Transcription
Journal of Applied Dental and Medical SciencesNLM ID: 101671413 ISSN:2454-2288Volume 4 Issue1 Jan-March 2018Review ArticleARCHFORM IN ORTHODONTICS: A REVIEWAmit Tiwari1, Ashish Garg2 , Bhavna Virang3, Samprita Sahu4, Neetu Shah5, Nikhil Verma61,2,3,4,5,6ARTICLE INFOMDS, Sri Aurobindo College of Dentistry, Indore(M.P.)ABSTRACTDental arch form is the arch, formed by the buccal and facial surfaces of the teeth when viewed from theirocclusal surfaces. The universal ideal arch form is one of the most persistent but exclusive task for most ofthe orthodontic researchers have. Concerning the orthodontic treatment, basic principle of arch form in isthat within reason, the patients original arch from should be preserved. Therefore, if the preformed archwires are to be used, it is to be kept in the mind that their shape should be considered a starting point forthe adjustment necessary for proper individualization as all the presently available preformed arch wire donot reflect these variations in the arch form. Because of these complex problems, and relatively lowknowledge of dental arches, as of today, there is no universally accepted ideal arch form. The presentarticle gives the review about the changes in the concept of arch form from conventional era to modernKeywords:practice.Dental arch form, orthodontic treatmentIntroductionPercy N. William (1917)2 conducted a study toDental arch form is the arch, formed by the buccal anddetermine the shape of normal dental arch. Hefacial surfaces of the teeth when viewed from theirbelieved that arch form does not correlate with facialocclusal surfaces. It is commonly believed that thepattern. He did not agree that a round face indicated adentalby theround arch or a narrow face a narrow arch, etc. Heconfiguration of supporting bone. Following eruptiondisproved it by sending photographs of an individualof teeth and by circum oral musculature and intra oralalong with a set of artificial teeth to ten of the leadingfunctional forces.practitioners of time, and asked them to arrange theHRDLICKA A. in 19161 conducted a study onteeth in an arch according to type. He received widelynormal dental arch and concluded that there is no suchvaryingthing in existence, in any race that we know of, as onepractitioners had their own concept of what an idealsingle normal dental arch; that in every race, and evenarch should look like which had no relation to theunder most normal conditions, we find a variety offacial type of the patient.arches which must be considered as normal arches andHe concluded from his studies that the front teethclose attention should be paid to these fact as it hasshould be arranged on a circle whose center is midwaydirect bearing on intelligent treatment of the patient.between the buccal grooves of the first molars. HeIdeal arch form-also believed that the ratio of the widths between * Corresponding author: Dr. Amit Tiwar, Sri Aurobindo College of Dentistry, Indore(M.P.), Email.add. dr.meet7590@gmail.comthatmany
ARCHFORM IN ORTHODONTICS 4(1);2018119first molars and the cuspids should be maintained atGeorge C. Chuck(1934)6 conducted a study on idealapproximately 14 to 9.arch form and suggested that using the Bonwil1-McCoy J D (1919)3 conducted a study on normal archHawley arch as an aid in constructing a symmetricallyform and agreed with the concept of William that archformed alignment arch wire which could then beform was not dependent on facial type. He felt thataltered according to the type of the individual, whilecareful observation would convince anyone to discardmaintaining the symmetry of the arch wire.the theory that nature always produces teeth inHassan Noroozi, Tahereh Hosseinzadeh Nik, Rezaharmony with face and features. He used as evidenceSaeeda, BS (2001) revisited the dental arch form. Inseveral skulls which he claimed showed no relation oftheir research, they tried to find the equation of athe forms of the teeth to the shapes or sizes of thecurve that would be similar to the generalized betaskulls.methods of archfunction curve and at the same time could representpredetermination, he stated that use of any of thetapered, ovoid, and square dental arches. A total of 23methods which were based on the amount of toothsets of naturally well-aligned Class I casts weresubstance contained within the arch, along withselected, and the depths and widths of the dentalrecognized anatomic principles, would render aarches were measured at the canine and second molargreater service than the operator depending on hisregions. Using the mean depths and widths, functions"Eagle Eye'" to guide him on his way.in the form of Y AXm BXn were calculated thatFrederick L. Stanton (1922)4 devised a method ofwould pass through the central incisors, canines, anddetermining the ideal form of the arches of each casesecond molars. Each function was compared with thestudied by using a map of the malocclusion and angeneralized beta function with the use of root mean“occlusal graph”, and then placing the teeth on chartssquare values. It was shown that the polynomialin a manner to assure the best occlusion with thefunction Y AX6 BX2 was the nearest to theminimum tooth movement.generalized beta function. Then the coordinates of theHowever, G. Izard (1927)5 believed that themid-incisal edges and buccal cusp tips of each dentaldimensions of the dental arch were governed by thearch were measured, and the correlation coefficient ofcorresponding dimensions of the face. A constant ratioeach dental arch with its corresponding sixth orderwas found to exist between the width of the maxillarypolynomial function was calculated. The resultsarch and width of the face, and between the length ofshowed that the function Y AX6 BX2 could be anthe arch and depth of the face. He established the formaccurate substitute for the beta function in lessof the maxillary arch as an ellipse, the large axis ofcommon forms of the human dental arch.which was determined by measuring the auriculo-Tarcila Trivino, Danilo Furquim Siqueira, and Marcoincisal radius with a radiometer and the small axis byAntonio Scanavini. (2008)8developed a new conceptmeasuring the bizygomatic distance with a largeof mandibular dental arch form with normal occlusioncompass and then subtracting the thickness of the softand concluded that the mandibular dental arch istissue.represented by 23 forms; thus, a normal dental archCommenting on thecannot be represented by only 1 simple arch form.Journal Of Applied Dental and Medical Sciences 4(1);20187
ARCHFORM IN ORTHODONTICS 4(1);2018120Shin-Jae Lee, Sungim Lee, Johan Lim, Heon-Jin Park,1) STABILITY: Robert M. Little, Terry R. Wallen,and Timothy T. Wheelere (2011)9 proposed a methodand Richard A. Riedel in 198112 did a study onto classify dental arch forms and they identified 3Stability and relapse of mandibular anteriortypes of arch forms, and cross-classification of theBONWILL – HOWLEY ARCH FORM14maxillary by mandibular arch forms showed a morefrequent distribution in the diagonal elements than inthe off-diagonal elements. It was concluded that bydefining area discrepancies as distance measures andapplying them to the cluster method by usingmedoids, the dental arch form can be classifiedkeeping control for the extremes without bias.alignment and concluded that Arch dimensions ofwidth and length typically decreased after retentionwhereas crowding increased. This occurred in spite oftreatment maintenance of initial intercanine width,treatment expansion, or constriction.2) OCCLUSION: Unless the teeth are aligned in aproper arch form in both upper and lower arches, theocclusion will not be normal. Angle (1907)13BASIC TYPES OF DENTAL ARCH FORM 10, 11Majority of them fall into one of the following types:(1) Parabolic: It is shaped like a parabola, with ananterior curve and slightly diverging posterior legs.(2) Hyperbolic: It is shaped like a hyperbola, with aflatter anterior curve and markedly diverging posterioremphasised this with his concept of Line ofOcclusion.3) ESTHETICS: Primary reason for the patient to taketreatment. Teeth arranged in proper arch form, willimprove smile value as proposed by Sarver (2003).Different concepts of arch form:legs.(3) Ellipsoidal: It is shaped like an ellipse with a curveanterior segment and slightly converging posteriorlegs.(4) Square: It has a flat anterior segment and relativelyparallel posterior legs.(5) Omega: It has a curved anterior segment andposterior legs that converge then divergeBONWILL’S CONCEPT OF ARCH FORMIt was founded on the premise that the ideal archshould be based on an equilateral triangle. Bonwillestablished his triangle on the average width betweenthe condyles which he found to be four inches.Hawley felt that orthodontists could not measure thedistance between the condyles accurately and,therefore, chose to base his arch on the width of theIMPORTANCE OF ARCH FORMS:front teeth. The anterior form of the arch was that of acircle, the radius of which was the width of the centralJournal Of Applied Dental and Medical Sciences 4(1);20187
ARCHFORM IN ORTHODONTICS 4(1);2018121and 1ateral incisors and the cuspid. The final form ofTo measure the arch perimeter, they used anthe arch was established by the projection of twoinstrument that was a modified Boley Guage with aequilateral triangles which would vary according tochain incorporated in it – CATANOMETERthe widths of the front teeth.Schulhoff (1997) used the same concept to describeANGLE‟S LINE FOR OCCLUSION13 in 1907the lower arch. Caternary curve is the shape that thedefined the line of occlusion as “the line with which inloop of a chain would take if it were suspended from 2form and position according to type, the teeth must behooks. Shape of the curve depends on the length of thein harmony i.e. in normal occlusion". He describedchain and the distance between the hooks. When thethis line as being more or less a parabolic curve whichwidth across the first molars is used to establish thevaried according to the race, facial type, temperamentposterior attachments, a caternary curve fits the dentaletc.arch form nicely for most individuals. Preformedarchwires based on average intermolar dimensions.APICAL BASE CONCEPT:Bruide & Lilley17 found that the shape of basic bonyIt was proposed by Lundstorm.15 He highlighted thearch at 9.5 weeks I.U, was caternary design. Caternaryneed to consider the apical base when determining thecurve was made popular by work of McConail &arch form for the patient. “Orthodontic experimentsScher, who felt that from an engineering andshowedbybiological point of view, the caternary curve was themechanical treatment is not necessarily accompaniedsimplest curve possible and could be easily explainedby a development of apical base in harmony with ion of the teeth, with the result that the occlusioncannot be maintained.” “Occlusion doesn‟t controlBRADER ARCH FORM 18form and amount of apical base development butThe unique geometry of the curve representingapical base is capable of affecting the dentalsuperior dental arch form is approximated by a closedocclusion”curve with trifocal elliptic properties, with the teethoccupying only a portion of the total curve at itsCATERNARY ARCH FORM16Concept first proposed by David Musich & JamesAckerman (1973).Journal Of Applied Dental and Medical Sciences 4(1);20187constricted end. The primary determinants of archform morphology are the (muscle) tissue forces of the
122ARCHFORM IN ORTHODONTICS 4(1);2018resting state in contradistinction to the intermittentpolynomial least squares curve- fitting program toforces of muscles in functioning states.compare the ellipse and parabolas to 25 pairs of plottedThe geometry of the curve of dental arch form is sodental arch curves. Statistical analysis of the resultrelated with the resting forces of the tongue thatshowed that the ellipse provided a better goodness ofPR C, where:(smaller variance) for the maxillary outer (facial) dentalarch curve than the parabola, while the parabolaprovided a better fit to the mandibular middle curvethan did the ellipse.The ellipse had a total smaller variance of fit to theouter curves in the maxillary and the mandibulararches, while the parabola had a total smaller varianceArch form from polynomial equation-of fit to the middle curves in both the arches. BecausemostP Pressure/unit area.R A radius of curvature at a point along thecompound curve corresponding precisely with thepresent–dayorthodonticproceduresareperformed on the outer (facial) surfaces of teeth, it wasconcluded that the ellipse is the better guide to archform than the parabola.pressure site.C A mathematic constant, exhibiting variation inmagnitude between individuals, and variation in thesame individual at different physiologic ages.Susan H. Pepe in 197522, fit polynomial and catenaryequations to the dentitions of seven children withnormal occlusion. She found that neither catenary norpolynomial curves fit the dental arch well enough toArch form from polynomial equation-serve as a template for an arch wire. The catenary fitthe arch form least accurately. She also found that theHayashi in 196244 used anatomical landmarks along6th degree polynomial equations afforded significantthe buccal cusps and incisal edges to study the curve ofincrease in accuracy of fit over the 4th degree, whichthe dental arch. He found that the arch fit very well tohad been suggested for use by Lu. She felt that the 6thn ea(x-b). Hayashi assumeddegree polynomial had potential as clinical indicatorssymmetry of the arches and, therefore, looked at onlyof arch form and perhaps malocclusion. She suggestedone side of the arch.that spline curves may also be found to have a highthe equation y axK. H. Lu, 196620 felt that Hayashi‟s method was toocumbersome. Lu suggested the use of orthogonalpolynomials for fitting equations to arch form. Theeven- powered polynomials measured the symmetry ofthe arch and the odd- powered the asymmetry He foundthat the fourth degree polynomial fit the arch formquite nicely.James H. Currier in 196921, used a generalizedJournal Of Applied Dental and Medical Sciences 4(1);20187degree of accuracy of fit.Seba AlHarbia; Eman A. Alkofideb; AbdulazizAlMadic, in 200823 did a mathematical Analyses ofDental Arch Curvature in Normal Occlusion and foundout that the polynomial function (fourth order) wasfound to be a reasonable analysis when the objective isto describe the general smooth curvature of the dentalarch, while a Hermite cubic spline is more appropriate
ARCHFORM IN ORTHODONTICS 4(1);2018123when it is desired to track arch irregularities, such asSystems computer derived formula. His subjectiveevaluating treatment changes. It was concluded that dueopinion of their fit to 24 untreated superior adultto its advantage in providing a more naturally smoothocclusions was:curve, the fourth-order polynomial function may be1) The catenary design had agood fit for 27% of theused as a guide to fabricate customized arch wires, orarches while the other three varied form 8-12%;even an entire fixed orthodontic appliance system.2) the R.M. D. S. computer-derived arch yielded 92%24Kazuhito Arai and Leslie A. Will in 2011 evaluatedmoderately good fit with no poor fits,the relationship between subjective classification of3) the Bonwill Hawley, Brader, and catenary curvesdental-arch shape, objective analyses via arch-widthhad between 40-46% moderately -derived good fitsmeasurements, and the fitting with the fourth-orderwith forms 27 to 52% poor fits. "The catenary andpolynomial equation. It was concluded that SubjectiveR.M.D.S computer derived arch forms were superiorclinical assessments were generally in agreement at theoverall to the Brader & Bonwill-Hawley designs,extremes of tapered and square arch forms; theWhite suggested that the lack of fit was due toexceptions were arches with an ovoid shape. Thereasymmetry of the arches.were statistically significant correlations betweensubjective dental-arch classifications and dental-archINDIVIDUALIZED IDEAL ARCHES25dimensions, as well as the ratio determined from thesevariables and polynomial equation analyses. Therefore,Proposed by Larry White in 1978. Undertook a study tofourth-order polynomial equations might be ansee how a collection of ideal, untreated archesimportant factor in the quantitative analysis of dental-conformed to the predetermined arch forms of the mostarch form in orthodontic patients.popular formulae. Models of 24 orthodonticallyuntreated superior, adult occlusions were collected andROCKY MOUNTAIN DATA SYSTEMtracings made on acetate paper & overlays weresuperimposed. The closeness of fit was evaluated andROCKY MOUNTAIN DATA SYSTEM computerderived formula relies upon measurements taken fromgraded as „good fit‟, „moderately good fit‟ and „poorfit‟.inter molar width, inter cuspid width and arch depth asmeasured from the facial surface of the incisors to thedistal surface of the terminal molar. This allowscomputer to be programmed with Cartesian X & Y coordinates that are necessary for arch computation.Facial type is also considered arch design applicableonly to the lower arch25RICKETTS PENTAMORPHIC ARCH FORMS26Considered the following factors in the determinationof the arch form: Arch correlation, size, arch length,where the arch was measured, contact details and format the bracket location. Originally 12 arch forms wereidentified from different studies. These were narrowedWhite in 1978 , compared arch forms derived Fromto 9 by computer analysis. Studies of other normal andfour basic designs the Bonwill-Hawley, the Brader,stable treated patients resulted in elimination of all butthe catenary, and the Rocky Mountain Data5 forms. These pentamorphic arch forms were such thatthey would fit most facial formsJournal Of Applied Dental and Medical Sciences 4(1);20187
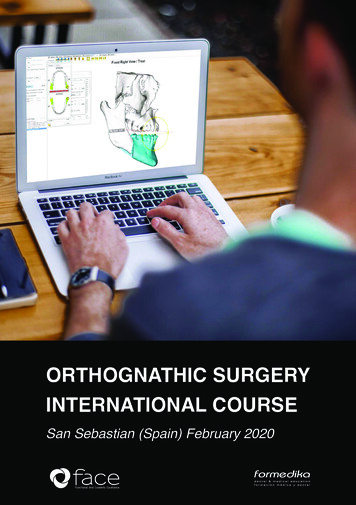
124ARCHFORM IN ORTHODONTICS 4(1);2018RESEARCH ARCH FORM/ CLINICAL ARCHpremolar regions. Cases undergoing single archFORMtreatment, in this way no expansion of treated archAcc. To McLaughlin & Bennet, there is a differenceoccurs. The posterior part of this arch form can easilybetween the clinical and research arch form. Braun et alTaperd Arch FormSquare Arch Form(1966)27 represented arch form by a complexmathematical formula known as “Beta Function”. Theymeasured the centre of each incisor incisal edge, cusptips of canines and premolars and the M-D and D-Bcusp tips of molars. This research arch form can besurprisingly tapered. In contrast clinicians arch wireshape must be based on the points where the wire willlie in the bracket slots of correctly positioned brackets.Ovoid Arch FormThis arch form relates to the mid-point on the labialsurface of the clinical crowns of the teeth, and shouldbe modified to match the inter-molar width of theinclude estimation for the in out which is built into thepatient.bracket system.THE SQUARE ARCH FORMMBT ARCH FORM28Indicated in cases with broad arch form and cases thatThe three basic arch forms are tapered, square andrequire buccal uprighting of the lower posteriorovoid. When superimposed they vary mainly in inter-segments and expansion of the upper arch. After over-canine width, giving a range of approximately 6mm.expansion has been achieved, it may be beneficial toInter-molar widths are similar, but the molar areas canchange to the ovoid arch form in the later stages ofbe widened or narrowed as needed, by easy wiretreatment. The square arch form is useful to maintainbending.expansion in upper arches after rapid maxillaryexpansion.THE TAPERED ARCH FORMThis arch form provides the narrowest inter-cuspidTHE OVOID ARCH FORMwidth & Indicated for patients with narrow, taperedIt is the most preferred arch form. The ovoid arch formarch form and gingival recession in canine andhas proved to be good, reliable arch form for highJournal Of Applied Dental and Medical Sciences 4(1);20187
125ARCHFORM IN ORTHODONTICS 4(1);2018percentage of cases treated. Treated cases have shownoriented as it moves to the desired position and cangood stability, with minimal amounts of post-treatmentdesign arch shape as desired, within the parameters ofrelapse. When superimposed, the three shapes varythe scanned limits of the buccal and lingual corticalmainly in inter-canine and inter-first premolar width,plates.giving a range of approximately 6 mm in this area.Arch Form in Lingual OrthodonticsDue to the lingual morphology of the teeth, a straightwire cannot be engaged lingually. The arch wire formis changed accordingly. The wires used here are“Mushroom Shaped”, with an offset present between4. Once the patient's customized occlusal scheme isfinalized, the data from the setup then is drawn on bythe CAD-CAM machinery to cut each bracket toindividual specifications for that patient, and the archwires also are manufactured to the specifications set bythe clinician.canine and premolar. During sliding mechanics, there isa transverse bowing of the arch leading to distortion ofCONCLUSIONthe arch form. To prevent this posterior legs of thearchwire are bowed outward to compensate for theThe universal ideal arch form is one of the mosttransverse bowing of the arch. Andreiko (1994)persistent but exclusive task for most of the orthodonticasserted that shape of the mandible should dictate theresearchers have. Although literature review illustratesarch form, with the teeth theoretically aligned anddivergent views on the shape of arch form, it is nowcontained within the limits of mandibular bone. Thegenerally believed that the arch shape is determined byarch forms are derived from the skeletal and dentalan interplay between genetic and many variedanatomy and are therefore designed to be closer to anenvironmental factors such as pressure from softanatomic ideal than a mathematical ideal. Previous archtissues; shape and position of jaws; alteration inwire shapes had them in the concept of an ideal archeruptiveform; anatomy probably was not given enoughConcerning the orthodontic treatment, basic principleconsideration in design.of arch form in is that within reason, the patientsmechanismandmorphologyofteeth.original arch from should be preserved. Therefore, ifThe appeal of the newer approach includes thefollowing.the preformed arch wires are to be used, it is to be keptin the mind that their shape should be considered a1. Arch forms are derived from the skeletal and dentalstarting point for the adjustment necessary for properanatomy and therefore are designed to be closer to anindividualizationanatomic ideal than a mathematical ideal.preformed arch wire do not reflect these variations in2. Individualized treatment is simplified.asallthepresentlyavailablethe arch form. Clinicians should therefore be cautiouswhen treating individuals to a mathematically derived3. This works by scanning models of the patient'sideal. Because of these complex problems, anddentition to a resolution of 50μm or 0.002 inch. With arelatively low knowledge of dental arches, as of today,three-dimensional control interface the clinician has thethere is no universally accepted ideal arch form. Thecapability of specifying exactly how each tooth isirony of wisdom is that, the more we know about aJournal Of Applied Dental and Medical Sciences 4(1);20187
ARCHFORM IN ORTHODONTICS 4(1);2018126particular subject, the more our ignorance unfolds and10.Black GV. Descriptive anatomy of humanthe goal seems far ahead.teeth. 5th ed. Philadelphia: E.H. Treatment ofMalocclusion of the teeth.11.REFERENCESBarrow GV and White JR. Developmentalchanges of the Maxillary and Mandibular Dental1.Hrdlicka A. The normal dental arch. DentalArches. Angle orthod.1952;22:41-46.Cosmos. 1916; 58:1029-1032.12.2.William PN. Determining the shape of theNormal Arch. Dental Cosmos. 1917; 59:695-708.3.Little RM, Wallen TR, Riedel RA. Stability andrelapse of mandibular anterior alignment: first premolarextraction cases treated by traditional edgewiseMcCoy JD. A Consideration of the Normalorthodontics. Am J Orthod 1981;80:349-64.Arch Form and Some of the Methods of Determining it.13.Int. J. Orthod. and Oral Surgery 1919; 5: 697-723.Philadelphia: S. S. White Dental Mfg. Co., 1907, p. 23.4.14.Stanton FL. Arch Predetermination and aAngle EH. Treatment of Malocclusion of teeth.Hawley CA. Determination of the Normal ArchMethod of Relating the Predetermined Arch to theand its Application to Orthodontia. Dental Cosmos.Malocclusion to show the Minimum tooth Movement.1905; 47: 541-552.Int. J. Orthod. 1922; 9:757-778.15.5.Lundstrom A F, Malocclusion of the teethIzard, G. New Method for the Determination ofregarded as a problem in connection with the apicalthe Normal Arch by the function of the Face. Int. J.base. International Journal of orthodontia, Oral surgeryOrthod. 1927;13:582-595.and Radiology. 1925; 11: 1022-10426.ChuckGC.IdealArchForm.AngleOrthod.1934; 4:312-327.7.Noroozi H, Nik TH, Saeeda R. The DentalTriviño T, Siqueira DF, and Scanavini MA. Anew concept of mandibular dental archform 8;133:1015-1022.9.Musich, D. R., and Ackerman, J. L., Thecatenometer: A reliable device for estimating dentalArch Form Revisited. Angle Orthod. 2001;71:386–389.8.16.Lee SJ, Lee S, Lim J, Park HJ, and Wheelerearch perimeter, Am. J. Orthod.1973 April; 63( 4):366375,.17.Burdi, A. R., and Lillie, J. H., A catenaryanalysis of the maxillary dental arch during humanembryogenesis, Anat. Rec.1966 ;154:13-20.18.Brader AC. Dental arch form related withintraoral forces. Am. J Orthod 1972; 61:541-61TT. Method to classify dental arch forms. Am J Orthod19.Dentofacial Orthop.2011; 140:87-96.Curve of the Dental Arch. Bull. Tokyo Med. Dent.Hayashi T. A Mathematical Analysis of theUniv.1962; 3:175-218.Journal Of Applied Dental and Medical Sciences 4(1);20187
ARCHFORM IN ORTHODONTICS 4(1);201820.Lu KH. An orthogonal analysis of the form,symmetry and asymmetry of the dental arch. Archiveof Oral Biology 1966;11:1057- 69.21.Currier JH. A computerized geometric analysisof human dental arch form. Am J Orthod 1969; 56:16575.22.Pepe SH. Polynomial and catenary curve fits tohuman dental arches. J Dent Res 1975; 54:1124-32.23.AlHarbia S, Alkofideb EA, AlMadic A.Mathematical Analyses of Dental Arch Curvature inNormal Occlusion. Angle Orthod.2008; 78:281-287.24.Arai K and Will LA. Subjective classificationand objective analysis of the mandibular dental-archform of orthodontic patients. Am J Orthod DentofacialOrthop.2011; 139:315-321.25.White LW. Individualized Ideal Arches. J.Clinical Orthod.1978; 12:779-787.26.Ricketts RM 1979 Bioprogressive therapy.Book 1. U.S.A :Rocky Mountain Orthodontics27.Braun S, Hnat WP, Fender DE, Legan HL. Theform of human dental arch. Angle Orthod. 1998Feb;68(1):29-36Journal Of Applied Dental and Medical Sciences 4(1);20187127
ARCHFORM IN ORTHODONTICS 4(1);2018 120 Journal Of Applied Dental and Medical Sciences 4(1);20187 Shin-Jae Lee, Sungim Lee, Johan Lim, Heon-Jin Park, and Timothy T. Wheelere (2011)9 proposed a method to classify dental arch forms and they identified 3 types of arch forms, and cross-classification of the .