Transcription
EFFECTIVELY ADDRESSINGCO-OCCURRING ADDICTION & PTS/D
TRAUMA DEFINEDExposure to actual or threatened death, serious injury,or sexual violence in one or more of the followingways: Directly experiencing;Directly witnessing;Learning that traumatic event(s) occurred to a loved one;Repeated/extreme exposure to aversive details of traumaticevents.
TRAUMATIC EVENTSINCLUDE: War, battles, combat (death, explosions, gunfire ) Natural disasters (floods, tornados, fires ) Catastrophe (harmful/fatal accidents, terrorism) Violent attack (animal attack, assault with or without a weapon,battery and domestic violence, rape, threats of bodily harm with orwithout a weapon) Abuse (physical, sexual, mental and/or verbal) Directly or indirectly witnessing any of the above
THE ACE STUDY ACE Adverse Childhood Experiences http://www.acestudy.org/ Studied the relationship between multiple categories ofchildhood trauma (ACEs), and health and behavioraloutcomes later in life Largest study of its kind (17,421 subjects)
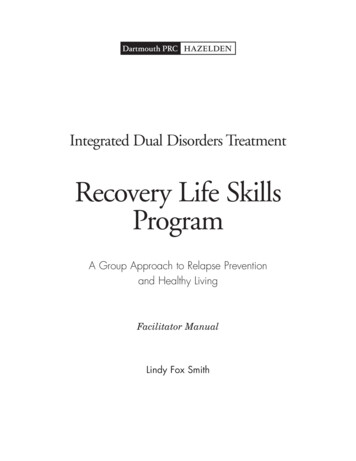
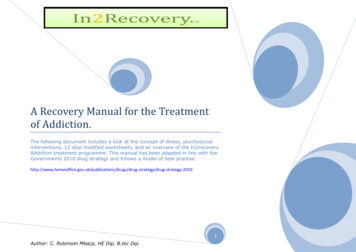
ADVERSE CHILDHOOD EXPERIENCES(ACES) ARE COMMONHousehold dysfunction:Substance abuseParental sep/divorceMental illnessBattered motherCriminal se:PsychologicalPhysicalSexual15%10%11%28%21%5
WHAT ARE CONSIDERED ACES?1.Recurrent physical abuse2.Recurrent emotional abuse3.6.Household member chronicallydepressed, mentally ill, institutionalized,or suicidalContact sexual abuse7.Mother treated violently4.Lack of adequate love or support8.One or no parents5.An alcohol and/or drug abuser inthe household9.Emotional or physical neglect10.Incarcerated family member
NADINE BURKE HARRIS, M.D.Childhood trauma isn’t something you just get over as you grow up. Pediatrician Nadine BurkeHarris explains that the repeated stress of abuse, neglect, and parents struggling with mentalhealth or substance abuse issues has real, tangible effects on the development of the brain.https://www.youtube.com/watch?v 95ovIJ3dsNk
HOW DO PEOPLE REACT TO TRAUMA? PTSD: Posttraumatic Stress Disorder – nowcharacterized (DSM-5) by four clusters of symptoms . . .① INTRUSIVE symptoms② AVOIDANCE symptoms③ NEGATIVE COGNITIVE/MOOD ALTERATIONS④ AROUSAL/REACTIVITY symptomsFrom “Anxiety Dis ord er” to “Tra um a - a nd Stres s or-Rela ted Dis ord er”
INTRUSIVE SYMPTOMS (PCL-5)(WEATHERS ET AL, 2013)1. Repeated, disturbing, and unwanted memories of the stressful experience?2. Repeated, disturbing dreams of the stressful experience?3. Suddenly feeling or acting as if the stressful experience were actually happeningagain (as if you were actually back there reliving it?)4. Feeling very upset when something reminded you of the stressful experience?5. Having strong physical reactions when something reminded you of the stressfulexperience (for example, heart pounding, trouble breathing, sweating)?
AVOIDANCE SYMPTOMS (PCL-5)(WEATHERS ET AL, 2013)6. Avoiding memories, thoughts, or feelings related tothe stressful experience?7. Avoiding external reminders of the stressfulexperience (for example, people, places, conversations,activities, objects, or situations)?
NEGATIVE COGNITIVE/MOOD ALTERATION SYMPTOMS (PCL-5)(WEATH ERS ET AL, 2013)8. Trouble remembering important parts of the stressful experience?9. Having strong negative beliefs about yourself, other people, or the world (for example, havingthoughts such as: I am bad, there is something seriously wrong with me, no one can be trusted, theworld is completely dangerous)?10.Blaming yourself or someone else for the stressful experience or what happened after it?11.Having strong negative feelings such as fear, horror, anger, guilt, or shame?12.Loss of interest in activities that you used to enjoy?13.Feeling distant or cut off from other people?14.Trouble experiencing positive feelings (for example, being unable to feel happiness or have lovingfeelings for people close to you)?
AROUSAL/REACTIVE SYMPTOMS (PCL-5)(WEATHERS ET AL, 2013)15. Irritable behavior, angry outbursts, or acting aggressively?16. Taking too many risks or doing things that could cause you harm?17. Being “superalert” or watchful or on guard?18. Feeling jumpy or easily startled?19. Having difficulty concentrating?20. Trouble falling or staying asleep?
PCL-5 SCORING(PAS T MONTH , ALS O EVALUAT E IMPACT ON LE V E L OF FUNC T IONIN G )For each item: Not at all 0; A little bit 1; Moderately 2; Quite a bit 3; Extremely 4.A provisional PTSD diagnosis can be made iffthe following 2 1 Intrusive symptom (q 1-5), 1 Avoidant (q 6-7), 2 Cognitive/Affective (q 8-14), 2 Arousal (q 15-20).Preliminary validation work is sufficient to make initial cut-point suggestions, but may besubject to change. A PCL-5 cut-point of 33 appears to be a reasonable value topropose until further psychometric work is available.
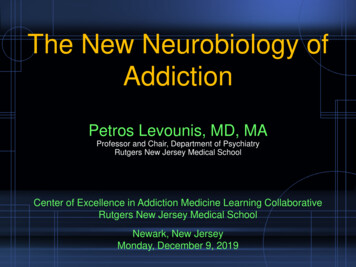
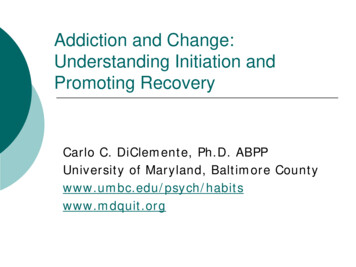
ACE S co re s Pre d ict Dru g Ab u s ePercent With Health Problem (%)14ACE Score1201234 51086420Eve r h a d ad ru g p ro b le mEve r a d d ict e dt o d ru g sEve r in je ct e dd ru g s
Men andWomen withACE scores 4are more than 3times morelikely to havedepression thanthose with anACE score of 0.
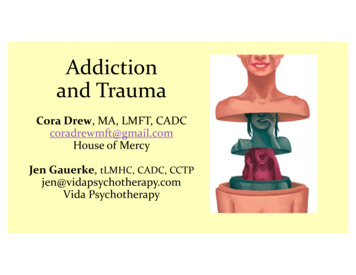
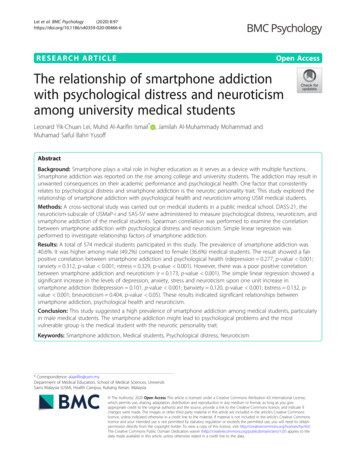
With 0 ACES,1 in 16 smokes,1 in 14 has heartdiseaseNo ACEs 1 in 69 is alcoholic; 1 in 480 uses IV drugs33% 1 in 96 has attempted suicide With 3 ACES, 1 in 9 smokes, 1 in 7 heart disease1-3 ACEs 1 in 9 is alcoholic, 1 in 43 uses IV drugs51% 1 in 10 has attempted suicide4-10ACEs16% With 7 ACEs, 1 in 6 smokes, 1 in 6 has heartdisease 1 in 6 is alcoholic, 1 in 30 uses IV drugs 1 in 5 has attempted suicide
OTHER FINDINGS OF THE ACE STUDY ACE score of 6 and higher – an almost 20-year shortening of lifespan. ACE score of 4 – 260% more likely to have Chronic Obstructive Pulmonary Disorder(COPD) than a person with an ACE Score of 0. ACE score of at least 7 – increased the likelihood of childhood/adolescent suicideattempts 51-fold and adult suicide attempts 30-fold. ACE scores of 4 or higher – increases the chance of having self-acknowledgedalcoholism as an adult by 500% (with a history of parental alcoholism). ACE scores of 4 or more – 12 times more likely to have attempted suicide, 7 timesmore likely to be alcoholic, and 10 times more likely to have injected street drugs.
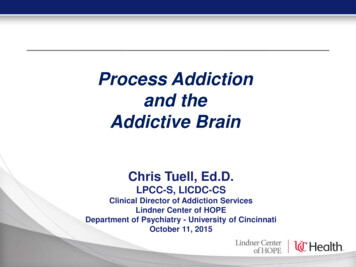
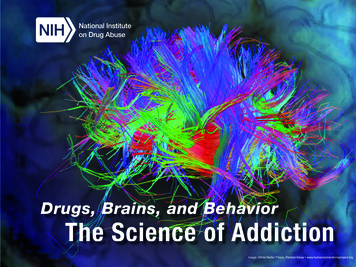
DeathEa rlyDe a t hDis e a s e , Dis a b ilit ya n d S o cia l Pro b le m sAd o p t io n o fHe a lt h -ris k Be h a vio rsS o cia l, Em o t io n a l, &Co g n it ive Im p a irm e n tAd ve rs e Ch ild h o o d Exp e rie n ce sConception
PREVALENCE OF PTSD IN CODPOPULATIONS In multiple national studies a high percentage of individualspresenting for addictions treatment were found to meet criteriafor a co-occurring PTSD diagnosis (Najavits, 2002). Studies from the ‘90s found 12%-59% co-prevalence; More recent studies found even higher co-prevalence rates. Higher percentages for females than for males.
PREVALENCE OF PTSD IN CODPOPULATIONS At Foundations Detroit, of all patients presenting for outpatient treatment,the following findings occurred: Average overall incoming PCL-5 score of 31 Female average score 42 Male average score 21 71% of female patients scored above the PTSD cutoff threshold; 21% of male patients scored above the PTSD cutoff threshold.
TRAUMA-SPECIFICTREATMENT MODELS Seeking Safety Trauma Recovery and Empowerment Model(TREM, M-TREM, G-TREM) Cognitive Behavioral Therapies (CBT/CPT) Prolonged Exposure Therapy (PET) Eye Movement Desensitization andReprocessing (EMDR)
TRAUMA-SPECIFICPhase IIPhase ITREMCBT/CPTEMDRSeekingSafetyPET
TRAUMA-SPECIFIC – PHASE 1Phase ITREMSeekingSafety
TREM: Part 1(Maxine Harris & Roger Fallot; Community Connections,Washington DC)Empowerment1.2.3.4.5.6.7.8.9.10.11.Introductory SessionWhat It Means to Be a WomanWhat Do You Know and How Do You FeelAbout Your Body?Physical BoundariesEmotional Boundaries: Setting Limits andAsking for What You WantSelf-EsteemDeveloping Ways to Feel Better: SelfSoothingIntimacy and TrustFemale SexualitySex with a PartnerTransition Session from Empowerment toTrauma Recovery1.Introduction2.Safety3.PTSD: Taking Back Your Power4.Detaching from Emotional Pain5.When Substances Control You6.Asking for Help7.Taking Good Care of Yourself8.Compassion9.Red and Green Flags10.Honesty11.Recovery Thinking12.Integrating the Split Self13.Commitment
TREM: Part 2(Maxine Harris & Roger Fallot; Community Connections,Washington DC)Trauma Recovery14.Creating Meaning12.Gaining an Understanding of Trauma15.Community Resources13.The Body Remembers What the MindForgets16.Setting Boundaries in Relationships17.Discovery18.Getting Others to Support Your Recovery19.Coping with Triggers20.Respecting Your Time21.Healthy Relationships22.Self-Nurturing23.Healing from Anger24.The Life Choices Game (Review)25.Termination14.What Is Physical Abuse?15.What Is Sexual Abuse?16.Physical Safety17.What Is Emotional Abuse?18.Institutional Abuse19.Abuse and Psychological or EmotionalSymptoms20.Trauma and Addictive or CompulsiveBehavior21.Abuse and Relationships
TREM: Parts 3 & 4(Maxine Harris & Roger Fallot; Community Connections, Washington DC)Advanced Trauma Recovery Issues22.23.24.25.26.27.Family: Myths and DistortionsFamily Life: CurrentDecision Making: Trusting YourJudgmentCommunication: Making YourselfUnderstoodSelf-Destructive BehaviorsBlame, Acceptance, and ForgivenessClos ing Ritua ls31.32.33.28.29.30.Feeling Out of ControlRelationshipsPersonal HealingTruths a nd MythsAb out Ab us eWha t It Mea ns toBe a Wom a nClos ing Ritua l
TRAUMA-SPECIFIC – PHASE iteboards.asp [1:17 min]Phase IIEMDRCBT/CPTPET
deos/whiteboards.asp [3:45 min]
E.M.D.R. Eye Movement Desensitization and Reprocessing (EMDR) is a one-onone form of psychotherapy that is designed to reduce trauma-relatedstress, anxiety, and depression symptoms associated with posttraumaticstress disorder (PTSD) and to improve overall mental healthfunctioning. The target traumatic memory for the treatment session is accessedwith attention to image, negative belief, and body sensations.
E.M.D.R. Repetitive 30-second dual-attention exercises are conducted in which theclient attends to a motor task while focusing on the target traumaticmemory and then on any related negative thoughts, associations, and bodysensations. The most common motor task used in EMDR is side-to-side eyemovements that follow the therapist's finger; however, alternating handtapping or auditory tones delivered through headphones can be used.
CBT/CPT FOR TRAUMAAutomaticthought CBT Distinctives1. Cognitive-Behavioral ModelEmotionalreaction2. Behavior Chain AnalysisBEHAVIORALRESPONSE3. als/videos/whiteboards.asp [2:40 min]
CBT: THE COGNITIVE-BEHAVIORAL ngBehavioraldisposition
2. Chain Analysis of Target Behavior#SCE chicagosummitconference.com
PROLONGED EXPOSURE eos/whiteboards.asp [2:44 min]
PROLONGED EXPOSURE THERAPY FOR PTSD IS A theoretically-based and highly efficacioustreatment for chronic PTSD and relateddepression, anxiety, and anger; Empirically validated with more than 20 yearsof research supporting its use;
PROLONGED EXPOSURE THERAPY FOR PTSD IS A flexible therapy that can be modified to fit theneeds of individual clients; Specifically designed to help clients process traumaticevents and reduce trauma-induced psychologicaldisturbances; A treatment that produces clinically significantimprovement in about 80% of patients with chronicPTSD.
PROLONGED EXPOSURE THERAPY FOR PTSDPE has three components:1) Psychoeducation about common reactions to trauma and the cause ofchronic post-trauma difficulties,2) Imaginal exposure (also called revisiting the trauma memory inimagination), repeated recounting of the traumatic memory, and3) In vivo exposure, gradually approaching trauma reminders (e.g., situations,objects) that are feared and avoided despite being safe.
TREATMENT FOR CO-OCCURRING PTSDIS EFFECTIVE #SCE chicagosummitconference.com
Community Connections/TREM website erior.html Seeking Safety website http://www.seekingsafety.org/ Prolonged Exposure information http://www.med.upenn.edu/ctsa/workshops pet.html E.M.D.R. websites http://www.emdr.com/ , http://www.emdria.org/ SAMHSA’s National Registry of Evidence-based Programs and Practices (NREPP) http://www.nrepp.samhsa.gov/
www.integratedrecovery.org On the RESOURCES page, there are several links under the headingSUPPORTING TRAUMA RECOVERY, including: Helping Yourself Heal: A Recovering Man's Guide to Coping with the Effectsof Childhood Abuse - (2006, 12 pages) Enhancing Substance Abuse Recovery Through Integrated TraumaTreatment - (2004; 13 pages) Helping Yourself Heal: A Recovering Women's Guide to Coping withChildhood Abuse Issues - (2003; 8 pages) Substance Abuse Treatment for Persons with Child Abuse and NeglectIssues - TIP 36 - (2000, on-line publication) Trauma-Informed Care in Behavioral Health Services – TIP 57
BIBLIOGRAPHICAL REFERENCES Beck, J.S. (2011). Cognitive Behavior Therapy: Basics and Beyond. New York: The GuilfordPress. Center for Substance Abuse Treatment. Substance Abuse Treatment for Persons WithChild Abuse and Neglect Issues. Treatment Improvement Protocol (TIP) Series Number36. DHHS Publication No. (SMA) 00-3357. Rockville, MD: Substance Abuse and MentalHealth Administration, 2000. Center for Substance Abuse Treatment. Substance Abuse Treatment for Persons With Cooccurring Disorders. Treatment Improvement Protocol (TIP) Series 42. DHHS PublicationNo. (SMA) 05-3992. Rockville, MD: Substance Abuse and Mental Health ServicesAdministration, 2005. Courtois, C.A., & Gold, S. The need for inclusion of psychological trauma in theprofessional curriculum: A call to action. Psychological Trauma, Theory, Research andPolicy. 2009,Vol. 1, No.1., 3-23.
BIBLIOGRAPHICAL REFERENCES Gradus JL, Qin P, Lincoln AK, et al. Posttraumatic stress disorder and completed suicide.Am J Epidemiol. 2010 Mar 15;171(6):721-7. Harris, M. and Fallot, R. (Eds.) (2001). Using Trauma Theory to Design Service Systems.New Directions for Mental Health Services. San Francisco: Jossey-Bass. Harris, M. and The Community Connections Trauma Work Group. (1998). TraumaRecovery and Empowerment: A Clinician’s Guide to Working with Women in Groups.New York: The Free Press. Mueser, K.T., Rosenberg, S.D., et al. A randomized controlled trial of cognitive-behavioraltreatment for posttraumatic stress disorder in severe mental illness. J of Consulting andClinical Psychology. 2008,Vol. 76, No.2., 259-271. Najavits, L. (2002). Seeking Safety: A Treatment Manual for PTSD and Substance Abuse.New York: The Guilford Press.
BIBLIOGRAPHICAL REFERENCES Shapiro, F. (2012). Getting past your past: Take control of your life with self-help techniquesfrom EMDR therapy. New York: Rodale. Shapiro, F. (2001). Eye Movement Desensitization and Reprocessing: Basic Principles,Protocols, and Procedures (2nd edition). New York: Guilford Press. Substance Abuse and Mental Health Services Administration. Trauma-Informed Care inBehavioral Health Services. Treatment Improvement Protocol (TIP) Series 57. HHSPublication No. (SMA) 14-4816. Rockville, MD: Substance Abuse and Mental HealthServices Administration, 2014. Van der Kolk, Bessel. (2014). The Body Keeps the Score: Brain, Mind, and Body in theHealing of Trauma. New York: Penguin Group.
Steve Wiland, LMSW, ICADCClinical Director, PNLHswiland@pnlh.org
PREVALENCE OF PTSD IN COD POPULATIONS In multiple national studies a high percentage of individuals presenting for addictions treatment were found to meet criteria for a co-occurring PTSD diagnosis (Najavits, 2002). Studies from the '90s found 12%- 59% co-prevalence; More recent studies found even higher co -prevalence rates.