Transcription
Improving Medication Safety: TheRole of the Medication Safety OfficerAlex Jenkins, PharmD, MSMedication Safety OfficerDepartment of PharmacyWakeMed Health & HospitalsRaleigh, NC
WakeMed Health & HospitalsThe Power to Heal. A Passion for Care.WakeMed Health & HospitalsRaleigh, North CarolinaNC Quality Center
Objectives Define medication safety and describe itsimportance to managing an effective patientsafety program Delineate the scope, positional goals, andpotential responsibilities for a medicationsafety officer Discuss opportunities, challenges, andstrategies for implementation of an effectivemedication safety programNC Quality Center
Key DefinitionsPatient Safety: freedom from accidental or preventableinjuries produced by medical careMedication Safety: freedom from accidental orpreventable injuries produced by medicationsAdverse Drug Event (ADE): an adverse event, or injuryresulting from medical care, involving medication usePreventable ADE: an ADE that involves some element oferror in medication useAvailable at: http://www.psnet.ahrq.gov/glossary.aspxNC Quality Center
Impact of Medications on Patient Safety 1999 Institute of Medicine Report– Up to 7,000 deaths result from ADEs every year– Have we improved since then? Impact of ADEs on patient care– As many as 10.4% of patients experience an ADE– Length of stay increased 8-12 days on average– Hospitalization costs increased by 16,000 to 24,000 Estimated 3.8 million inpatient admissions and 3.3 millionoutpatient visits have serious preventable medication errorsresulting in 21 billion in wasteful costs to healthcareTo Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000Preventing Medication Errors: A 21 Billion Opportunity. December 2010Arch Intern Med 2000;180(14): 2129-34JAMA 1996;274(1):29-34NC Quality Center
Accountability for Medication Use National Quality Forum (NQF) Safe Practice 18:“Pharmacy leaders should have an active role on theadministrative leadership team that reflects their authority andaccountability for medication management systems performanceacross the organization.” American Society of Health-System Pharmacists (ASHP)Council recommendations– Council on Pharmacy Practice– Council on Therapeutics Pharmacy Practice Model Initiative (PPMI)Safe practices for better healthcare-2010 update: a consensus report. Washington, DC: National Quality Forum; 2010AJHP 2011;68:1444-48NC Quality Center
Polling QuestionDoes your healthcare organization have aMedication Safety Officer or other medicationsafety leadership position?A. YesB. NoNC Quality Center
Importance of Quality and Safety Increasing number of standards and quality measuresrelying on medication use Increasing number of quality and safety measures tied toreimbursement––––Core MeasuresPay-for-PerformanceValue-Based PurchasingAccountable Care The PATIENTNC Quality Center
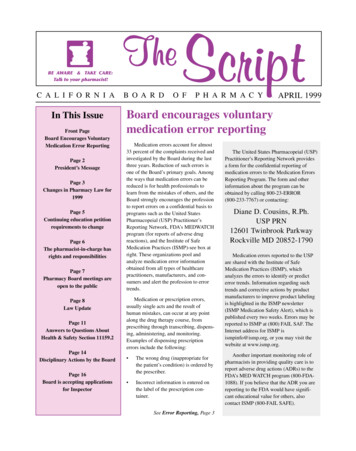
Adverse Drug Events and Medication ErrorsQual Safe Health Care 2004;13:306-314NC Quality Center
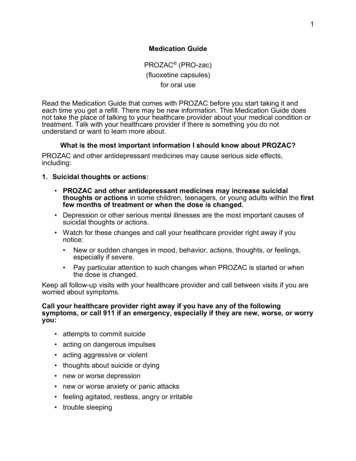
Swiss-Cheese ModelAvailable at: http://www.carefusion.com/pdf/Center for Safety/InvitedConferences/Using Tech to Address Med Errors Summary.pdfNC Quality Center
“An error doesn't become a mistake untilyou refuse to correct it.”- Orlando A. BattistaNC Quality Center
Business Case for Safety Making the business case for medication safety What is the cost to the healthcare system ofeach preventable ADE? Medication safety leader should be anauthoritative expert in safe medication use Key questions– What can larger organizations do?– What can smaller organizations do that canʼtjustify the creation of an MSO position?NC Quality Center
Safety Innovation: Unit-Dosing Innovative pharmacy practice spurred bymedication safety Ready-to-administer dosage forms Reduce medication errors throughstandardization Opportunity for safety improvements– Automated dispensing– 49% of errors observed in dispensing oradministration phases (Bates et al)Journal of General Internal Medicine 1995;10:199-205JAMA 1995;274:35-43NC Quality Center
Role and Scope Integration across the department andorganization Challenges of facilitating process improvementinitiatives related to safe medication use thataffect multiple disciplines“Pharmacists can play an important role as leaders to reducepatient safety risks, optimize the safe function of medicationmanagement systems, and align pharmacy services with nationalinitiatives that measure and reward quality performance.”Journal of Patient Safety 2010;6:31-37NC Quality Center
Regulatory Compliance Joint Commission Medication Management Chapter– MM.07.01.03 – Analyzing actual and potential ADEs– MM.08.01.01 – Evaluation of the medication management program Centers for Medicare and Medicaid (CMS)– Condition of Participation – Medication errors, adverse drug reactions,drug incompatibilities North Carolina Board of Pharmacy (NCBOP)Division of Health Service Regulation (DHSR)Drug Enforcement Administration (DEA)Environmental Protection Agency (EPA)North Carolina Department of Energy and Natural Resources(NCDENR)NC Quality Center
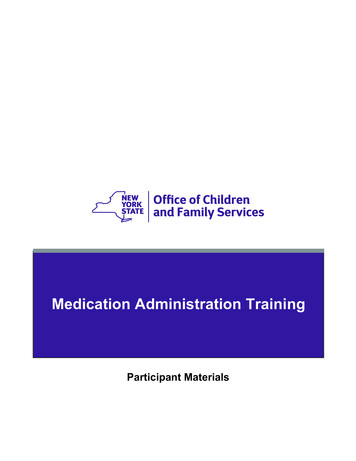
Medication-Use ProcessAvailable at: http://www.achca.org/content/pdf/LTCPLC Stmt3 MedUseProcess 081031.pdfNC Quality Center
Safe Medication ManagementPatient SpecificInformationSelection andProcurementStorage &HandlingMM.02.01.01MM.03.01.01Ordering &TranscribingMM.01.01.01Verifying,Preparing 5MM.05.01.09High Alert &Hazardous MedsMM.01.01.03Sound-Alike/LookAlike DrugsMM.01.02.01InvestigationalDrugsMM.06.01.05ADE ManagementMM.07.01.03NC Quality Medication Management EvaluationMM.08.01.01
Role and Scope Identifying and prioritizing medication safetyinitiatives Balance of visibility throughout theorganization and hospital administration withengaging front-line staff Liaison and contact person for medical staff,nursing, pharmacy, and ancillary servicesNC Quality Center
Key Leadership CharacteristicsA medication safety leader must be an effective leaderwithin the organization OrganizerFacilitatorStewardDynamicPatient safety liaisonConsultativeWriterNC Quality Center Excellent communicationGood presentation skillsEngagingNon-punitiveEncouraging (i.e. ofincident reporting)
Potential Responsibilities Patient/Medication safety roundsPrecepting residents/studentsPolicy development and reviewReviewing ADE dataIdentifying and leading performance improvement and qualityimprovement initiativesConducting medication safety tracers to assess medication managementcomplianceHosting surveyor/inspector visits from regulatory agenciesReviewing and providing recommendations for new technologiesMedication safety assessments and gap analysesAuditing for compliance with regulatory standardsDeveloping programs for hazardous drug managementNC Quality Center
Delivering Safety Information Storytelling and its impact Case presentations Multidisciplinary collaboration– Nurse shadowing Medication safety pearlsISMP Medication Safety Alert 2011;16(18):1-3NC Quality Center
Case Presentations Real experiences that emphasize key points Analysis of the case– Existing safety strategies– Potential reasons for system breakdowns Identified risks Attributable causes Contributing factors– Risk reduction strategies Tell a story that captures attentionNC Quality Center
Shadowing Experience Resident/Student shadowing nurses Learning experience Unbiased learner observing the medication-useprocess from the nursing perspective Reduces the Hawthorne Effect Discuss the experience and provide feedbackNC Quality Center
Data Analysis and Trending Clear definitions of medication error, adversedrug reaction, and adverse drug event Actual versus potential medication errors Quality Improvement (QI) metrics Maximize technology for reporting Minimize workarounds– Medication errors associated with informationtechnologyNC Quality Center
Implementing Technology Computerized Prescriber Order Entry (CPOE) Clinical decision support Automated storage devices– Automated dispensing cabinets (ADCs)– Carousel technology Barcode Medication Administration (BCMA) Electronic Medication Administration Record(eMAR) Automated compounding devicesNC Quality Center
Polling QuestionWhich of the following medication usetechnologies does your healthcare organizationhave?A. Barcode Medication Administration (BCMA)onlyB. Computerized Prescriber Order Entry(CPOE) onlyC. Both BCMA and CPOENC Quality Center
2007 Informatics SurveyNational survey of medication-use technologies(25.6% response rate)Hospital CategoryAll U.S. HospitalsBCMA (%)24.1 50 staffed beds14.750-99 staffed beds24.3100-199 staffed beds30.2200-299 staffed beds36.5300-399 staffed beds40.2400-799 staffed beds25.6 800 staffed beds6.3Veterans Affairs Hospitals100AJHP 2008;65:2244-2264AJHP 2006;63:327-345NC Quality Center9.4% in20051.5% in2002Of thehospitalswithout BCMA,56.5% plannedto implement asystem within 3years
Technology Barriers: BCMA Implementation of a BCMA system can preventmany errors but may also contribute to some ADEs Failure points in the BCMA process––––Medication mislabelingMedication missing bar-codeInability to scan bar-codeSystem not available Potential system workarounds– Facilitated by workflow design Any other processes that may contribute to errorscaused by BCMAJournal of the American Informatics Association 2008;15(4):408-423NC Quality Center
Technology Workarounds: BCMAWorkaroundUser scans med without visual checkPotential ErrorWrong med, dose & routeUser bypasses med “double check”User does not verify new med ordersUser scans bar-code after label removedUser administers med without parametersWrong med, dose, route & timeUser administers med without scanning bar-codeUser administers med without scanning patient IDWrong patientPatient ID placed somewhere besides the patientUser scans & transports meds for 1 patientUser separates scanner from cartUser scans 1 med multiple times for full doseJourn of the Amer Inform Assoc 2008;15(4):408-423NC Quality CenterWrong med & dose
Implementing New Technology Conduct a Failure Mode and Effects Analysis(FMEA) whenever possible Utilize champions in the nursing staff Define expectations and a standardized processthrough written policies and procedures Hold staff accountable Utilize available continuous quality improvement(CQI) reporting capabilities Technology is an additional safety measure NOT areplacement for critical thinkingNC Quality Center
Polling QuestionDoes your healthcare organization use availablecontinuous quality improvement (CQI) reportingfunctions to monitor use and optimize informationtechnology applications?A. ExtensivelyB. SomewhatC. RarelyD. NeverE. Reporting functions are not availableNC Quality Center
Literature Review and Evaluation ISMP Medication Safety AlertsNurse Advise-ERRJoint Commission Sentinel Event AlertsMedication safety assessmentsGap analysesNC Quality Center
Success Stories Share your successes within and outside yourhealthcare organization WakeMed recent examples of safetyimprovement– Acetadote dosing standardization– Concentrated oral morphine Quality improvement changes across the health systemin ordering, preparing, dispensing and administration– PCA protocol changes to reduce the risks of dosingerrorsNC Quality Center
Using Medication Safety to ImplementQuality Improvement InitiativesCollect data Retrospective vementsNC Quality CenterIdentify risksand hazardsDevelop actionplan(s)
Medication Safety: A Shared Responsibility Safety is a broader goal that should be shared The patient does not benefit if lessons learnedare not shared Systems breakdowns are generally not uniqueto one system just like individual errors areoften not isolated to one individual Share stories of system breakdowns andprocess improvements that were implementedNC Quality Center
Conclusion Healthcare organizations should have a position withresponsibilities dedicated to improving medicationsafety Role and scope of a medication safety leader mayinclude a variety of responsibilities that provideoversight over the medication management system Medication safety leaders should coordinate medicationrelated systems improvement initiatives to improvepatient safetyNC Quality Center
To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000 Preventing Medication Errors: A 21 Billion Opportunity. December 2010 Arch Intern Med 2000;180(14): 2129-34 JAMA 1996;274(1):29-34 . NC Quality Center Accountability for Medication Use