Transcription
EMDR & Dissociation: Keepingthe dissociated client anchoredin the therapy roomIan Plágaro-NeillEMDR ConsultantAutumn Workshops – Sheffield – 5th October
Dissociation & EMDR This is an overview of dissociation and how itcan be reversed during EMDR work. Essential further reading can be found inHealing the Heart of Trauma and Dissociationwith EMDR and Ego State Therapy. Othersuggested books are Coping with TraumaRelated Dissociation, Stranger in the Mirror,The Haunted Self, Ego States: Theory andTherapy (Watkins and Watkins).
Imagine looking at a photo of yourself as achild and knowing that it must be you becausethere is a physical similarity. Also peoplearound you tell you that you were there.However, you cannot place yourself in thephoto; you cannot look at it as if through your‘child’s eye’.
What is dissociation? The term dissociation was firstattributed to Janet in the 1870swhereby he described a mentalstructure created to exclude traumaticlife events from conscious awareness. Boon et al (2011) give the followingdefinition: ‘Dissociation is a majorfailure of integration that interferes withand changes our sense of self and ourpersonality’.
Dissociation is a healthy adaptivedefence used almost universally bypeople in response to overwhelmingstress or life-threatening danger. However, most people experience milddissociative symptoms on occasionswhen their lives are not in immediatedanger.
So we could say that dissociationruns along a continuum; such aslosing track of time when reading agood book to the client who avoidsdistress by not letting him/herselffeel anything emotionally.
People with dissociative disorders do not feelintegrated and instead feel fragmented because theyhave memories, thoughts, feelings, behaviours etcthat are experienced as uncharacteristic and foreign. They experience more than one sense of self, andthey do not experience these selves as whollybelonging to one person.
These divided senses of self and responsepatterns are called dissociative parts of thepersonality. It is almost as though there are not enoughlinks or mental connections between onesense of self and another; between one set ofresponses and another.
In a ‘good enough’ childhood environmentego states develop in a state of coconsciousness and are relatively wellintegrated in their functioning.Maintainingconnectionwith othersProductivityCorestateEnergymaintenance:food, sleep, focusSelf-defence: Fight or FlightPlay,funSubmit: When fightor flight is notpossible
However a child repeatedly abused by a caretaker is in animpossible dilemma. Defensive systems of anger and escapefrom harm are activated, but at the same time, the child mustcontinue to regard the abusing caregiver as a source ofsupport necessary for survival.
In these circumstances a child will oftendissociate the memories of the abuse (whichcan be a vague memory or a minimisation ofthe significance of abusive events).
The child will turn anger inward andfrequently have an attitude towards their ownabuse ‘I deserve this because I am bad’. This isdescribed as an ‘introject’ which takes on theattitudes of the perpetrator in order tocontinue to maintain the necessaryconnection with him/her.
So it is reasonable to state that peoplewho have suffered trauma, especiallywhen it occurs in childhood, are morelikely to experience high levels ofdissociation. In order to process traumatic memorieswith EMDR it is necessary for thedissociation to be managed effectivelyand for the client to be stable (Shapiro2001, p.95).
This shows how EMDR works, in the absence ofsignificant psychological defences and/or dissociationDual Attention Bi-lateralStimulation ‘Adult perspective’ Trauma memory Present Orientation Image, Negative Cognition,Emotion, Physical Sensations Present Safety Positive resources Resolution of traumatic memory Integration of traumatic event into the person’s life Increased Self EsteemKnipe 2011
This shows what happens with EMDR in the presence ofpsychological defences and/or dissociationBi-lateral Stimulation ‘Adult perspective’? Image? Present Orientation? NegativeCognition Present Safety? Positive resources? Emotions PhysicalSensationsKnipe, 2011Ego StateDefences Trauma memory Image
As we can see from the diagram on theprevious page, the use of standard EMDRprocedures will often result in ‘blocking’by a dissociated person. The clientreports ‘Nothing is different’, ‘This isn’thelping’.
For successful EMDR therapy to take place theclient must metaphorically have one foot in thepast and one foot in the present If we think about dissociation, people will oftenfeel that the foot in the past is the biggest. Consider preparatory work as helping themregain more of a balance.
Assessing for dissociation The psychometric measure used to assess fordissociation during EMDR training is theDissociative Experiences Scale (DES-2) whichis a 28 question self administeredquestionnaire. Note, the DES-2 is a screening tool, not adiagnostic tool. For a more detailed analysisof dissociation the MID (Dell, 2006) can beused (free of charge and available from PaulDell PFDell@aol.com ).
One way to look for signs of dissociation is toask the client about their earliest memories(good or bad). Memories formed before the ages of approx3-4 can be described as implicit. Once sufficient speech is developed it is usualfor people to remember events from approx3-5 years old An indicator of dissociation is gaps inchildhood memories; gaps of years or monthsat a time.
0-18
Sometimes clients will state that they feel as though they areon the outside looking in at their life (depersonalisation) If clients describe feeling ‘spacey’ this can be an indication ofdissociation A less obvious sign is if the client ‘switches’ ego states. Lookfor a change in the tone of voice or posture, especially if theclient suddenly sounds or looks like a child. The client mightrock or fidget uncharacteristically
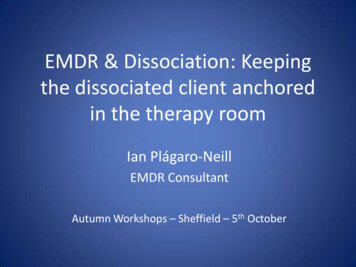
In order to understand more pronouncedlevels of dissociation I would like to brieflymention the idea of ego state therapy, whichhas been around, in different guises, for manydecades. There are several approaches which have incommon the idea that different personalityparts, sub-personalities, or ego states canhave different views of reality. I have successfully incorporated ego statetherapy into EMDR with positive results(Plágaro-Neill, 2011).
If you think about ego states in conflict orsimply being at odds with each other, it fits inwith the idea of internal splitting. The more that ego states can work together orexist in a state of consensus the more ‘whole’– and less dissociated - the person will feel.
Method I begin by asking the client if they ever have asense of different parts of themselves, internalarguments or discussions I then draw a dot in the centre of apage/white board The first ego state I ask the client to identify istheir current ‘self’ which provides a sense ofhere and now. If the current ‘self’ is away from the centre it islikely that they will be struggling (especially ifthey subsequently place child states at thecentre)
Names of ego states might be actualnames, representative names, male orfemale. I usually ask the client to give mea couple adjectives associated with thename. Initially I am looking to plot out individualstates to give the client and myself a senseof perspective and to identify alliancesand conflicts To follow is an example of an ego statediagram:
Mick’s Ego State DiagramGuilt (-2)Mick (54)Striving (4-5)Interested (7)Caring (4)Crushed(32)Mr Angry(Child)Rebel (15-16)Competent(40 )Mr Worry(Young Child)
The client’s ability to access andintegrate with child ego states alsoprovides a sense of how the ‘adult’feels towards the ‘inner child/ren’.
The Back of the Head Scale (BHS) is ameasurement tool that is useful in assessingthe client’s moment-to-moment level ofdissociation. This procedure is introduced to the clientduring the preparation phase, before anydesensitisation of trauma commences.
Think of a line that goes from approx 15-18inches in front of your face, running backwardsthrough your face to the back of your head The point 15-18 inches in front of your facemeans that you are fully in the room, in the hereand now Let the other point, at the back of your head,mean that you are so distracted by disturbingthoughts, feelings or memory pictures that youfeel like you are somewhere else.
Reversal technqiues A straightforward technique is to encourage theclient to ‘ground’ his/herself into the presentmoment; paying attention to details in the roomand/or their body (check with the client firstespecially if working with issues of childhood abuse). Other techniques include asking the client to “Take adrink of water.” “Hold this drop of water/ice cube in your hand.” “Hum a song and then count to ten”, etc.
One of the simplest methods for bringing aclient out of a dissociative state (and can beused with CIPOS/BHS) is to get them to playcatch with a cushion, a scrunched up piece ofpaper or a soft ball (check first with the client)
Constant Installation of Present Orientation& Safety (CIPOS) The CIPOS method is used in conjunction with theBHS and basically consists of using eye movements tostrengthen or install the client’s awareness of a clearsubjective sense of being present in the immediatereal-life situation of the therapy room It is used in the preparation phase or during actualdesensitisation of a particularly disturbing traumamemory ntation-and-safety-cipos-j
Essentially, with the client’s agreement youagree to allow them to oscillate between thepresent safety of the present moment and thetrauma memory from the past Gradually you increase the amount of timethe client spends with the trauma memory
2-10 seconds ofdeliberate dissociationinto traumatic material,No EMOrientation topresent safety,Paired with EMPresent safety,EMPresent safety,EMPresent safety,EMPresent safety,EMPresent safety,EMPresent safety,EM2-10 seconds in trauma,No EM2-10 seconds in trauma,No EM2-10 seconds in trauma,No EM2-10 seconds in trauma, No EMMore than 10 seconds in trauma, No EMMore than 10 seconds in trauma, EM(standard EMDR EM setsKnipe, 2008
Longer-term systematic techniquesfor reversing dissociation can befound in Coping with Trauma-RelatedDissociation: Skills Training forPatients and Therapists (Boon et al,2011)
REFERENCESBoon, S. Steele, K. & Van der Hart, O. (2011) Coping with Trauma-RelatedDissociation: Skills Training for Patients and Therapists. New York: Norton.Dell, P.F. (2006) The Multidimensional Inventory Of Dissociation (MID): Acomprehensive measure of pathological dissociation. Journal of Trauma andDissociation, 7(2), 77-106.Forgash, C. & Copeley, M. (Eds.) (2008)Healing the Heart of Trauma and Dissociation with EMDR and Ego State Therapy.New York: Springer Publishing Company.Knipe, J Loving Eyes. Procedures to Therapeutically Reverse Dissociative ProcessesWhile Preserving Emotional Safety. In: Forgash, C. & Copeley, M. (Eds.) (2008)Healing the Heart of Trauma and Dissociation with EMDR and Ego State Therapy.New York: Springer Publishing Company.Plágaro-Neill, I. (2011) The use of ego state therapy and EMDR to reverse dissociation.Northern Region Autumn Workshops, October 2011.Shapiro, F. (2001)EMDR, Basic Principles, Protocols and Procedures. 2nd Edition. New York: GuilfordPress.Steinberg, M. & Schnall, M. (2001) The Stranger in the Mirror: Dissociation – TheHidden Epidemic. New York: Harper.Van Der Hart, O. Nijenhuis, E.R.S. & Steele, K. (2006) The Haunted Self: StructuralDissociation and the Treatment of Chronic Traumatization. New York: Norton.Watkins, J.G. & Watkins, H.H. (1997)Ego States: Theory and Therapy. New York: Norton.
THEEND
suggested books are Coping with Trauma-Related Dissociation, Stranger in the Mirror, The Haunted Self, Ego States: Theory and Therapy (Watkins and Watkins). Imagine looking at a photo of yourself as a child and knowing that it must be you because there is a physical similarity. . J Loving Eyes. Procedures to Therapeutically Reverse .