Transcription
Learning fromreported medicationincidents inNorthern IrelandSummary ReportJanuary to December 2018
Intentionally blank for printing purposes
IndexPageIntroduction4Data at a glance6Northern Ireland Data7Secondary Care Data11Thematic analysis17Omission / delay of ds and analgesics40Antipsychotics and Lithium44Oxygen47Primary Care Data50Medication Safety Messaging and Alerting553
IntroductionReporting all medication incidents whether they resulted in harm or not, is essential to improvingpatient safety. It permits us to learn and improve when things go wrong and take action to preventsimilar events from re-occurring. This is the second annual medication incident report of this typeto be produced in Northern Ireland. Prior to this reports were generated on a three monthly basisbut it was felt that aggregated data over a one year period would provide richer analysis forthemed learning.New sections in this report include:Review of oxygen, opioids, antipsychotic and lithium reported incidents.Purpose of the reportThe purpose of this report is to inform the NI Health and Social Care (HSC) community of thefollowing:The main types of medication incidents reported.The factors identified in the reports which led to the incident occurring.Good practice that is occurring within local organisations which are supporting patientsafety in the themes discussed.This report assists to inform the work led by the Department of Health in its response to the WorldHealth Organization’s (WHO) third Global Patient Safety Challenge: Medication Without Harm. Thischallenge aims ‘to reduce severe avoidable medication-related harm by 50%, globally in the nextfive years’.The requirements of the WHO challenge are for countries to:1.Target improvements in three priority areas:Transitions of carePolypharmacyHigh Risk Situations2.Design specific programmes of action for improving safety in each of four domains inwhich medications can cause avoidable harm: patients and the public, health careprofessional’s behaviour, systems and practices of medication and the medicinesthemselves.Further information about the WHO ‘Medication Without Harm’ challenge can be found at y/en/.As incident reporting is a voluntary process it is not a reliable source to be used to trackimprovement over time. However it does help to identify and target areas for improvement andthe reports themselves provide invaluable insights into current situations and practice that impacton medication safety.4
Who should read this report?This report should be shared with everyone who has a responsibility for medication safety withintheir organisation, including all health care professionals who prescribe, dispense, administer ormonitor medication and also managers who have a responsibility for patient safety within theirorganisations or remit. The contents of the report can also be used to support medication safetytraining and should be shared with relevant undergraduate and postgraduate training providers.Data analysis scope and structureThis review is informed by medication incidents reported by the five Health and Social Care Trustsand the Health and Social Care Board (HSCB) from 1st January -31st December 2018. The HSCBdata refers to medication incidents reported by community pharmacies. As there is nocurrent regional adverse incident reporting system, it was not possible to include incidentsreported by general practitioners or dentists and this review also does not include incidentsreported to RQIA from nursing / residential care homes.The aim of this report is to learn from preventable medication related harm and thereforeincidents related to adverse drug reactions, security and storage of controlled drugs and defectivemedicines are not included in the analysis.The data which informs this report has been gathered and analysed by the secondary careNorthern Ireland Medicines Governance team and the HSCB Pharmacy Co-Ordinator for primarycare*. Quantitative and themed analyses of the datasets have been undertaken and the findingsare summarised and discussed within two distinct sections for secondary and primary care.As readers may prefer to avail of a quick summary of the quantitative data, a ‘Data at a Glance’page is included on page 6.Linked to the findings from the themed analyses is information on current improvement initiativesor projects that are being undertaken by HSC organisations to help mitigate against the types ofcommon and problematic errors identified.A summary of medication safety messaging / alerts that was issued during this time period is alsoincluded.Our thank youThe publication of this report would not be possible if we did not havepeople taking the time to report medication incidents. This is a thankyou to all staff for sharing your learning. We hope that you find thereport useful and informative, and that it encourages all staff tocontinue to report medication incidents so that together we canimprove medication safety for our patients.This report has been authored by the Northern Ireland MedicinesGovernance Team and has been endorsed by the HSCB RegionalMedicines Safety Group and the Safety Quality Experience (SQE) group.*Further information about these roles can be found at http://www.medicinesgovernanceteam.hscni.net/5
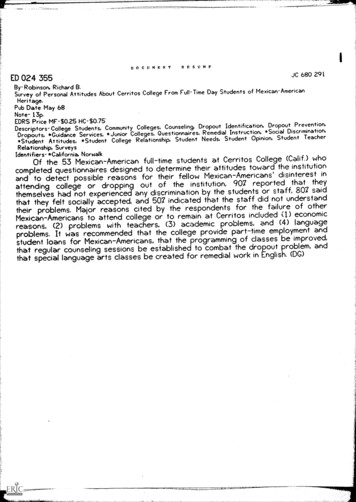
Data at a glanceTrends in incident reporting7054Medication Incidents ReportedThis is an increase on the previous year—6148 in 2017**21Serious Adverse Incidents (SAIs)reported involving medication(15 Secondary care and 6 Primary care*)(*data from Community Pharmacy only)* Community Pharmacy incidents have been included since quarter period October – December 2013.Number of incidents reported by organisationPercentage of incidents by stage of themedicines management processActual impact versus Potential impact of incidentsPercentage of Harm/ No Harm by organisationThe NI average is 77.7% of incidents are reported as causing ‘no harm’HSCB data refers to community pharmacist reported incidents common inistrationPrescribingOmitted / delayed medicineor doseDose or strength was wrongor unclearDose or strength was wrongor unclearWrong / unclear drug/medicineOmitted / delayed medicineor dose15515464303553536Most common therapeutic group / medicinesreported in incidents causing actual harm(moderate and above) and potentially major /catastrophic hoticOxygen1364532151312
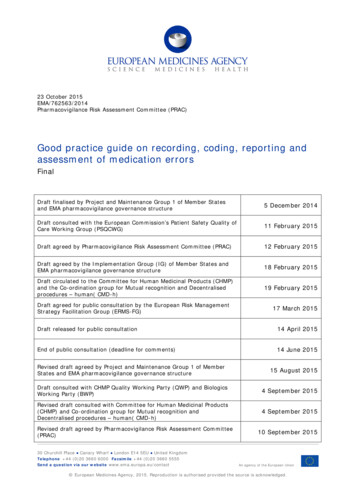
Northern Ireland DataFigure 1 shows the number of medication incidents reported by organisationsfrom 2002. Community pharmacy incidents have been included since quarterperiod October – December 2013.There were 7054 incidents submitted in 2018, which is a increase of 907 from the previous year.211,278 medication incidents were reported in England for a similar time period October 2017 toSeptember 2018 (Obtained from NaPSIR quarterly data, accessed at ent-safety-incident-reports-27-march-2019/. The reporting rate per head ofcapita for both Northern Ireland and England, for this time period is 0.004%. This is also without thefull complement of Northern Ireland data from integrated care and care home facilities .The National Reporting and Learning System (NRLS) in England also includes incidents related toadverse drug reactions and the safe storage and custody of medicines. Verbal communication fromthe Medication Safety Lead at NHS Improvement England, confirms that the numbers are small,equating to 1.5% of the total number of medication incidents reported.Figure 1Trends in incident reporting**Community Pharmacy incidents have been included since quarter period October – December 2013. Learning from reported medication incidents in Northern Ireland Summary Report January to December 2017 reported the reporting rate per head ofcapita for Northern Ireland and England in 2017 as 0.032 and 0.030 respectively. The figures should have been 0.0032 and 0.0030.7
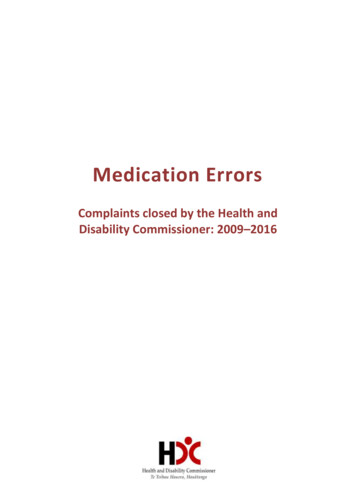
The number of medication incidents reported by organisations in 2018 is shown in Figure 2.Figure 2Number of incidents reported by organisationNumber of incidents reported by 629WHSCTHSCB5000BHSCTNHSCTSEHSCTSHSCTFigure 3 shows an incident reporting rate per 1000 bed for each trust. This is calculated as:the total number of medication incidents reported in 2018X 1000the total number of occupied bed days **The Hospital Information Branch at the Department of Health provided this data, which includesthe following clinical areas:Acute services, Maternity and Child Health, Elderly Care, Mental Health and Learning DisabilityFigure 3Medication incident reporting rate per 1000bed days per Trust8
The medication incident rate is based on medication incidents that have been reported and istherefore subject to reporting bias. Research has also shown that ‘higher reporting rates correlatewith a better safety culture and risk management ratings. Regular reporting of incidents fromorganisations is therefore something to be encouraged’ (NPSA, Safety in Doses, 2009).The degree of harm to patients, both actual and potential harm, as a result of a medication incidentis coded in Northern Ireland using the HSC Regional Impact Table (June 2016). Patient harm isdefined under 5 categories as noted below.Harm level DefinitionInsignificant Near miss, no injury or harm.Minor Short-term injury / minor harm requiring first aid / medical treatment. Any patients safety incident that required extra observation or minortreatment e.g. first aid. Non-permanent harm lasting less than one month. Admission to hospital for observation or extended stay (1-4 days duration). Emotional distress (recovery expected within days or weeks). Semi-permanent harm/ disability (physical, emotional injuries / trauma)(Recovery expected within one year). Admission / readmission to hospital or extended length of hospital stay / careprovision (5-14 days). Any patient safety incidents that resulted in a moderate increase in treatmente.g. surgery required. Long- term permanent harm / disability (physical / emotional injuries / trauma). Increase in length of hospital stay / care provision by 14 days. Permanent harm / disability (physical / emotional trauma) to more than oneperson. Incident leading to death.ModerateMajorCatastrophic9
An average of 77.7% of incidents reported resulted in ‘no harm’ to the patient. ImplementingHuman Factors in Healthcare (Patient Safety First, 2010) recommends that a minimum of 70%of reported incidents should involve ‘no harm’ to the patient as an indicator of a positivereporting culture where staff are aware of the importance of reporting ‘no harm’ incidents. Itshould be noted that the descriptor of ‘minor’ harm includes ‘extra observation’ as well asminor treatment, for example where no actual harm has occurred however additional stepsare taken to ensure the safety of a patient following the incident. Figure 4 shows percentage of‘no harm’ and ‘harm’ reporting by organisation.Figure 4Percentage of Harm / No Harm by organisation10
Secondary Care DataFigure 5 shows the actual impact of the incidents reported within secondary care versus theirpotential impact. However when reviewing this chart it should be taken into account that assigningpotential harm is often subjective and not as easy to define as the actual impact. The incidentreporter, reviewer or approving manager may consider the impact of harm in terms of the barriersthat already exist to prevent that incident from re-occurring. Therefore variability within andbetween organisations will exist. Despite this, it is well recognised that learning from potentiallyserious harm incidents is essential and demonstrates a healthy safety culture.Figure 5Actual impact versus Potential impact of incidentsThere were 15 Serious Adverse Incidents (SAI) reported in 2018 in line with the Regional SAIdefinition. Details of these incidents are noted below. Four of these incidents were deemed to be‘Never Events’.* NHS Improvement defines Never Events as ‘Serious Incidents that are whollypreventable because guidance or safety recommendations that provide strong systemic protectivebarriers are available at a national level and should have been implemented by all healthcareproviders. Strong systemic protective barriers are defined as barriers that must be successful, reliableand comprehensive safeguards or remedies.’’Patient had recent treatment for gastric cancer and presented with a 2 to 3 day history ofblood stained sputum, bruising, intermittent nose bleeds and left sided chest pain and a hadrecently fallen. From history and examination pulmonary embolism (PE) was considered themost likely diagnosis. CT PA was requested but was not immediately available andenoxaparin 80mg was prescribed and administered. Ninety minutes after this dose, bloodresults were reported with low platelets at 42 x109/l and low fibrinogen at 0.9mg/l. Aplatelet transfusion was administered but over the next 12 hours the patient complained ofa worsening headache and CT Brain demonstrated bilateral subdural haematomas andcerebral oedema. CT PA was negative. Further investigations revealed metastaticmalignancy; the bleeding tendency and cerebral oedema were secondary to this. Patient‘scondition deteriorated and subsequently t/files/publications/health/HSC-SQSD-36-18.pdf11
‘Patient suffered cardiac arrest on ward and passed away. Discussed with coroner and felt thatmost likely diagnosis was acute PE causing cardiac arrest as post mortem indicated patient hadmultiple PEs and right leg DVT. Patient had not been prescribed enoxaparin during a period priorto their death.’‘Patient had a lower limb cast put in place following an ankle fracture and wer
Reporting all medication incidents whether they resulted in harm or not, is essential to improving patient safety. It permits us to learn and improve when things go wrong and take action to prevent similar events from re-occurring. This is the second annual medication incident report of this type to be produced in Northern Ireland. Prior to this reports were generated on a three monthly basis