Transcription
Fracture Testing of a Self-Healing Polymer Compositeby E.N. Brown, N.R. Sottos and S.R. WhiteABSTRACT—Inspired by biological systems in which damagetriggers an autonomic healing response, a polymer composite material that can heal itself when cracked has been developed. In this paper we summarize the self-healing conceptfor polymeric composite materials and we investigate fracture mechanics issues consequential to the development andoptimization of this new class of material. The self-healingmaterial under investigation is an epoxy matrix composite,which incorporates a microencapsulated healing agent thatis released upon crack intrusion. Polymerization of the healing agent is triggered by contact with an embedded catalyst.The effects of size and concentration of the catalyst and microcapsules on fracture toughness and healing efficiency areinvestigated. In all cases, the addition of microcapsules significantly toughens the neat epoxy. Once healed, the self-healingpolymer exhibits the ability to recover as much as 90 percentof its virgin fracture toughness.KEY WORDS—Self-healing, autonomic healing, fracturetoughness, microcapsule toughening, tapered doublecantilevered beam, brittle fracture of epoxyIntroductionFracture of the skeletal structure in biological systems provides an excellent model for developing a synthetic healingprocess for structural materials. For a bone to heal, nutrientsand undifferentiated stem cells must be delivered to the fracture site and sufficient healing time must elapse.1 The healingprocess consists of multiple stages of deposition and assembly of material,2 as illustrated in Fig. 1. The network of bloodvessels in the bone is ruptured by the fracture event, initiatingautonomic healing by delivering the components needed toregenerate the bone.In recent breakthrough research, White et al.3 have developed a self-healing polymer that mimics many of thefeatures of a biological system. The self-healing system,shown schematically in Fig. 2, involves a three-stage healingprocess, accomplished by incorporating a microencapsulated healing agent and a catalytic chemical trigger in anepoxy matrix. A conclusive demonstration of self-healingwas obtained with a healing agent based on the ring-openingmetathesis polymerization (ROMP) reaction. Dicyclopenta-diene (DCPD), a highly stable monomer with excellent shelflife, was encapsulated in microcapsules with a thin shell madeof urea-formaldehyde. A small volume fraction of microcapsules was dispersed in a common epoxy resin along with theGrubbs ROMP catalyst, a living catalyst that remains activeafter triggering the polymerization. The embedded microcapsules were shown to rupture in the presence of a crack andto release the DCPD monomer into the crack plane. Contactwith the embedded Grubbs catalyst initiated polymerizationof the DCPD and rebonded the crack plane. Crack healingefficiency, η, is defined as the ability of a healed sample torecover fracture toughness4η KI chealed,KI cvirgin(1)where KI Cvirgin is the fracture toughness of the virgin specimen and KI Chealed is the fracture toughness of the healedspecimen. Fracture test results using the ROMP-based healing system revealed that, on average, 60 percent of the fracturetoughness was recovered in the healed samples.Crack healing phenomena have been discussed in the literature for several types of synthetic materials including glass,concrete, asphalt and a range of polymers.4 22 While theseprevious works have been successful in repairing or sealingcracks, the healing was not self-initiated and required someform of manual intervention (e.g., application of heat, solvents, or healing agents). Others have proposed a tube delivery concept for self-repair of corrosion damage in concreteand cracks in polymers.23 25 While conceptually interesting,the introduction of large hollow tubes in a brittle matrix material causes stress concentrations that weaken the material,and beneficial healing may be difficult to realize.25In contrast, the microcapsule concept developed by Whiteet al.3 is particularly elegant and promising for healing brittle,thermosetting polymers. In this paper, we present a comprehensive experimental investigation of the correlative fractureand healing mechanisms of this self-healing system. The effects of microcapsule concentration, catalyst concentrationand healing time are studied with a view towards improvinghealing efficiency.Experimental ProcedureEric N. Brown is a Doctoral Candidate and Nancy R. Sottos is a Professor,Department of Theoretical and Applied Mechanics and Beckman Institutefor Advanced Science and Technology, 216 Talbot Laboratory, 104 SouthWright Street Urbana, IL 61801. Scott R. White is a Professor, Departmentof Aerospace Engineering and Beckman Institute for Advanced Science andTechnology, 306 Talbot Laboratory, 104 South Wright Street, Urbana, IL61801.Original manuscript submitted: February 26, 2002.Final manuscript received: August 6, 2002.372 Vol. 42, No. 4, December 2002Using the protocol established by White et al.,3 healingefficiency is measured by carefully controlled fracture experiments for both the virgin and the healed materials. Thesetests utilize a tapered double-cantilever beam (TDCB) geometry, which ensures controlled crack growth along the centerline of the brittle specimen. The TDCB fracture geometry,developed by Mostovoy et al.,26 provides a crack length independent measure of fracture toughness
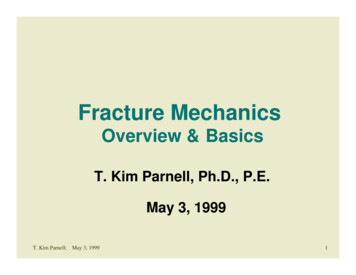
ntFig. 1—Healing stages of bone: (a) internal bleeding, forminga fibrin clot; (b) unorganized fiber mesh develops; (c) calcification of the fibrocartilage; (d) calcification converted intofibrous bone; (e) transformation into lamellar bone KI c 2Pcm,βwhich requires knowledge of only the critical fracture loadPc and geometric terms m and β. The value of β depends onthe specimen and crack widths b and bn , respectively. Thevalue of m is defined by the theoretical relationm 3a 2h(a)3 1,h(a)PolymerizedHealing Agent(2)Fig. 2—Self-healing concept for a thermosetting polymer(3)or determined experimentally by the Irwin-Kies27 methodwherem Eb dC.8 daPchealed.Pcvirgin21.8º(4)Young’s modulus is given by E, C is the compliance, a isthe crack length from the line of loading, and h(a) is thespecimen height profile. For the TDCB sample geometry, thehealing efficiency (eq (1)) is rewritten asη bn 2.525.4(5)TDCB SpecimenValid profiles for a TDCB fracture specimen are determined by finding a height profile that, when inserted intoeq (3), yields a constant value of m over a desired rangeof crack lengths. Height profiles that provide an exact solution are complex curves, but are approximated with lineartapers.12,26,28,29 In the current work, we adopt a modifiedversion of the TDCB geometry developed and verified byBeres et al.28 Relevant dimensions are shown in Fig. 3.When the taper angle is small, a crack propagating in abrittle material exhibits a propensity to deflect significantlyfrom the centerline. Failure commonly occurs as arm breakoff. To ensure fracture follows along the desired path, sidegrooves are incorporated into the TDCB geometry. The addition of side grooves is valid for the TDCB geometry, asthere is no restriction that b and bn be the same. Stable crackpropagation with maximum crack width, bn , is obtained byselecting a groove with 45 internal angle.30 For this particular geometry, the geometric term β in eq (2) is given by31β b0.61 bn0.39 .ah(a)61 2831.759245º76.2b 6.25Fig. 3—TDCB geometry (dimensions in mm)A series of 18 fracture toughness tests was performedon pure epoxy (EPON 828/DETA) TDCB specimens withcrack lengths ranging from 20 to 37 mm to determine mfrom eq (4). A plot of compliance versus crack length wasconstructed and a linear fit made, extrapolating a constantvalue of dC/da. The fracture toughness of the neat epoxyand the geometric constant m were measured to be 0.55 MPam1/2 and 0.6 mm 1 . This experimental value of m is in excellent agreement with the value predicted by the finite elementmethod (FEM).28 The Young’s modulus of the epoxy wasmeasured according to the American Society for Testing andMaterials (ASTM) Standard D 638, E 3.4 0.1 GPa.Sample Preparation and Test MethodSamples were prepared by mixing EPON 828 epoxyresin with 12 pph Anacmine DETA curing agent. The epoxyExperimental Mechanics 373
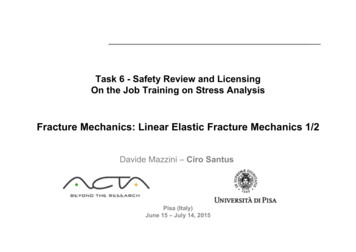
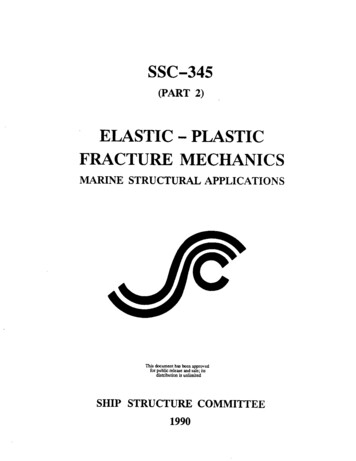
Healing of the Reference SystemThe healing system was first investigated via fracturetoughness testing of reference samples. Following a virgin fracture test, approximately 0.03 ml of mixed DCPDmonomer and catalyst was injected into the crack plane. Anadvantage of the ROMP healing system is the heterogeneousnature of the reaction. Unlike two part epoxy polymerization reactions, which require a precise stoichiomerty ratio,the ROMP reaction can be triggered by discrete mixing atlow concentration (10,000:1 monomer to catalyst ratio).374 Vol. 42, No. 4, December 200260η 90.3%50Load (N)mixture was degassed, poured into a closed silicone rubbermold and cured for 24 h at room temperature, followed by24 h at 30 C. After curing, a sharp pre-crack was createdby gently tapping a razor blade into the molded starter notchin the samples. To facilitate investigation of the effects ofthe constituents on the self-healing system, varying weightpercent of Grubbs catalyst and/or microcapsules were mixedinto the resin prior to pouring.Three types of experiments were conducted: two types ofcontrol in addition to the self-healing in situ tests. The firsttype of control, referred to as reference samples, consisted ofepoxy without embedded catalyst. Reference samples witha range of microcapsule concentrations were investigated;however, the content of the microcapsules in these sampleswas not utilized for the healing process. Reference sampleswere tested to failure and then manually healed by injection ofDCPD monomer that was pre-mixed with catalyst. Referencetests removed the variables associated with DCPD deliveryand the embedding of Grubbs catalyst. The second control,referred to as self-activated samples, consisted of epoxy withembedded catalyst but no microcapsules. Self-activated samples were tested to failure and then healed by manual injectionof DCPD monomer into the crack plane. This intermediatelevel control test enabled investigation of the embedded catalyst, without the variability of DCPD delivery through microencapsulation. The third type of sample was the fully selfcontained, or in situ, system. In situ samples contained boththe microencapsulated healing agent and Grubbs catalyst, enabling them to self-heal after fracture. Urea-formaldehydemicrocapsules containing DCPD monomer were manufactured by an emulsion microencapsulation method outlined inWhite et al.3 Table 1 summarizes the different sample types.Fracture specimens were tested under displacement control, using pin loading and a 5 µm s 1 displacement rate.Samples were tested to failure, measuring compliance andpeak load. For the reference samples, 0.03 ml of pre-mixedDCPD monomer and Grubbs catalyst was injected into thecrack plane, prior to crack closing. For the case of selfactivated samples, 0.03 ml of DCPD monomer with no catalyst was injected into the crack plane, which was subsequently allowed to close. In situ samples were unloaded, allowing the crack faces to come back into contact. After asufficient time for healing efficiency to reach a steady value,the healed samples were tested again. For the majority of experiments, the second test was performed after 48 h. Valuesof fracture toughness and the subsequent healing efficiencywere calculated using eqs (2) and (5). A representative loaddisplacement curve is shown in Fig. 4 for the in situ healingcase. The virgin fracture was brittle in nature, while the healedfracture exhibited prolonged stick-slip.Stick-Slip Failure4030Healed20Virgin1000250500750 1000Displacement (µm)12501500Fig. 4—Representative load-displacement curve for an insitu sample with 2.5 wt% Grubbs and 5 wt% microcapsulesCatalyst ConcentrationThe effect of the ratio of Grubbs catalyst to DCPDmonomer was investigated by measuring the healing efficiency in four sets of samples with catalyst to DCPD ratiosof 2, 4.4, 10 and 40 g liter 1 . Each set consisted of 18 samples. As shown in Table 2, the level of healing efficiency increased as the concentration of catalyst was increased, whilethe gel time decreased exponentially, taking approximately,600, 235, 90 and 25 s, respectively.An investigation of the fracture planes highlights two phenomena: fracture in pure epoxy results in locally smooth surfaces down to micrometer length scales (Fig. 5(a)) and fracture in the healed material occurs as separation between thebulk epoxy and polyDCPD film (Fig. 5(b)). The increasedhealing efficiency is attributed to changes in the chemicalkinetics and thermodynamics with increased catalyst concentration. Shorter cure times reduce the time required forhealing efficiency to reach a steady value and prevent diffusion and evaporation of DCPD from the crack plane. Theability of the healed reference sample to obtain full healing(η 100 percent) indicates excellent adhesion between thepolymerized DCPD and the epoxy.Microcapsule ConcentrationReference samples have also been used to study the influence of microcapsule concentration on the fracture of thevirgin and healed epoxy. Reference samples containing 0–25 percent by weight of microcapsules ( 180 µm diameter)were tested to failure and healed manually. As observed earlier in the literature for the addition of solid particles,32,33the virgin fracture toughness of the material increased significantly with increasing concentration of microcapsules, asshown in Fig. 6. A maximum was achieved at 15 wt% capsule concentration. Characteristic tails originating from broken spheres in the fracture plane (Fig. 5(c)) indicate a crackpinning toughening mechanism may be operative.The healing agent released from the microcapsules was allowed to evaporate from the crack plane. The reference samples were then injected with a 4.4 g liter 1 mixture of Grubbscatalyst and DCPD monomer. The healed fracture toughness demonstrated minimal dependence on capsule concentration over a range of 5–20 percent by weight. For capsule
TABLE 1—SAMPLE TYPESSampleTypeReference controlSelf-activated controlIn situ self-healingEpoxy(Epon 828:DETA)100:12100:12100:12GrubbsCatalyst—0-5 %wt2.5 %wtMicroencapsulatedHealing Agent0-25 %wt—5-10 %wtTABLE 2—INFLUENCE OF CATALYST CONCENTRATION ON HEALING EFFICIENCY IN REFERENCE SAMPLESConcentrationFracture Toughness (MPa m1/2 )HealingGrubbs (g):DCPD (I)VirginHealedEfficiency40:10.55 0.050.71 0.08Full heal10:10.56 0.040.61 0.09Full heal4.4:10.55 0.050.53 0.1097 15%2:10.54 0.040.45 0.0884 8%concentrations close to the value that yields a maximum forthe virgin fracture toughness ( 15 wt%), a local minimumin healing efficiency occurred due to the minimal gains inhealed fracture toughness, illustrated in Fig. 7. For a capsuleconcentration of 25 wt% and greater, near perfect healing wasobtained. However, as the capsule concentration increased,the manufacture of samples was more difficult due to theincreased viscosity of the uncured resin.Healing of the Self-Activated SystemThe Grubbs catalyst is a fine purple powder with a propensity to form small clumps. Chemical investigation of the interactions between the catalyst and the epoxy system indicatesthat contact of the catalyst with the DETA curing agent candegrade the catalyst during manufacture.34 The availabilityof active catalyst is dependent on the order of mixing the catalyst, resin and curing agent, the catalyst particle size, and theamount of catalyst added. These parameters are investigatedwith self-activated samples.Mixing OrderThe stability of the Grubbs catalyst in the current healing system was investigated previously using proton nuclearmagnetic resonance (NMR)34 (a standard technique for probing chemical structures35 ). Although the Grubbs catalyst retained activity in the presence of the EPON 828/DETA system during cure, contact with the DETA curing agent alonecaused rapid deactivation of the catalyst. To ascertain theoptimal mixing sequence of the three components (EPON 828/12pph DETA/2.5 wt% Grubbs catalyst) for maximumcatalyst activity and healing efficiency, six self-activated samples were manufactured for each of the three possible sequences. In each case, the first two components were mixedand degassed for 5 min. The third component was then integrated and degassed for an additional 5 min.Fracture test results for the different mixing sequences aresummarized in Table 3. Although virgin fracture toughnessvalues are statistically unchanged, the healed fracture toughness values and in turn the efficiency of healing indicate theimportance of mixing order. Mixing the catalyst and DETAcuring agent first results in no measurable healing. Failure torecover fracture toughness indicates that the catalyst was extensively deactivated. The other two mixing orders had littleeffect on the healing efficiency.Catalyst Particle SizeThe size of the Grubbs catalyst particles also influencedthe behavior of the virgin and healed composites. To determine the size distribution of the catalyst for maximum healingefficiency, a sample of catalyst was ground to provide a powder with particle diameters of less than 1 mm. Sets of sixself-activated samples were manufactured with 2.5 wt% ofcatalyst with distributions of particle sizes of less than 75 µm,75–180 µm, 180-355 µm and 355–1000 µm (Fig. 8). Boththe virgin and healed fracture toughness values, plotted inFig. 9, increased as the catalyst particle size increased. Poorhealing efficiencies were obtained for small particles, due tolow healed fracture toughness, and for large particles becausethe high healed fracture toughness was not coterminous withtheir high virgin fracture toughness. The highest healing efficiency corresponded to 180–355 µm catalyst particle size.In the virgin material, the catalyst particles toughenthrough crack pinning,36 as shown in Fig. 5(d). In the healedmaterial, there are the competing effects of smaller particlesproviding improved dispersion—and thus availability of catalyst in the crack plane for polymerization of DCPD—and oflarger particles providing a reduced surface area to volumeratio for the catalyst. The smaller surface area to volume ratiois believed to reduce the opportunity for DETA curing agentto react with the Grubbs catalyst.Catalyst ConcentrationTo establish the catalyst concentration that provides forhigh healing efficiency without diminishing virgin fracturetoughness, six sets of self-activated TDCB samples weremanufactured with Grubbs catalyst concentrations from 0wt% to 4 wt%. Each set consisted of six samples. Virgin andhealed fracture toughness values and the corresponding healing efficiency have been measured and are plotted in Fig. 10.The healed fracture toughness increased with the addition ofmore catalyst. However, the relative gain in healed fracturetoughness actually decreased for each additional incrementof catalyst concentration. For a catalyst concentration beyond3 wt%, the virgin fracture toughness decreased with furtheraddition of catalyst. Although a high healing efficiency resulted at these high catalyst concentrations, gains were dueto diminution of the virgin properties. Moreover, scatter inthe data was dramatically increased at higher concentrations.Experimental Mechanics 375
TABLE 3—INFLUENCE OF MIXING ORDER ON HEALING EFFICIENCY IN REFERENCE SAMPLESFracture Toughness (MPa m1/2 )Mixing OrderVirginHealed(Epon 828 DETA) Grubbs0.73 0.060.45 0.08(Epon 828 Grubbs) DETA0.75 0.050.45 0.09(DETA Grubbs) Epon 8280.76 0.070Self-Healing of the In Situ SystemThe ultimate goal of this research was the developmentof a self-healing polymer composite. To achieve this, microencapsulated DCPD monomer and Grubbs catalyst wereincorporated into an in situ sample. The effects of microcapsule size on healing efficiency and the evolution of healedfracture toughness over time were investigated using in situsamples with 2.5 wt% Grubbs catalyst and 10 wt% of DCPDmonomer encapsulated microcapsules. The findings of thesestudies and the results presented thus far have been used tooptimize the healing system through choice of catalyst andmicrocapsule concentration.Microcapsule SizeThree sets of samples were manufactured with 180 40 µm, 250 80 µm and 460 80 µm diameter capsules.When fracture occurred, DCPD monomer was observed tofill the crack plane of the TDCB specimen. Variation in thehealed fracture toughness was small, with a trend for increased toughness with decreased capsule diameter as shownin Fig. 11. The divergence of healing efficiency was governedby the virgin fracture toughness, which increased significantly with decreased capsule diameter. The self-healed specimens with 460 µm diameter capsules exhibited the greatesthealing efficiency, recovering 63 percent of virgin load onaverage. An investigation of the crack planes (Fig. 5(e)) revealed that all of the microcapsules fractured, releasing theencapsulated healing agent, with no mounds or protrudingshell material representative of debonding.Development of Healing EfficiencyThe healing efficiencies presented thus far were measured after waiting 48 h after the virgin test. This time waschosen to ensure sufficient time for healing. Previous workwith thermoplastics4 6 reported that healing efficiency wasstrongly tied to healing time. A series of 28 in situ sampleswas manufactured with 10 wt% of 180 µm diameter capsulesand 2.5 wt% of catalyst. The virgin fracture tests were performed in rapid succession with the exact time of the fractureevent noted for each specimen. Healed fracture tests were performed at time intervals ranging from 10 min to 72 h after thevirgin test. The resulting healing efficiencies are plotted versus time in Fig. 12. A significant healing efficiency developedwithin 25 min, which closely corresponds to the gelation timeof the polyDCPD. Steady-state values were reached within10 h.Microcapsule ConcentrationIn previous work on this self-healing system,3,37 microcapsule concentration was chosen to be 10 wt% to maximizeDCPD delivery, while retaining near maximum virgin fracture toughness. For the large range of microcapsule sizes in376 Vol. 42, No. 4, December 2002HealingEfficiency63 6%60 6%0%vestigated in Fig. 11, only a small change in healed fracturetoughness was measured. Excess DCPD was also observedduring fracture for all capsule sizes. Moreover, the data forreference samples in Fig. 6 showed that a reduction in concentration from 10 wt% to 5 wt% had minimal impact on thehealed fracture toughness. By reducing the capsule concentration, near perfect healing was obtained.To investigate this effect for the self-healing case, a set ofsix in situ samples was manufactured with 5 wt% of 180 µmdiameter capsules and 2.5 wt% of catalyst. An average healing efficiency of 85 5% was measured. The relative healingefficiencies of neat epoxy and the in situ system with 10 wt%and 5 wt% microcapsules, are shown in Fig. 13, illustrating the successful development of an optimized self-healingsystem.ConclusionThe use of TDCB fracture geometry has provided an accurate method to measure the fracture behavior and healingefficiency of self-healing polymer composites and to compare with appropriate controls. Virgin fracture properties ofthe polymer composite were improved by the inclusion ofmicrocapsules and catalyst particles. The size and concentration of the catalyst were shown to have a significant impacton the virgin properties of the composite and the ability tocatalyze the healing agent. The highest healing efficiencywas obtained with 180–355 µm catalyst particles. Catalystconcentrations of greater than 2.5 wt% provided diminishinggains in healed fracture toughness. A significant loss of virginfracture toughness was observed for a catalyst concentrationof about 3%. The catalyst was found to remain active following the curing process, given that it was not first mixed withthe DETA curing agent. The addition of microcapsules, upto 15 wt%, served to increase the virgin toughness. Capsulesize had a direct influence on the volume of DCPD monomerreleased into the crack plane but, over the range of capsulesizes investigated, healing efficiency was not restricted bylack of healing agent. Maximum healing efficiency was obtained within 10 h of the fracture event. By optimizing theconcentrations of catalyst and microcapsules, the healing efficiency of the system was increased to over 90 percent.AcknowledgmentsThe authors gratefully acknowledge the support of theUniversity of Illinois Critical Research Initiative Program,AFOSR Aerospace and Materials Science Directorate Mechanics and Materials Program, and Motorola Labs, Motorola Advanced Technology Center Schaumburg IL. Specialthanks are extended to Dr A. Skipor of Motorola Labs forhis continuing support and suggestions. The authors wouldalso like to thank Prof. J.S. Moore, Prof. P.H. Geubelle andgraduate students M.R. Kessler and S.R. Sriram for technicalsupport and helpful discussions. Undergraduate B. Lung was
a.Fracture Toughness1/2(K Ic, MPa m )1.5Virgin10.5005101520Capsule Concentration (wt%)25Fig. 6—Virgin and healed fracture toughness as a function ofcapsule ng Efficiency(%)10080604020005101520Capsule Concentration (wt%)25Fig. 7—Healing efficiency as a function of capsuleconcentrationGrubbspolyDCPDe.Fig. 5—Crack plane environmental scanning electron microscopy (ESEM) images: (a) neat epoxy; (b) polyDCPD separation from bulk epoxy; (c) reference sample (10 wt% capsules) showing tails related to the crack pinning tougheningmechanism; (d) self-activated (2.5 wt% Grubbs catalyst); (e)in situ samples (10 wt% capsules and 2.5 wt% catalyst). Thecrack propagation direction is from left to right in all imagesNormalized Distribution (%)d.403020100 7575-180180-355Catalyst Size ( µm)355-1000Fig. 8—Particle size distribution of the Grubbs catalystfollowing grindingExperimental Mechanics 377
708060Virgin0.8400.60.4200.2Healed00 75Fig. 9—The effect of catalyst particle size on fracturetoughness and healing efficiencyVirgin0.4 Healed0.31000.2500.10Healing Efficiency (%)Fracture Toughness1/2(MPa m )0.5000.5 1 1.5 2 2.5 3 3.5Catalyst Concentration (wt%)5040Healed0.6300.420Neat Epoxy0.2Resin1070Healing Efficiency (%)1500.60.8Fig. 11—Influence of microcapsule size on fracture toughness and healing efficiency2000.7Virgin00100 200 300 400 500 600 Self-Activated700 800 900Mean Capsule Diameter (µm)75-180 180-355 355-1000Catalyst Size (µm)0.8601Healing Efficiency (%)1Fracture Toughness1/2(MPa m )1.2Healing Efficiency (%)Fracture Toughness1/2(MPa m )1.2504030201004Fig. 10—Fracture toughness and healing efficiency as afunction of catalyst concentration6001020304050Healing Time (hr)6070Fig. 12—Development of healing efficiencyReferences1. Caplan, A.I., “Bone Development, Cell and Molecular Biology ofVertebrate Hard Tissues,” Ciba Foundation Symposium, 136, 3–16, JohnWiley & Sons (1988).2. Albert, S.F., “Electrical Stimulation of Bone Repair,” Clin. PodiatricMed. Surg., 8, 923–935 (1981).3. White, S.R., Sottos, N.R., Geubelle, P.H., Moore, J.S., Kessler, M.R.,Sriram, S.R., Brown, E.N., and Viswanathan, S., “Autonomic Healing ofPolymer Composites,” Nature, 409, 794–797 (2001).4. Wool, R.P., and O’Conner, K.M., “A Theory of Crack Healing in Polymers,” J. Appl. Phys., 52, 5953–5963 (1982).5. Jud, K., and Kausch, H.H., “Load Transfer Through Chain MoleculesAfter Interpentration at Interfaces,” Polym. Bull., 1, 697–707 (1979).6. Kausch, H.H., and Jud, K., “Molecular Aspects of Crack Formationand Healing in Glassy Polymers,” Rubber Process. Appl., 2, 265–268 (1982).7. Sukhotskaya, S.S., Mazhorava, V.P., and Terekhin, Yu N., “Effect ofAutogenous Healing of Concrete Subjected to Periodic Freeze Thaw,” Hydrotech. Constr., 17, 295–296 (1983).8. Clear, C.A., “The Effect of Autogenous Healing upon Leakage of Waterthrough Cracks in Concrete,” Cement and Concrete Association, WexhamSpring, May (1985).9. Edvardsen, C., “Water Permeability and Autogenous Healing ofCracks in Concrete,” ACI Mater. J., 96, 448–454 (1999).378 Vol. 42, No. 4, December 2002Healing Efficiency (%)100extremely helpful in the preparation of the TDCB samples.Electron microscopy was performed in the Imaging Technology Group, Beckman Institute, of the University of Illinois,with the assistance of S. Robinson.806040200NeatEpoxyIn-SituInSitu10 wt%CapsulesIn-SituInSitu5 wt%CapsulesFig. 13—Comparison of in situ healing efficiency for differentcapsule concentrations (2.5 %wt catalyst)10. Kim, Y.R., and Little, D., “Evaluation of Self-Healing in AsphaltConcrete by Means of the Theory of Nonlinear Elasticity,” Transp. Res.Rec., no. 1228, 198–210 (1989).11. Stavrinidis, B., and Holloway, D.G., “Crack Healing in Glass,” Phys.Chem. Glasses, 24, 19–25 (1983).12. Jung, D., “Performance and Properties of Embedded Microspheresfor Self-Repairing Applications,” MS Thesis, University of Illinois atUrbana-Champaign (1997).
13. Hegeman, A., “Self-repairing Polymers, Repair Mechanisms andMicromechanical Modeling,” MS Thesis, University of Illinois at UrbanaChampaign (1997).14. Jung, D., Hegeman, A., Sottos, N.R., Geubelle, P.H., and White, S.R.,“Self-healing Composites Using Embedded Microspheres,” Proc. AmericanSociety for Mechanical Engineers (ASME), Symposium on Composites andFunctionally Graded Materials, Dallas, TX, eds. K. Jacob, N. Katsube andW. Jones, ASME, MD-80, 265–275 (1997).15. Zako, M., and Takano, N., “Intelligent Material Systems Using EpoxyParticles to Repair Microcracks and Delamination Damage in GFRP,” J. Intell. Mater. Syst. Struct., 10, 836–841 (1999).16. Wiederhorn, S.M., and Townsend, P.
The healing system was first investigated via fracture toughness testing of reference samples. Following a vir-gin fracture test, approximately 0.03 ml of mixed DCPD monomer and catalyst was injected into the crack plane. An advantage of the ROMP healing system is the heterogeneous nature of the reaction. Unlike two part epoxy polymeriza-