Transcription
PATIENT ASSESSMENT SCREENINGTOOL AND OUTCOMES REGISTRY(PASTOR/PASTOR PLUS)
DoD Pain Management Task Force––––Provide recommendations for MEDCOM for acomprehensive pain management strategythat is holistic, multidisciplinary, and multimodalutilizes state of the art/science modalities and technologies, andprovides optimal quality of life for Soldiers and other patientswith acute and chronic pain.Adopt a clinical information system that provides painassessment screening with an outcome registry to promoteconsistency in pain care delivery*--Army Pain Management Task Force Charter; signed 21 Aug 2009Relieving Pain in America: A Blueprint for TransformingPrevention, Care, Education and Research, June 2011 Recommendation 4.1.9.1Jointly fund development of a Pain Assessment ScreeningTool and Outcome Registry under the direction of a centralpain management advisory board.
Problem StatementMilitary Health System (MHS) looking to develop an enterprisepain management capability that would provide needed outcomesevidence to: Standardize pain assessment process Centralize pain data registry and pain outcomes trackingPain management in it’s current state adversely impacts theentire care continuum. Physicians cannot guide treatment decisions Patient involvement is limited Efforts of military and civilian researchers to identify the mosteffective pain management strategies are impeded Pain is number one reason veterans seek care3
CREATE A “PSYCHOMETRICALLY VALIDATED,DYNAMIC SYSTEM TO MEASURE PROSEFFICIENTLY IN STUDY PARTICIPANTS WITH AWIDE RANGE OF CHRONIC DISEASES ANDDEMOGRAPHIC CHARACTERISTICS.”National Institutes of Health,2003
PROMIS10 Years and 100 Million Dollars Later 40,000 people have contributed dataLongitudinal, clinical validation in a host ofchronic conditionsHuge push to use PROs in clinical settingsValue Based Care Care Networks
RESEARCH, OUTCOMES REGISTRY, CLINICALDECISION TOOLWeb application served from MAMC– Clinical Assessment Using validated computer adaptive testing (CAT) PROMISinstruments– Clinical Report/Decision Tool Longitudinal patient pain/function/alert data in concise format– Patients Enter Information Prior to Appointments Using the web capable device of their choice
PLUSPLUS Specialty support focus PROMIS Sleep DisruptionPROMIS Global Satisfaction with sex life Tampa Scale of Kinesiophobia - TSK-11Pain Catastrophizing Scale – PSCPain Self Efficacy Questionnaire – PSEQChronic Pain Acceptance Questionnaire – CPAQPTSD checklist-Civilian Version - PCL-C *Drug Abuse Screening Test – DAST 10 * consideration -Patient Activation Measure – PAM 13/8* Triggered logic
PLUSFunctional Restoration : Specialty support focus Sit to StandHarvard Step TestProgressive Isoinertial Lifting Evaluation ( PILE)
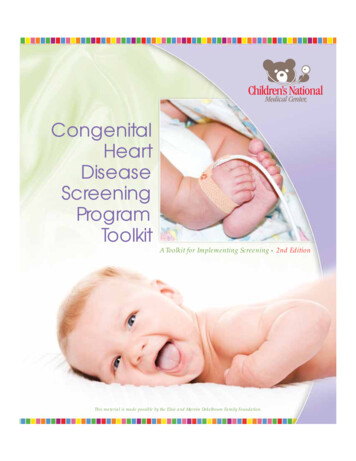
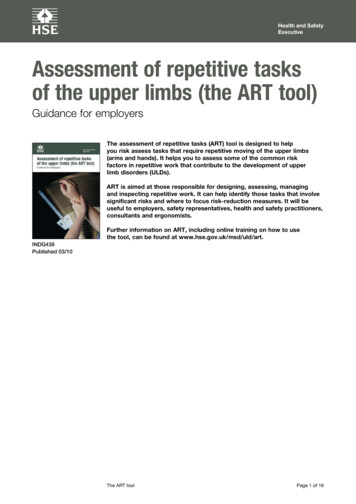
PASTOR : Data FlowPROMIS EnginePatient Self-EnteredPain RegistryAHLTAvia HAIMSPain Specialty Care &PCMH CareCoordinationPlan (CCP) and WorkflowPersonal Health RecordPatient ViewProvider View &Report generation
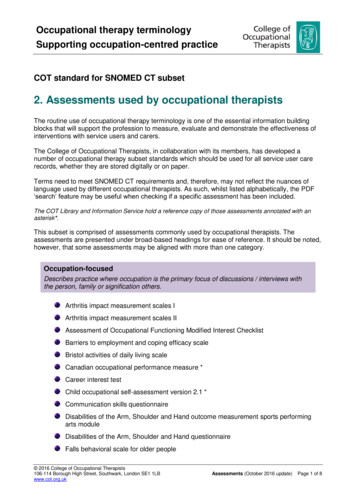
PASTOR CLINICAL REPORT Pain Mapped byRegion Clinical Alerts Patient Defined Goals
Gen population percentile indicator Color Coding on each graph
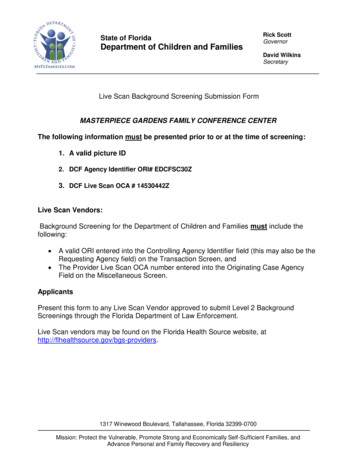
FUNCTIONAL RESTORATION PAIN PROGRAM
FUNCTIONAL RESTORATION PAIN PROGRAM* FRPP Booster carealigned to facilitatecontinued PCMHoriented management5. Start FRPP1. Patientreferred toFRPPInt/Ext –referralsEligibility Screen3. Patient scheduled forNCM FRPP intakegroup visit2. Patientsscheduled forIndividual teammember intakes4. Patient completes“Baseline”PASTOR-PLUSWeeks priortoFRPP Start* Referrals arefor active dutyonlyWeek priorFRPPNCM Intake8 week IOP6-10 patientsper cycleMedical MGMTMedicationsSleep TxPhysically reconditioningWork HardeningYoga/PilatesAquatic trainingMind Body MedicinePain Self-care trainingPain EducationCBT/ACTRecreation TherapyDay 1FRPPInterdisciplinaryTeam*Review PASTOR-PROMIS result*Integrate TeamIntake Evaluations*Determine Diagnosis*DevelopInterdisciplinaryTreatment Plan*Discuss Outcomesand treatment planwith patient7. Patient completes“FRPP complete”PASTOR-PLUSI. Post –program responsiblePCM identifiedII. FRPP discharge treatmentplan developed to supportcontinued care within PCMH6. Patient completes“Interim”PASTOR-PLUSWeek 4FRPPInterdisciplinaryTeam*Review PASTOR-PROMIS interimresults*Integrate findings* AdjustInterdisciplinaryTreatment Plan asneeded*Discuss Outcomesand treatment planwith patientWeek 8FRPP complete actionsvia patientDashboardHealth carecoaching8. Patients complete“FRPP Booster”PASTOR-PLUS viaweb @ 3, 6, 12monthsFRPP Boostersessions scheduledFRPPBoosterInterdisciplinaryTeam*Review PASTORPROMIS Boosterresults*Integrate findings* Interdisciplinaryteam develops boostertreatment plan*Discuss Outcomesand treatment planwith patient
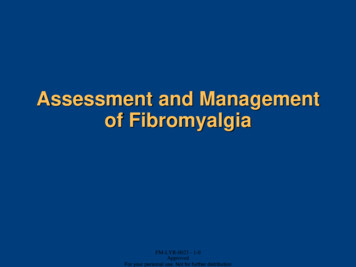
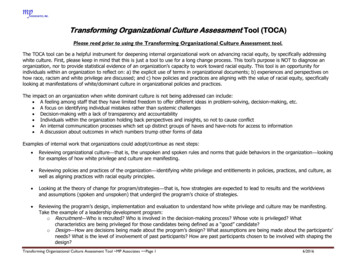
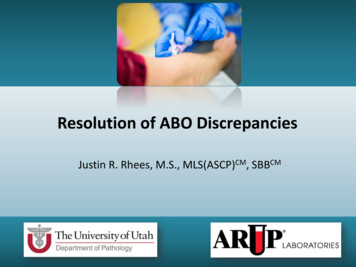
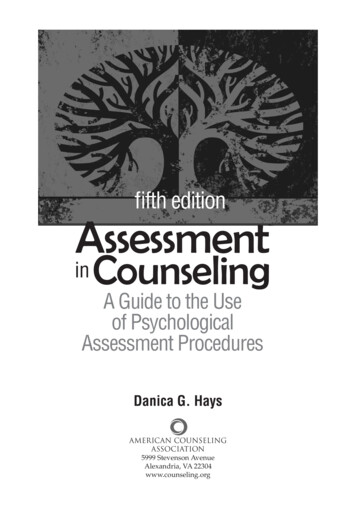
Preliminary Result of 33 Chronic Pain Patients at Balboa Undergoing treatment in theFunctional Restoration Program17
Tampa Scale of Kinesiophobia - TSK-11
Pain Catastrophizing Scale
Pain Catastrophizing Scale - subscales**Decrease in Measure Indicates Improvement**
PASTOR is in full production at Pilot sites Naval Medical Center San Diego Walter Reed Military Medical Center Madigan Army Medical CenterUnderway - Linking outpatient therapy and collaboration betweenthe specialty pain clinics and primary care - common language Medical Home Pain Champion and Pain Specialist TelePain ScanEcho21
CURRENT PROMIS END USERSWashington University Medical School, St. LouisVirginia Commonwealth UniversityUniversity of Washington, SeattleUniversity of Rochester, Center for Musculoskeletal ResearchUniversity of Maryland School of NursingUniversity College London, Health Behavior Research CentreNorthwestern University, Center for Psychosocial Research in GINewcastle University Medical School, Institute of Cellular Medicine,Newcastle, UKUniversity of UtahUniversity of MichiganUniversity of British ColumbiaRehaKlinikum Bad Säckingen GmbHMD Anderson Cancer CenterJewish General Hospital, Montreal (plus 14 other facilities),CanadaRAND CorporationHenry Ford Medical GroupMayo ClinicDurham Veterans Affairs Medical CenterMass GeneralClinic for Internal Medicine,Charite – Universitatsmedizin, BerlinIllinois State UniversityCase WesternAlbany Medical CollegeUCLA and VA GI ClinicsUniversity of Adelaide, AustraliaStony Brook Center for Pain ManagementOregon College of Oriental MedicineSumma Health SystemUniversity of Washington and CNICS HIV CareAMVETSStanford Pain ClinicCleveland Clinic
“In God we trust; all others must bring data.”W. Edwards Deming
Mayo Clinic . Durham Veterans Affairs Medical Center . Mass General . Clinic for Internal Medicine, Charite - Universitatsmedizin, Berlin . Illinois State University . Case Western . Albany Medical College . UCLA and VA GI Clinics . University of Adelaide, Australia . Stony Brook Center for Pain Management . Oregon College of Oriental Medicine