmentTable 5.1 describes the campaign materials. The 2001 campaign maintained thevisual identity of PEI’s 2000 campaign.Table 5.1PEI Campaign Materials, 2001MaterialDescriptionDistributionTV Commercialthree generations ofwomen on the TC trail(produced in 2000)50 Prime Time airings on CBC for Oct23 - Nov 6; repeated for 2 weeks inJanuary 2002RadioCommercial3 scripts with young,middle aged, and olderwomen21 ads per week on CFCY, CHTN,Magic 93, C102 for October 22 - Nov12; repeated for 3 weeks in January2002Brochure“You can preventcervical cancer”(updated in 2001)16,000 to 80 physician offices, 44pharmacies, 30 health organizationsPoster“You can preventcervical cancer”600 to physician offices, pharmacies,health organizations, 8 malls, 41grocery storesPocket Calendars“You can preventcervical cancer”15,000 to malls, grocery stores, 210hairdressers, 11 fitness centres, largeemployers, 70 school staff rooms, 20librariesOther activities included notices in church bulletins, and a press release (shortly afterthe Minister’s press conference for the opening of the Pap Clinic).PEI Pap Screening Program, 2001 Report16
5.2Cytology LaboratoryPEI has one centralized laboratory for the interpretation of smears located at theQueen Elizabeth Hospital. Pathologists also provide histology results at this hospital,and the Prince County Hospital.Cytology and histology results in PEI were computerized using the Laboratory CaseManagement System (LCMS), developed in 1996. The LCMS produces: case reports for each cytology and histology specimen annual summaries of Pap test adequacy for each physician laboratory summary of correlation between cytology and histology reports data for the Pap Screening Program’s performance indicators(see Appendix I).Upgrades to the system are underway to allow for additional summa
The program indicators available in this report are statistical measures of program performance that can be used to inform policy decisions, and to assess program effectiveness. The PEI Pap Screening Program encourages regular screening at least every two years. PEI's overall two year screening rate during 2000-2001 for women aged 20 to 69 .