Transcription
The Lancet CommissionsDementia prevention, intervention, and care: 2020 report ofthe Lancet CommissionGill Livingston, Jonathan Huntley, Andrew Sommerlad, David Ames, Clive Ballard, Sube Banerjee, Carol Brayne, Alistair Burns,Jiska Cohen-Mansfield, Claudia Cooper, Sergi G Costafreda, Amit Dias, Nick Fox, Laura N Gitlin, Robert Howard, Helen C Kales, Mika Kivimäki,Eric B Larson, Adesola Ogunniyi, Vasiliki Orgeta, Karen Ritchie, Kenneth Rockwood, Elizabeth L Sampson, Quincy Samus, Lon S Schneider,Geir Selbæk, Linda Teri, Naaheed MukadamExecutive summaryThe number of older people, including those living withdementia, is rising, as younger age mortality declines.However, the age-specific incidence of dementia has fallenin many countries, probably because of improvements ineducation, nutrition, health care, and lifestyle changes.Overall, a growing body of evidence supports the ninepotentially modifiable risk factors for dementia modelledby the 2017 Lancet Commission on dementia prevention,intervention, and care: less education, hypertension,hearing impairment, smoking, obesity, depression, phy sical inactivity, diabetes, and low social contact. We now addthree more risk factors for dementia with newer, convincingevidence. These factors are excessive alcohol consumption,traumatic brain injury (TBI), and air pollution. We havecompleted new reviews and meta-analyses and incorporatedthese into an updated 12 risk factor life-course model ofdementia prevention. Together the 12 modifiable riskfactors account for around 40% of worldwide dementias,which consequently could theo retically be prevented ordelayed. The potential for prevention is high and mightbe higher in low-income and middle-income countries(LMIC) where more dementias occur.Our new life-course model and evidence synthesis hasparamount worldwide policy implications. It is never tooearly and never too late in the life course for demen tia prevention. Early-life (younger than 45 years) risks,such as less education, affect cognitive reserve; midlife(45–65 years), and later-life (older than 65 years) risk factorsinfluence reserve and triggering of neuropathologicaldevelopments. Culture, poverty, and inequality are keydrivers of the need for change. Individuals who are mostdeprived need these changes the most and will derive thehighest benefit.Policy should prioritise childhood education for all.Public health initiatives minimising head injury anddecreasing harmful alcohol drinking could potentiallyreduce young-onset and later-life dementia. Midlife sys tolic blood pressure control should aim for 130 mm Hg orlower to delay or prevent dementia. Stopping smoking,even in later life, ameliorates this risk. Passive smoking isa less considered modifiable risk factor for dementia.Many countries have restricted this exposure. Policymakers should expedite improvements in air quality,particularly in areas with high air pollution.We recommend keeping cognitively, physically, andsocially active in midlife and later life although littleevidence exists for any single specific activity protectingwww.thelancet.com Vol 396 August 8, 2020against dementia. Using hearing aids appears to reducethe excess risk from hearing loss. Sustained exercise inmidlife, and possibly later life, protects from dementia,perhaps through decreasing obesity, diabetes, andvascular risk. Depression might be a risk forcardio dementia, but in later life dementia might causedepression. Although behaviour change is difficult andsome associations might not be purely causal, individualshave a huge potential to reduce their dementia risk.In LMIC, not everyone has access to secondaryeducation; high rates of hypertension, obesity, andhearing loss exist, and the prevalence of diabetes andsmoking are growing, thus an even greater proportion ofdementia is potentially preventable.Amyloid-β and tau biomarkers indicate risk of progres sion to Alzheimer’s dementia but most people withnormal cognition with only these biomarkers neverdevelop the disease. Although accurate diagnosis is impor tant for patients who have impairments and functionalconcerns and their families, no evidence exists to supportpre-symptomatic diagnosis in everyday practice.Our understanding of dementia aetiology is shifting,with latest description of new pathological causes. In theoldest adults (older than 90 years), in particular, mixeddementia is more common. Blood biomarkers might holdpromise for future diagnostic approaches and are morescalable than CSF and brain imaging markers.Wellbeing is the goal of much of dementia care. Peoplewith dementia have complex problems and symptoms inmany domains. Interventions should be individualisedand consider the person as a whole, as well as their familycarers. Evidence is accumulating for the effectiveness, atleast in the short term, of psychosocial interventionstailored to the patient’s needs, to manage neuropsychiatricsymptoms. Evidence-based interventions for carers canreduce depressive and anxiety symptoms over years andbe cost-effective.Keeping people with dementia physically healthy isimportant for their cognition. People with dementiahave more physical health problems than others of thesame age but often receive less community health careand find it particularly difficult to access and organisecare. People with dementia have more hospitaladmissions than other older people, including forillnesses that are potentially manageable at home. Theyhave died disproportionately in the COVID-19 epidemic.Hospitalisations are distressing and are associated withpoor outcomes and high costs. Health-care professionalsLancet 2020; 396: 413–46Published OnlineJuly 30, ivision of Psychiatry(Prof G Livingston MD,J Huntley PhD, A Sommerlad PhD,Prof C Cooper PhD,S G Costafreda PhD,Prof R Howard MD, V Orgeta PhD,Prof E L Sampson MD,N Mukadam PhD), DementiaResearch Centre, UK DementiaResearch Institute(Prof N Fox MD), andDepartment of Epidemiologyand Public Health(Prof M Kivimäki FMedSci),University College London,London, UK; Camden andIslington NHS FoundationTrust, London, UK(Prof G Livingston, J Huntley,A Sommerlad, Prof C Cooper,S G Costafreda, Prof R Howard,N Mukadam); Barnet, Enfield,and Haringey Mental HealthTrust, London, UK(Prof E L Sampson); NationalAgeing Research Institute andAcademic Unit for Psychiatry ofOld Age, University ofMelbourne, Royal MelbourneHospital, Parkville, VIC,Australia (Prof D Ames MD);University of Exeter, Exeter, UK(Prof C Ballard MD); Faculty ofHealth: Medicine, Dentistry andHuman Sciences, University ofPlymouth, Plymouth, UK(Prof S Banerjee MD); CambridgeInstitute of Public Health,University of Cambridge,Cambridge, UK(Prof C Brayne MD); Departmentof Old Age Psychiatry,University of Manchester,Manchester, UK(Prof A Burns MD); Departmentof Health Promotion, Schoolof Public Health, SacklerFaculty of Medicine(Prof J Cohen-Mansfield PhD),Heczeg Institute on Aging(Prof J Cohen-Mansfield),and Minerva Center forInterdisciplinary Study of Endof Life (Prof J Cohen-Mansfield),413
The Lancet CommissionsTel Aviv University, Tel Aviv,Israel; Department ofPreventive and SocialMedicine, Goa Medical College,Goa, India (A Dias MD);Institute of Neurology,National Hospital forNeurology and Neurosurgery,University College LondonHospitals NHS FoundationTrust, London, UK (Prof N Fox);Center for Innovative Care inAging (Prof L N Gitlin PhD), andDepartment of Psychiatryand Behavioral Sciences(Q Samus PhD), Johns HopkinsUniversity, Baltimore, MA,USA; Department ofPsychiatry and BehavioralSciences, UC Davis School ofMedicine, University ofCalifornia, Sacramento, CA,USA (Prof H C Kales MD); KaiserPermanente WashingtonHealth Research Institute,Seattle, WA, USA(Prof E B Larson MD);University College Hospital,Ibadan, Nigeria(Prof A Ogunniyi MBChB);Inserm, Unit 1061,Neuropsychiatry:Epidemiological and ClinicalResearch, La ColombièreHospital, University ofMontpellier, Montpellier,France (Prof K Ritchie PhD);Centre for Clinical BrainSciences, University ofEdinburgh, Edinburgh, UK(Prof K Ritchie); Centre for theHealth Care of Elderly People,Geriatric Medicine DalhousieUniversity, Halifax, NS, Canada(Prof K Rockwood MD);Department of Psychiatry andthe Behavioural Sciences andDepartment of Neurology,Keck School of Medicine,Leonard Davis School ofGerontology of the Universityof Southern California,Los Angeles, CA, USA(Prof L S Schneider MD);Norwegian National AdvisoryUnit on Ageing and Health,Vestfold Hospital Trust,Tønsberg, Norway(Prof G Selbæk MD); Instituteof Clinical Medicine, Faculty ofMedicine, University of Oslo,Oslo, Norway (Prof G Selbæk);Geriatric Department, OsloUniversity Hospital, Oslo,Norway (Prof G Selbæk);Department Psychosocial andCommunity Health, School ofNursing, University ofWashington, Seattle, WA, USA(Prof L Teri PhD)414Key messages Three new modifiable risk factors for dementia New evidence supports adding three modifiable riskfactors—excessive alcohol consumption, head injury,and air pollution—to our 2017 Lancet Commission ondementia prevention, intervention, and care life-coursemodel of nine factors (less education, hypertension,hearing impairment, smoking, obesity, depression,physical inactivity, diabetes, and infrequent socialcontact). Modifying 12 risk factors might prevent or delay up to40% of dementias. Be ambitious about prevention Prevention is about policy and individuals.Contributions to the risk and mitigation of dementiabegin early and continue throughout life, so it is nevertoo early or too late. These actions require both publichealth programmes and individually tailoredinterventions. In addition to population strategies,policy should address high-risk groups to increasesocial, cognitive, and physical activity; and vascularhealth. Specific actions for risk factors across the life course Aim to maintain systolic BP of 130 mm Hg or less inmidlife from around age 40 years (antihypertensivetreatment for hypertension is the only known effectivepreventive medication for dementia). Encourage use of hearing aids for hearing loss andreduce hearing loss by protection of ears from excessivenoise exposure. Reduce exposure to air pollution and second-handtobacco smoke. Prevent head injury. Limit alcohol use, as alcohol misuse and drinking morethan 21 units weekly increase the risk of dementia. Avoid smoking uptake and support smoking cessationto stop smoking, as this reduces the risk of dementiaeven in later life. Provide all children with primary and secondaryeducation.should consider dementia in older people withoutknown dementia who have frequent admissions or whodevelop delirium. Delirium is common in people withdementia and contributes to cognitive decline. Inhospital, care including appropriate sensory stimulation,ensuring fluid intake, and avoiding infections mightreduce delirium incidence.Acting now on dementia prevention, intervention, andcare will vastly improve living and dying for individualswith dementia and their families, and thus society.IntroductionWorldwide around 50 million people live with dementia,and this number is projected to increase to 152 million Reduce obesity and the linked condition of diabetes.Sustain midlife, and possibly later life physical activity. Addressing other putative risk factors for dementia,like sleep, through lifestyle interventions, will improvegeneral health. Tackle inequality and protect people with dementia Many risk factors cluster around inequalities, which occurparticularly in Black, Asian, and minority ethnic groupsand in vulnerable populations. Tackling these factors willinvolve not only health promotion but also societalaction to improve the circumstances in which people livetheir lives. Examples include creating environments thathave physical activity as a norm, reducing the populationprofile of blood pressure rising with age through betterpatterns of nutrition, and reducing potential excessivenoise exposure. Dementia is rising more in low-income and middleincome countries (LMIC) than in high-income countries,because of population ageing and higher frequency ofpotentially modifiable risk factors. Preventativeinterventions might yield the largest dementiareductions in LMIC.For those with dementia, recommendations are: Provide holistic post-diagnostic care Post-diagnostic care for people with dementia shouldaddress physical and mental health, social care, andsupport. Most people with dementia have other illnessesand might struggle to look after their health and thismight result in potentially preventable hospitalisations. Manage neuropsychiatric symptoms Specific multicomponent interventions decreaseneuropsychiatric symptoms in people with dementiaand are the treatments of choice. Psychotropic drugs areoften ineffective and might have severe adverse effects. Care for family carers Specific interventions for family carers have long-lastingeffects on depression and anxiety symptoms, increasequality of life, are cost-effective and might save money.by 2050,1 rising particularly in low-income and middleincome countries (LMIC) where around two-thirds ofpeople with dementia live.1 Dementia affects individuals,their families, and the economy, with global costsestimated at about US 1 trillion annually.1We reconvened the 2017 Lancet Commission ondementia prevention, intervention, and care2 to identifythe evidence for advances likely to have the greatestimpact since our 2017 paper and build on its work. Ourinter disciplinary, international group of experts presented,debated, and agreed on the best available evidence.We adopted a triangulation framework evaluating theconsistency of evidence from different lines of researchand used that as the basis to evaluate evidence. We havewww.thelancet.com Vol 396 August 8, 2020
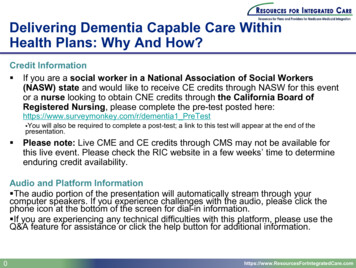
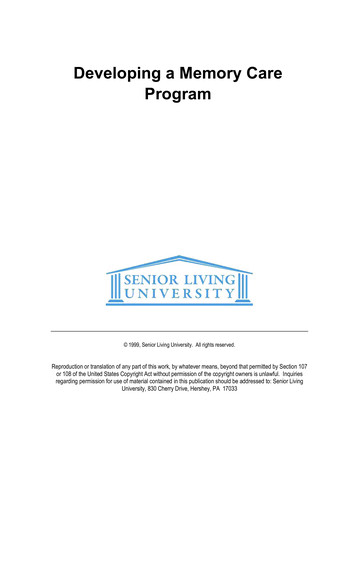
The Lancet Commissionssummarised best evidence using, where possible, goodquality systematic reviews, meta-analyses, or individualstudies, where these add important knowledge to thefield. We performed systematic literature reviews andmeta-analyses where needed to generate new evidence forour analysis of potentially modifiable risk factors fordementia. Within this framework, we present a narrativesynthesis of evidence including systematic reviews andmeta-analyses and explain its balance, strengths, andlimitations. We evaluated new evidence on dementia riskin LMIC; risks and protective factors for dementia; detec tion of Alzheimer’s disease; multimorbidity in dementia;and interventions for people affected by dementia.Nearly all the evidence is from studies in highincome countries (HIC), so risks might differ in othercountries and interventions might require modificationfor different cultures and environments. This notion alsounderpins the critical need to understand the dementiasrelated to life-course disadvantage—whether in HICs orLMICs.Our understanding of dementia aetiology is shifting.A consensus group, for example, has described hippo campal sclerosis associated with TDP-43 proteinopathy,as limbic-predominant age-related TDP-43 encepha lopathy (LATE) dementia, usually found in people olderthan 80 years, progressing more slowly than Alzheimer’sdisease, detectable at post-mortem, often mimicking orcomorbid with Alzheimer’s disease.3 This situationreflects increasing attention as to how clinical syndromesare and are not related to particular underlying patho logies and how this might change across age. More workis needed, however, before LATE can be used as a validclinical diagnosis.The fastest growing demographic group in HIC is theoldest adults, those aged over 90 years. Thus a uniqueopportunity exists to focus on both human biology, inthis previously rare population, as well as on meetingtheir needs and promoting their wellbeing.Prevention of dementiaThe number of people with dementia is rising.Predictions about future trends in dementia prevalencevary depending on the underlying assumptions andgeographical region, but generally suggest substantialincreases in overall prevalence related to an ageingpopulation. For example, according to the GlobalBurden of Diseases, Injuries, and Risk Factors Study,the global age-standardised prevalence of dementiabetween 1990 and 2016 was relatively stable, but with anageing and bigger population the number of peoplewith dementia has more than doubled since 1990.4However, in many HIC such as the USA, the UK, andFrance, age-specific incidence rates are lower in morerecent cohorts compared with cohorts from previousdecades collected using similar methods and targetpopulations5 (figure 1) and the age-specific incidenceof dementia appears to decrease.6 All-cause dementiawww.thelancet.com Vol 396 August 8, 2020incidence is lower in people born more recently,7 proba blydue to educational, socio-economic, health care, and life style changes.2,5 However, in these countries increasingobesity and diabetes and declining physical activitymight reverse this trajectory.8,9 In contrast, age-specificdementia prevalence in Japan, South Korea, Hong Kong,and Taiwan looks as if it is increasing, as is Alzheimer’sin LMIC, although whether diagnostic methods arealways the same in comparison studies is unclear.5–7Modelling of the UK change suggests a 57% increase inthe number of people with dementia from 2016 to 2040,70% of that expected if age-specific incidence ratesremained steady,10 such that by 2040 there will be1·2 million UK people with dementia. Models alsosuggest that there will be future increases both in thenumber of individuals who are independent and thosewith complex care needs.6PopulationCorrespondence to:Prof Gill Livingston, Division ofPsychiatry, University CollegeLondon, London W1T 7NF, UKg.livingston@ucl.ac.ukHazard ratioincidence ratio (95%CI)Rotterdam (age 60–90 years)2000 vs 1990Total0·8 (0·6–1·0)2000 vs 1990Men0·7 (0·4–1·2)2000 vs 1990Women0·8 (0·5–1·1)Bordeaux (clinical diagnosis, age 65 years)1999 vs 1988Total0·9 (0·7–1·1)1999 vs 1988Men1·2 (0·8–1·9)1999 vs 1988Women0·9 (0·7–1·2)Bordeaux (algorithmic diagnosis, age 65 years}1999 vs 1988Total0·6 (0·5–0·8)1999 vs 1988Men1·1 (0·7–1·8)1999 vs 1988Women0·6 (0·5–0·8)2008 vs 1991Total0·8 (0·6–1·0)2008 vs 1991Men0·6 (0·4–0·9)2008 vs 1991Women1·0 (0·7–1·3)CFAS (age 65 years)IIDP (African American age 70 years)2001 vs 1992Total0·4 (0·3–0·5)Total0·8 (0·6–1·1)IIDP (Yoruba age 70 years)2001 vs 1992Framingham heart study (age 60 years)1986–91 vs 1977–83Total0·8 (0·6–1·0)1992–98 vs 1977–83Total0·6 (0·5–0·8)2004–08 vs 1977–83Total0·6 (0·4–0·8)1986–91 vs 1977–83Men1·0 (0·6–1·6)1992–98 vs 1977–83Men0·9 (0·6–1·4)2004–08 vs 1977–83Men0·6 (0·4–1·1)1986–91 vs 1977–83Women0·7 (0·5–1·0)1992–98 vs 1977–83Women0·5 (0·4–0·7)2004–08 vs 1977–83Women0·5 (0·4–0·8)0·250·51·02·04·0Decreased incident Increased incidentdementia dementiaFigure 1: Incidence rate ratio comparing new cohorts to old cohorts from five studies of dementia incidence5IIDP Project in USA and Nigeria, Bordeaux study in France, and Rotterdam study in the Netherlands adjusted forage. Framingham Heart Study, USA, adjusted for age and sex. CFAS in the UK adjusted for age, sex, area, anddeprivation. However, age-specific dementia prevalence is increasing in some other countries. IID Indianapolis–Ibadan Dementia. CFAS Cognitive Function and Ageing Study. Adapted from Wu et al,5 by permission of SpringerNature.415
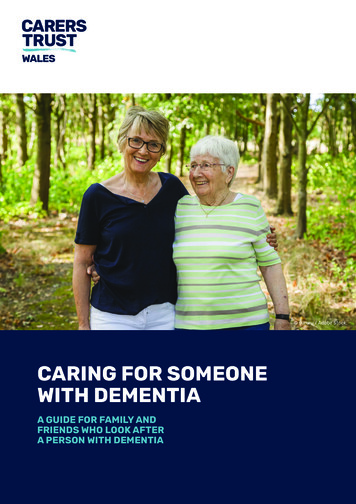
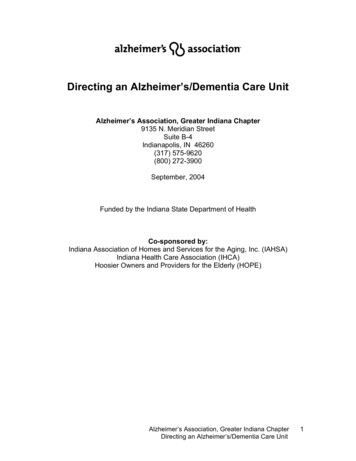
The Lancet CommissionsIn our first report, the 2017 Commission described alife-course model for potentially modifiable risks fordementia.2 Life course is important when consideringrisk, for example, obesity and hypertension in midlifepredict future dementia, but both weight and bloodpressure usually fall in later life in those with or dev eloping dementia,9 so lower weight and blood pressurein later life might signify illness, not an absence ofrisk.11–14 We consider evidence on other potential riskfactors and incor porate those with good quality evidencein our model.Figure 2 summarises possible mechanisms of protec tion from dementia, some of which involve increasingor maintaining cognitive reserve despite pathology andneuropathological damage. There are different termsdescribing the observed differential susceptibility to agerelated and disease-related changes and these are notused consistently.15,16 A consensus paper defines reserveas a concept accounting for the difference between anindividual’s clinical picture and their neuropathology.It, divides the concept further into neurobiologicalbrain reserve (eg, numbers of neurones and synapses at agiven timepoint), brain maintenance (as neurobiologicalcapital at any timepoint, based on genetics or lifestylereducing brain changes and pathology developmentover time) and cognitive reserve as adaptability enablingpreser vation of cognition or everyday functioning inspite of brain pathology.15 Cognitive reserve is changeableand quantifying it uses proxy measures such as educa tion, occupational complexity, leisure activity, residualapproaches (the variance of cognition not explained bydemographic variables and brain measures), or identi fication of functional networks that might underlie suchreserve.15–20Early-life factors, such as less education, affect theresulting cognitive reserve. Midlife and old-age risk factorsinfluence age-related cognitive decline and triggering ofneuropathological developments. Consistent with thehypothesis of cognitive reserve is that older women aremore likely to develop dementia than men of the same Minimise diabetes Treat hypertension Prevent head injury Stop smoking Reduce air pollution Reduce midlife obesityReduced neuropathologicaldamage (amyloid ortau-mediated, vascular orinflammatory) Mantain frequent exercise Reduce occurrence of depression Avoid excessive alcohol Treat hearing impairment Mantain frequent social contact Attain high level of educationPreventing dementiaIncreased and maintainedcognitive reserveFigure 2: Possible brain mechanisms for enhancing or maintaining cognitive reserve and risk reduction ofpotentially modifiable risk factors in dementia416age, probably partly because on average older women havehad less education than older men. Cognitive reservemechanisms might include preserved metabolism orincreased connectivity in temporal and frontal brainareas.17–21 People in otherwise good physical health cansustain a higher burden of neuropathology withoutcognitive impairment.22 Culture, poverty, and inequalityare important obstacles to, and drivers of, the need forchange to cognitive reserve. Those who are most deprivedneed these changes the most and will derive the highestbenefit from them.Smoking increases air particulate matter, and hasvascular and toxic effects.23 Similarly air pollution mightact via vascular mechanisms.24 Exercise might reduceweight and diabetes risk, improve cardiovascular func tion, decrease glutamine, or enhance hippocampalneurogenesis.25 Higher HDL cholesterol might protectagainst vascular risk and inflammation accompanyingamyloid-β (Aβ) pathology in mild cognitive impairment.26Dementia in LMICNumbers of people with dementia in LMIC are risingfaster than in HIC because of increases in life expectancyand greater risk factor burden. We previously calculatedthat nine potentially modifiable risk factors togetherare associated with 35% of the population attributablefraction (PAFs) of dementia worldwide: less education,high blood pressure, obesity, hearing loss, depression,diabetes, physical inactivity, smoking, and social isola tion, assuming causation.2 Most research data for thiscalcu lation came from HIC and there is a relative absenceof specific evidence of the impact of risk factors ondementia risk in LMIC, particularly from Africa andLatin America.27Calculations considering country-specific prevalence ofthe nine potentially modifiable risk factors indicate PAFof 40% in China, 41% in India and 56% in Latin Americawith the potential for these numbers to be even higherdepending on which estimates of risk factor frequencyare used.28,29 Therefore a higher potential for dementiaprevention exists in these countries than in globalestimates that use data predominantly from HIC. If notcurrently in place, national policies addressing access toeducation, causes and management of high bloodpressure, causes and treatment of hearing loss, socioeconomic and commercial drivers of obesity, could beimplemented to reduce risk in many countries. Thehigher social contact observed in the three LMIC regionsprovides potential insights for HIC on how to influencethis risk factor for dementia.30 We could not considerother risk factors such as poor health in pregnancyof malnourished mothers, difficult births, early lifemalnutrition, survival with heavy infection burdensalongside malaria and HIV, all of which might add tothe risks in LMIC.Diabetes is very common and cigarette smokingis rising in China while falling in most HIC.31 Awww.thelancet.com Vol 396 August 8, 2020
The Lancet Commissionsmeta-analysis found variation of the rates of dementiawithin China, with a higher prevalence in the north andlower prevalence in central China, estimating 9·5 millionpeople are living with dementia, whereas a slightly latersynthesis estimated a higher prevalence of around11 million.30,32 These data highlight the need for morefocused work in LMIC for more accurate estimates ofrisk and interventions tailored to each setting.Specific potentially modifiable risk factors fordementiaRisk factors in early life (education), midlife (hypertension,obesity, hearing loss, TBI, and alcohol misuse) and laterlife (smoking, depression, physical inactivity, socialisolation, diabetes, and air pollution) can contribute toincreased dementia risk (table 1). Good evidence existsfor all these risk factors although some late-life factors,such as depression, possibly have a bidirectional impactand are also part of the dementia prodrome.33,34In the next section, we briefly describe relevant newlypublished and illustrative research studies that add tothe 2017 Commission’s evidence base, including risksand, for some, mitigation. We have chosen studiesthat are large and representative of the populations, orsmaller studies in areas where very little evidence exists.We discuss them in life-course order and within thelife course in the order of magnitude of populationattributable factor.Education and midlife and late-life cognitive stimulationEducation level reachedHigher childhood education levels and lifelong highereducational attainment reduce dementia risk.2,35–37 Newwork suggests overall cognitive ability increases, witheducation, before reaching a plateau in late adoles cence, when brain reaches greatest plasticity; withrelatively few further gains with education afterage 20 years.38 This suggests cognitive stimulation ismore important in early life; much of the apparentlater effect might be due to people of higher cognitivefunction seeking out cognitively stimulating activitiesand education.38 It is difficult to separate out thespecific impact of education from the effect of overallcognitive ability,38,39 and the specific impact of later-lifecognitive activity from lifelong cognitive function andactivity.39,40Cognitive maintenanceOne large study in China tried to separate cognitiveactivity in adulthood from activities for those with moreeducation, by considering activities judged to appeal topeople of different levels of education.40 It found peopleolder than 65 years who read, played games, or betmore frequently had reduced risk of dementia (n 15 882,odds ratio [OR] 0·7, 95% CI 0·6–0·8). The studyexcluded people developing dementia less than 3 yearsafter baseline to reduce reverse causation.www.thelancet.com Vol 396 August 8, 2020Relative risk for Risk factorprevalencedementia(95% CI)Communality UnweightedPAFWeightedPAF*1·6 (1·3–2·0)40·0%61·2%19·4%7·1%Early life ( 45 years)Less educationMidlife (age 45–65 years)Hearing loss1·9 (1·4–2·7)31·7%45·6%22·2%8·2%TBI1·8 6 (1·2–2·2)8·9%68·3%5·1%1·9%Alcohol ( 21 units/week) 1·2 (1·1–1·3)11·8%73·3%2·1%0·8%1·6 (1·3–1·9)3·4%58·5%2·0%0·7%Smoking1·6 (1·2–2·2)27·4%62·3%14·1%5·2%Depression1·9 (1·6–2·3)13·2%69·8%10·6%3·9%Social isolation1·6 (1·3–1·9)11·0%28·1%4·2%3·5%Physical inactivity1·4 (1·2–1·7)17·7%55·2%9·6%1·6%Diabetes1·5 (1·3–1·8)6·4%71·4%3·1%1·1%Air pollution1·1 (1·1–1·1)75·0%13·3%6·3%2·3%Obesity (body-massindex 30)Later life (age 65 years)Data are relative risk (95% CI) or %. Overall weighted PAF 39·7%. PAF population attributable fraction. TBI traumaticbrain injury. *Weighted PAF is the relative contribution of each risk factor to the overall PAF when adjusted forcommunality.Table 1: PAF for 12 dementia risk factorsThis finding is consistent with small studies of midlifeactivities which find them associated with better late-lifecognition; so for example, in 205 people aged 30–64 years,followed up until 66–88 years, travel, social outings,playing music, art, physical activity, reading, and speakinga second language, were associated with maintainingcognition, independent of education, occupation, late-lifeactivities, and current structural brain health.41 Similarly,engaging in intellectual activity as adults, particularlyproblem solving, for 498 people born in 1936, was associ ated with cognitive ability acquisition, although not thespeed of decline.42Cognitive declineThe use it or lose it hypothesis suggests that mentalactivity, in general, might improve cognitive function.People in more cognitively demanding jobs tend toshow less cognitive deterioration before, and sometimesafter retirement than those in less demanding jobs.43,44One systematic review of retirement and cognitivedecline found conflicting evidence.45 Subsequently, a12-year study of 1658 people found older retirement agebut not number of years working, was associated withlower dementia risk.46 Those retiring because of ill healthhad lower verbal memory and fluency scores than thoseretiring for other reasons.47 Anothe
physical inactivity, diabetes, and infrequent social contact). Modifying 12 risk factors might prevent or delay up to 40% of dementias. Be ambitious about prevention Prevention is about policy and individuals. Contributions to the risk and mitigation of dementia begin early and continue throughout life, so it is never