Transcription
Diabetes FundamentalsNutrition and ExerciseBeverly Dyck Thomassian, RN, MPH, BC-ADM, CDEPresident, Diabetes Education Services Copyright 1999-2014, Diabetes Education Services, All Rights Reserved.Diabetes Fundamentals Nutrition guidelines Describe current MNTrecommendationsList 3 teaching strategies tohelp patients succeed Exercise Guidelines Discuss exercise goals forpeople with diabetesDescribe safety precautionsGood Resources Review Exchange ListReview ADA Standards of Care:Diabetes Education Services www.DiabetesEd.netPage 1
Assess Knowledge, Self Management Skills Eating Patterns Preferences, portionsizes, timing on mealsand snacks, eatingenvironment,disordered eatingMedical Nutrition Therapy – ADA 2014 No ideal percentage of calories from protein, carbohydrate and fatfor people with diabetes. Macronutrient distribution should be based on an individualizedassessment of eating patterns, preferences and metabolic goals.Medical Nutrition Therapy – ADA 2014Focus on the IndividualMaintain pleasure of eating Provide positive messagesabout food Limit food choices only whenbacked by science Provide practical tools Refer to a RD and DiabetesEducation – Lowers A1c by 1-2% Diabetes Education Services www.DiabetesEd.netPage 2
Medical Nutrition Therapy – WhatMedicare Covers 3 hours initial benefit infirst calendar year2 hours follow-upannuallyMust be ADA/AADERecognizedMNT for diabetes andrenalApproach Depends on Patient New Type 2 Portion ControlPlate MethodRecord KeepingEducationOn Insulin? Carb countingPost prandial checksSodium, Fat and Fiber Sodium – Try and keep less than2,300 mg a dayVitamin and mineral supplementsnot recommended -lack of evidence.Fat - same as recommended forgeneral population Less than 10% saturated fat,Limit trans fatsLess than 300 mg cholesterol dailyMediterranean Diet looks like goodoptionFiber 25 -38 gms a dayDiabetes Education Services www.DiabetesEd.netPage 3
Average American Consumes25 teaspoons of sugar a day (400 cals)Warning label on sodasproposed One soda has 12 teaspoonssugar On avg, 1 person consumes 40gallons of soda each year ADA guidelines “limit sodas andbeverages with sugar, HighFructose Corn Syrup, (HFCS) ADA recommendationEat Less Junk Food & Sugary Drinks – Less Processed FoodsLess Sugary Beverages increase visceral adiposityWith sugar orHigh fructose corn syrupSoda Tax?Junk Food Tax?Teaching About Eating HealthyMajor food groups“Handy Diet”Plate MethodExchange ListsFood Diaries / GlucoseRecordsCarbohydrate CountingAssess what is best for the situation.Diabetes Education Services www.DiabetesEd.netPage 4
Move toward the TomatoLosing 2-8kg Early in diagnosis Type 2 HelpfulADA 2014 Weight Loss – The optimal macronutrient intake to lose weightnot knownThe literature does not support one particularnutrition therapy to reduce weight, but rather aspectrum of eating patterns that result in reducedenergy intake.To lose one pound – avoid 3,500 cals Decrease intake 250-500 cals daily exerciseSuccessful weight loss strategiesincludeWeekly self-weighingEat breakfast Reduce fast food intake. Decrease portion size Increase physical activity Use meal replacements Eat healthy foods Diabetes Education Services www.DiabetesEd.netPage 5
Bariatric SurgeryConsider for adults with BMI 35 or greaterIncreases gut hormone availability Need life long support and monitoring More likely to cause remission* with recentlydiagnosed diabetes (more beta cell mass) 68% remission within 5 years35% redeveloped diabetesLong term benefits still under investigation*remission BG levels normal without medsUSDA www.myplate.govBalancing Calories Enjoy your food, but eat less. Avoid oversized portions.Foods to Increase Make half your plate fruits and vegetables. Make at least half your grains whole grains. Switch to fat-free or low-fat (1%) milk.Foods to Reduce Compare sodium in foods like soup, bread, and frozen meals― and choose the foods with lower numbers. Drink water instead of sugary drinks.Another plate exampleDiabetes Education Services www.DiabetesEd.netPage 6
How nutrients affect blood sugarCarbs affect Post meal BloodGlucoseo Starcho Fruito Milko DessertsCarbohydrate Needs forMost AdultsEach MealSnacksGrams45-60 gm15-30 gmServings3-41- 2Carbs affect Post Meal Blood GlucoseRDA – at least 130 gms of Carb a dayDiabetes Education Services www.DiabetesEd.netPage 7
Each Food has:80 Calories15 grams carbCarb Counting - Starch1/2 cupcooked beans1 small ear of corn or1/2 cup corn1/3 cupcooked pasta3/4 cup coldcereal1 slice bread1 small potato1/3 cupcooked rice1/2 English muffin1 small tortilla5-6 small crackersEach Food has:60 Calories15 grams carbCarb counting- fruit1 small freshfruit½ cup fruit juice½ banana½ cup unsweetenedapple sauce1 slice bread17 small grapes1 cup melon¼ cup dried fruit2 tbsp raisins1 1/4 cupstrawberriesCarb Counting - MilkEach Food has:90-150 calories12-15 grams carb8 oz buttermilk1 packet diet hot cocoa1 slice bread6 oz plainyogurt8 oz milk8 oz soy milk6 oz light fruityogurtDiabetes Education Services www.DiabetesEd.netPage 8
Carb Counting - Sweets2 inch squarecake or brownie,unfrosted½ cupregular jello½ cup diet puddingEach Food has:Calories vary15 grams carb2 tbsp lightsyrup1 slice bread1 tbsp syrup, jam, jelly,table sugar, honey2 smallcookies¼ cup sorbet½ cup ice creamor frozen yogurt½ cup sherbetChoose Healthy CarbsoCarbs have fiber, vitamins, minerals and phytonutrientso25 gms of fiber a dayoPower Carbs include:oBeansoVeggiesoFruitsoWhole grain foods10 SuperfoodsBeansDark Green Leafy Vegs Citrus Fruit Sweet Potatoes Berries Tomatoes Fish High in Omega-3Fatty Acids Whole Grains Nuts Fat-Free Milk andYogurt Diabetes Education Services www.DiabetesEd.netPage 9
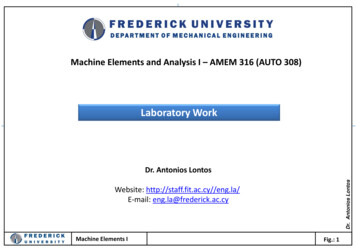
Nutrition FactsServing Size 1/2 cup (114 g)Servings Per Container 4Amount Per ServingCalories 90Calories from Fat 30% Daily Value*Total Fat 3g5%Saturated Fat 0g0%Cholesterol 0g0%Sodium 300mg13%Total Carbohydrate 13g4%Dietary Fiber 3g1 tsp sugar 4 gmsFooducate App –gives grade andnutrition info.12%Sugars 3gProtein 3gVitamin A80%Calcium4%**Vitamin CIron60%4%* Percent Daily Values are based on a 2,000 calorie diet. Your dailyvalues may be higher or lower depending on your calorie needs:Total FatSat FatCholesterolSodiumTotal CarbohydrateFiberCaloriesLess thanLess thanLess thanLess thanCalories per gram: Fat 375g30gCarbohydrates 4Protein 4Dietary Fat and Cholesterol Guidelines Avg Calorie distribution for PWD 45% of calories from carbs30-40% from fat,16-18% from proteinGuidelines from ADASaturated fats 10% of caloriesLimit trans fat as much as possible Limit total dietary cholesterol to300 mg/day Fats- 9 calories per gram Monounsaturated - healthyooo Olive & canola oils, Nuts, AvocadoLowers total cholesterol and LDLRaise HDL, high in omega 3 fatty acidsPolyunsaturated - healthyoocorn, walnut, safflower, soybeanLowers total cholesterol and LDL Saturated fats (limit 10%)oooServing sizesoooo1 tsp butter, margarine, oil,mayonnaise1 Tbsp salad dressing,cream cheese, seeds2 Tbsp avocado, cream,sour cream1 slice baconAnimal products – meat, chicken, pork,fish, skin, cheese butter, dairyPlant products include; palm, coconut,palm kernel oilSolid at room tempDiabetes Education Services www.DiabetesEd.netPage 10
Unhealthy Dietary Fats Trans Fat – strong link betweendiet high in trans fat and heartdisease Lowers HDLIncreases LDLMay increase wt gain and abdominal fatMay contribute to type 2 diabetesLook on label and look for words“hydrogenated” or “partiallyhydrogenated”.Diabetes Prevention ProgramFocus on fat wt loss gnition/curriculum.htmProtein Recommendations -2014 For people with diabetes and no diabeteskidney disease, evidence is inconclusive forideal amount of protein; there fore, goalsshould be individualized. RDA – 0.8gm good qualityprotein/kg/day Protein seems to stimulate insulin response,do not use to treat hypoglycemiaFor those with kidney failure, reducing theamount of dietary protein is notrecommended. Does not improve outcomes.Diabetes Education Services www.DiabetesEd.netPage 11
Protein – 4 cals per gramoChoose lean proteinooooLimit high fat proteinooooPoultry, fish, egg, lean beefPlant sources- beans, lentils, nutsLow fat cheese- cottage cheese, mozzarella cheeseBacon & sausageHigh fat cuts of beefWhole milk cheeseServing sizeoo1 oz ¼ cup3 oz deck of cardsUsing Alcohol SafelyWomen- 1 or fewer alcoholic drinks aday Men 2 or fewer alcoholic drinks a day 1 alcoholic drink equals 12 oz beer, 5 oz glass of wine, or 1.5 oz distilledspirits (vodka, gin etc)If drink, limit amount and drink w/food. Can cause hypo and worsenneuropathy Ms. Gonzales’ Daily Meal planDiabetes Education Services www.DiabetesEd.netPage 12
Celiac Disease Type 1 – Affects 10 \%Immune reaction to gluten - affects function of villi inintestine, decreasing nutrient absorptionS/S: bloating, malabsorption, wt loss, fatty stools,diarrhea, muscle tenderness, failure to thriveDiagnosis: measure either anti-endomysial antibodies(EMA) titers or tissue transglutaminase.If positive, refer to GI specialist for endoscopy andbiopsy of small intestine to confirm diagnosis.Treatment – Gluten Free for Life Avoid Wheat (einkorn, durum, faro, graham,kamut, semolina, spelt), Rye BarleyRefer to a dietitianASSOCIATED AUTOIMMUNE DISORDERS Insulin-dependent Type 1 Diabetes Mellitus, Liver diseases,Thyroid Disease-Hashimoto’s Thyroiditis, Lupus (SLE),Addison’s Disease, Chronic Active Hepatitis, RheumatoidArthritisEx of Gluten Containing Foods Brown rice syrup Breading & coating mixes Croutons Energy Bars Flour or cereal products Imitation bacon Imitation seafood Marinades Pastas Processed luncheon meats Sauces, gravies Self-basting poultry Soy sauce or soy saucesolids Soup bases Stuffings, dressing Thickeners (Roux) Communion wafersAnd more!Diabetes Education Services www.DiabetesEd.netPage 13
Gastroparesis Gastroparesis: affects 20 – 30% of pt’sw/ longstanding dmDelayed emptying of stomachcontents due to nerve damageS/S include early satiety, fullness,postprandial hypo, vomitingDiagnosis: gastric emptying studies,post-prandial hypoglycemiaTx: improve BG, small, low fat & fibermeals meds: reglan, erythromycinDisordered Eating “DiaBulimia”People with type 1 diabetes givethemselves less insulin than needed tolose weightTends to start in adolescence, morelikely to occur in women than men.Signs: unexplainable spikes, A1c, weightloss, lack of marks from fingerpricks,lack of prescription refills for diabetesmeds, records that don’t match A1c.Treatment – Mental health specialistand teamPhysical Activity – Key areasADA and American College ofSports Medicinerecommendations Benefits, barriers precautions Exercise and activity plan(aerobic, resistance training,etc) Adjustment and monitoring offood and/or meds Diabetes Education Services www.DiabetesEd.netPage 14
Physical Activity - Kids Children should beencouraged toengage in at least60 minutes ofphysical activity aday.Physical Activity - ADA Adults with diabetes – 150 minutes a week of moderateintensity aerobic physical activityspread over at least 3 days/wkDon’t miss more than 2consecutive days of exercise.In absence ofcontraindications, type 2adults should engage inresistance training 2x’s a wkDefinitions Physical activity Exercise Bodily movement produced by thecontraction of skeletal muscle that requiresmore energy than when restingSubset of physical activity that is planned,structured and includes repetitive bodymovementsPerformed to improve or maintain physicalfitnessSedentary behavior Little on no movement or physical activityDiabetes Education Services www.DiabetesEd.netPage 15
Progressive Resistance exerciseImproves insulin sensitivityGoal is 2 sessions a week Examples include: Exercise with free weights, wtmachinesEach session consisting of least: One set of five or more resistanceexercises using large muscle groupsBenefits of Exercise Improve BG Improves insulin sensitivityReduce CV Risk factorsMaintain wt loss Contribute to well being Muscle strength Slows decline in mobility Importance of Exercise with Diabetes Vital component of prevention aswell of the management of type 2diabetesGreatest impact in improvingmetabolic abnormalities in type 2when started early in progressionfrom IR to Pre Diabetes to DMType 1 – emphasis on adjustinginsulin to allow for safeparticipation in all forms ofactivity.Diabetes Education Services www.DiabetesEd.netPage 16
Pre-exercise Eval Use clinical judgment when making physicalactivity suggestions and check in withprovider if unsure.Encourage high risk pts to start with lowintensity and short time. Increase duration and intensity slowlyContraindications to certain types ofexercise: Uncontrolled HTN, severe autonomic or peripheralneuropathy, history of foot lesions, unstableproliferative retinopathy.Pt w/ complications require a more thoroughassessment.Patients to discuss symptoms with provider beforestarting exerciseChest pain and/or shortness ofbreath Leg cramps that go away with rest Head, shoulder, neck and or backaches. Any unexplained pain above the beltline should be considered cardiac inorigin until proven otherwise. Hormone Response –Type 1Exogenous insulin remains highIncreased insulin sensitivity Increased insulin absorption What is this group at risk for?What strategies to stay safebefore, during and afterexercise?Diabetes Education Services www.DiabetesEd.netPage 17
Hormone Response –Type 2Decreased secretion ofendogenous insulin Increased insulin sensitivity Increased glucose disposal What is this group at risk for?What strategies to stay safebefore, during and afterexercise?Duration of Hypoglycemia RiskDuring exercise Immediately after exercise Post exercise late onset hypo More often in type 1More often at nightModerate to high intensity exercise 30 min4 to 15 hours following an exercisesessionHypoglycemia Prevention StrategiesIf planned activity, adjust insulinin anticipation of activities Reduce insulin in post exerciseperiod Frequent monitoring in postexercise period Pt to keep log to determine howresponds to different activities,duration and intensity. Diabetes Education Services www.DiabetesEd.netPage 18
Hypoglycemia Prevention StrategiesCarry fast acting carb/ glucagonER Kit Extra CHO in post exercise period Caution with alcohol postexercise Adjust carbohydrate prior toplanned activity: If BG 100 prior to exerciseIf using insulin and /or secretagogues 15 gms carb snackBehavior Change and Smart GoalsJulie currently walks herdog 3 times a weekaround the block. Is this exercise? What new and revisedSMART Goal could youset with her? Diabetes Education Services www.DiabetesEd.netPage 19
Setting SMART GoalsSpecificMeasurable Attainable Realistic Timely Behavioral Goal – Walk the dog around the block 4days a week.Walk the dog around the blocktwo times.Do 10 minutes of weight bearingactivity on 2 of the days youdon’t walk the dog.Help Patients Prepare for SetbacksThank YouQuestions?Emailbev@diabetesed.net Webwww.diabetesed.net Diabetes Education Services www.DiabetesEd.netPage 20
Diabetes Education Services www.DiabetesEd.net Page 6 Bariatric Surgery Consider for adults with BMI 35 or greater Increases gut hormone availability Need life long support and monitoring More likely to cause remission* with recently diagnosed diabetes (more beta cell mass) 68% remission within 5 years 35% redeveloped diabetes Long term benefits still under investigation