Transcription
UnderstandingUnderstandingNon-Hodgkin LymphomaThis patient guide is supported throughunrestricted educational grants from:Non-HodgkinLymphomaA Guide for Patients,Survivors, andLoved Ones8th EditionContact the Lymphoma Research FoundationHelpline: (800) 500-9976helpline@lymphoma.orgWebsite: lymphoma.orgFall 2020
Lymphoma Research Foundation(LRF) Helpline and Clinical TrialsInformation ServiceCONTACT THELRF HELPLINETrained staff are available to answer questionsand provide support to patients, caregivers andhealthcare professionals in any language.Our support services include: Information on lymphoma, treatment options,side effect management and current researchfindingsFOCUS ON LYMPHOMAMOBILE APPThe Lymphoma Research Foundation’smobile app, Focus on Lymphoma, is agreat tool and resource for lymphomapatients to manage their disease.Focus on Lymphoma is the first mobileapp that provides patients andcaregivers comprehensive content Financial assistance for eligible patients andreferrals for additional financial, legal andinsurance helpbased on their lymphoma subtype and tools to help manage their diagnosis, Clinical trial searches based on patient’sdiagnosis and treatment historyThe Focus on Lymphoma mobile app was recently named Best App by PR News and Support through LRF’s Lymphoma SupportNetwork, a national one-to one volunteerpatient peer programMonday through Friday9:30 am 7:30 pm Eastern Standard Time (EST)Toll-Free (800) 500-9976or email helpline@lymphoma.orgincluding a medication manager, doctor sessions tool and side effects tracker.is available for free download for iOS and Android devices in the Apple App Storeand Google Play.For further information on LRF’s award winning mobile app or any of ourprograms and services, call the LRF Helpline toll free (800) 500-9976,email helpline@lymphoma.org or visit us at lymphoma.org.
UnderstandingNon-Hodgkin LymphomaA Guide For Patients, Survivors, and Loved OnesFall 20208th EditionThis guide is an educational resource compiled by the LymphomaResearch Foundation (LRF) to provide general information on adultnon-Hodgkin lymphoma. This booklet is not intended to replaceindividualized medical care or the advice of a patient’s doctor.Patients are strongly encouraged to talk to their doctors for completeinformation on how their disease should be diagnosed, treated, andfollowed. Before starting treatment, patients should discuss thepotential benefits and side effects of cancer therapies with theirphysician.Contact the Lymphoma Research FoundationHelpline:(800) his patient guide is supported through unrestricted educational grants from: 2020 Lymphoma Research Foundation.Information contained herein is the property of the Lymphoma Research Foundation (LRF). Anyportion may be reprinted or reproduced provided that LRF is acknowledged to be the source and theFoundation’s website (lymphoma.org) is included in the citation.
ACKNOWLEDGMENTSThe Lymphoma Research Foundation wishes to acknowledge thoseindividuals listed below who have given generously of their time andexpertise. We thank them for their contributions, editorial input, andprofessional knowledge, which have truly enhanced this publication.The review committee guided the content and development of thispublication. Without their dedication and efforts, this publication wouldnot have been possible. We hope those in the lymphoma and chroniclymphocytic leukemia community will now be better informed and havea better understanding of these diagnoses because of the graciousefforts of those involved in the planning and execution of thiscomprehensive disease guide.Review CommitteeEditorial Board Steering CommitteeEditorial Chairman*Morton Coleman, MD, FACP, NewYork-Presbyterian Hospital/Weill Cornell MedicineMedical Review BoardJeremy S. Abramson, MD, FACP, Massachusetts GeneralHospital/Harvard MedicineNancy L. Bartlett, MD, Washington University School of Medicine*Bruce D. Cheson, MD, FACP, FAAAS, FASCO, LombardiComprehensive Cancer Center/Georgetown University Hospital*Kieron M. Dunleavy, MD, GW Cancer Center/GeorgeWashington UniversityDavid R. Freyer, DO, MS, Children’s Hospital Los Angeles andUSC Norris Comprehensive Cancer Center*Leo I. Gordon, MD, FACP, Robert H. Lurie ComprehensiveCancer Center of Northwestern UniversityiiUnderstanding Non-Hodgkin Lymphoma
*Thomas M. Habermann, MD, Mayo Clinic, Rochester, MN*Brad S. Kahl, MD, Washington University Medical School*Ann S. LaCasce, MD, MMSc, Dana-Farber Cancer Institute/Harvard Medicine*John P. Leonard, MD, New York-Presbyterian Hospital/WeillCornell Medicine*Peter Martin, MD, New York-Presbyterian Hospital/Weill CornellMedicineJohn M. Pagel, MD, PhD, Center for Blood Disorders andTransplantation/Swedish Cancer InstituteLauren C. Pinter-Brown, MD, FACP, Chao FamilyComprehensive Cancer Center/University of California at IrvinePierluigi Porcu, MD, Sidney Kimmel Cancer Center/JeffersonHealthLymphoma Research Foundation ReviewersVictor Gonzalez, Associate Director of Support Resources andStrategic PartnershipsMeghan Guiterrez, Chief Executive OfficerSarah Quinlan, Senior Director of Program and StrategyIzumi Nakano, Associate Director of Support ServicesUchenna Esomonu, Support Services Coordinator*Member of LRF Scientific Advisory Board (SAB), comprised of 45 world-renowned lymphoma experts, seeksout the most innovative and promising research projects for support.Understanding Non-Hodgkin Lymphomaiii
TA B L E O F C O N T E N T SAbbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Part 1 — Learning the Basics. . . . . . . . . . . . . . . . . . . . . . . . . 8Chapter 1: Understanding the Disease. . . . . . . . . . . . . . . . . . . . 8Table 1.1. Main Types of Indolent and Aggressive NHLs(Listed Alphabetically). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Chapter 2: Seeking Medical Attention. . . . . . . . . . . . . . . . . . . . 30Table 2.1. Signs and Symptoms Commonly Found inPatients With NHL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Chapter 3: Receiving a Diagnosis. . . . . . . . . . . . . . . . . . . . . . . 35Table 3.1. The Three Main Types of Biopsies. . . . . . . . . . . . . 37Table 3.2. Immunohistochemistry andFlow Cytometry Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Chapter 4: Work-Up Before Treatment Can Begin. . . . . . . . . . 45Table 4.1. The Eastern Cooperative Oncology Group (ECOG)Performance Status Scale. . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Table 4.2. Types of Imaging Tests. . . . . . . . . . . . . . . . . . . . . . 48Table 4.3. Other Types of Biopsies. . . . . . . . . . . . . . . . . . . . . 501Understanding Non-Hodgkin Lymphoma
Part 2 — Treatment of Non-Hodgkin Lymphoma. . . . . 55Chapter 5: What to Know Before Starting Treatment . . . . . . . 55Table 5.1. International Prognostic Index for Diffuse LargeB-Cell Lymphoma and NHL. . . . . . . . . . . . . . . . . . . . . . . . . . . 58Chapter 6: Treatments for Non-Hodgkin Lymphoma. . . . . . . . 69Table 6.1. Common Chemotherapy Regimens for NHL . . . . 73Table 6.2. Catheters Used to AdministerDrug Treatments. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97Table 6.3. Methods for Delivering Radiation Therapy . . . . 100Table 6.4. Terms Used to Describe Treatmentand Its Outcomes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106Table 6.5. Forms of Complementary Therapy. . . . . . . . . . . 110Part 3 — Survivorship and Living With theSide Effects of Treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . 112Chapter 7: Common Treatment Side Effects . . . . . . . . . . . . . 112Table 7.1. Five Common Conditions Caused byDecreased Blood Cell Production . . . . . . . . . . . . . . . . . . . . 115Chapter 8: Managing Life During and After Treatment. . . . . 142Table 8.1. Coping Strategies. . . . . . . . . . . . . . . . . . . . . . . . . 142Understanding Non-Hodgkin Lymphoma2
Part 4 — Hospital Admission. . . . . . . . . . . . . . . . . . . . . . . 148Chapter 9: Preparing to Go to the Hospital. . . . . . . . . . . . . . . 148Part 5 — Clinical Trials and Advancesin Treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155Chapter 10: Overview of Clinical Trials. . . . . . . . . . . . . . . . . . 155Table 10.1. The Four Phases of Clinical Trials. . . . . . . . . . . 156Chapter 11: Advances in Treatment of Patients WithNon-Hodgkin Lymphoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161About The Lymphoma Research Foundation . . . . . . . . . . . . . . 1663Understanding Non-Hodgkin Lymphoma
A B B R E V I AT I O N S3D-CRT three-dimensionalconformal radiationtherapyABMS American Board ofMedical SpecialtiesAIDS acquiredimmunodeficiencysyndromeAIHA autoimmune hemolyticanemiaAITLangioimmunoblasticT-cell lymphomaALCL anaplastic large celllymphomaALKanaplastic lymphomakinaseALLacute lymphoblasticleukemiaANCabsolute neutrophil countASCO American Society ofClinical OncologyASHAmerican Society ofHematologyβ2Mbeta-2 microglobulinBTKBruton tyrosine kinaseCARchimeric antigen receptorCGVHD chronic graft-vs-hostdiseaseCBCcomplete blood countCLLchronic lymphocyticleukemiaCNScentral nervous systemCPRcardiopulmonaryresuscitationCRcomplete al fluidcomputed tomographycutaneous T-celllymphomadouble-hit lymphomadiffuse large B-celllymphomadeoxyribonucleic acid;genetic materialenteropathy-associatedT-cell lymphomaEpstein-Barr virusechocardiogramextranodal marginal zonelymphomaFellow of the AmericanCollege of PhysiciansU.S. Food and DrugAdministrationfluorescence in situhybridizationfollicular lymphomaFollicular LymphomaInternational PrognosticIndexfine needle aspirationgerminal center B-cell–likegraft-versus-host diseasegraft-versus-lymphomahepatitis B virushepatitis C virushistone deacetylasehumanimmunodeficiency virusAbbreviations4
HGBCL high-grade B-celllymphoma with MYC andBCL2 and/or BCL6 generearrangementsHLHodgkin lymphomaHTLV-1 human T-celllymphotropic virus type 1IgMimmunoglobulin MIGRT image-guided odulatory drugIPIInternational PrognosticIndexIRBinstitutional review ate dehydrogenaseLRFLymphoma ResearchFoundationMALT mucosa-associatedlymphoid tissueMIPIMantle Cell LymphomaInternational PrognosticIndexMCLmantle cell lymphomaMMAE monomethyl auristatin EMRminor responseMRD minimal residual diseaseMRImagnetic resonanceimagingMUGA multigated acquisitionscanMZLmarginal zone lymphomaNCCN National ComprehensiveCancer NetworkNCINational Cancer InstituteNHLnon-Hodgkin lymphomaNIHNational Institutes ofHealthNKnatural killer (cell)NSAID nonsteroidal antiinflammatory drugNTBR not-to-be-resuscitatedPCRpolymerase chainreactionPETpositron emissiontomographyPFTpulmonary function testPI3Kphosphoinositide (orphosphatidylinositol)-3kinasePICC peripherally insertedcentral catheterPMBCL primary mediastinalB-cell lymphomaPMLprogressive multifocalleukoencephalopathyPNPeripheral neuropathyPRpartial remissionPSperformance statusPTCL peripheral T-celllymphomaPTCL- peripheral T-cellNOSlymphoma, not otherwisespecifiedRNAribonucleic acid; geneticmaterialSAB5Understanding Non-Hodgkin Lymphomascientific advisory board
SEERSLLSMZLSYKTLSTNFTSEBTWHOWMSurveillance, Epidemiology, and End Resultssmall lymphocytic lymphomasplenic marginal zone lymphomaspleen tyrosine kinasetumor lysis syndrometumor necrosis factortotal skin electron beam therapyWorld Health OrganizationWaldenström macroglobulinemiaAbbreviations6
INTRODUCTIONThe purpose of this guide is to educate and support patients withnon-Hodgkin lymphoma and their caregivers. It is designed to allowthem to familiarize themselves with this disease and to become activeparticipants in their healthcare decisions. Chapters in this guideaddress different issues faced by patients with non-Hodgkinlymphoma, including what to expect during diagnosis, work-up, andtreatment; how to cope with treatment side effects; and what questionsto ask doctors, nurses, physician assistants, social workers, and othermembers of the healthcare team.In addition to this guide, information is available on the LymphomaResearch Foundation’s (LRF’s) website at lymphoma.org. The LRFHelpline can also provide additional information and copies of LRFeducational and support publications. For Helpline assistance, call(800) 500-9976 or email helpline@lymphoma.org.7Understanding Non-Hodgkin Lymphoma
Part 1 — Learning the BasicsChapter 1: Understanding the DiseasePart 1Non-Hodgkin lymphoma (NHL) is a type of blood cancer that affectsspecialized white blood cells called lymphocytes. Lymphocytes worktogether with other cells in the immune system to defend the bodyagainst invasion by bacteria, viruses, parasites, and other foreignsubstances. Lymphocytes travel in the bloodstream and in anothernetwork of mostly small vessels called the lymphatic system.Lymphocytes are found in tissues and many of the organs of the bodybut are concentrated in the bone marrow, in the spleen, and inspecialized structures called lymph nodes. Lymph nodes, which arepart of the lymphatic system, are where the body develops an immuneresponse to viruses and bacterial infections.This chapter explains these and other terms that will help peopleunderstand NHL and how it affects a person’s health. A betterunderstanding of the disease may allow patients to be activeparticipants in their care.What Is Cancer?The body is made up of many different types of specialized cells thatare organized into tissues and organs that perform the tasks neededto sustain life. To keep the body running smoothly, cells in the bodygrow, work, and multiply in a highly regulated way.All normal cells have a limited lifespan, which means they areprogrammed to die when they have served their purpose. A selfdestruct mechanism is triggered when cells become senescent (tooold) or get damaged; this process is called apoptosis or programmedcell death. However, sometimes damage to the genes inside a cell(gene mutations) leads to the loss of normal regulation and allows theLearning the Basics8
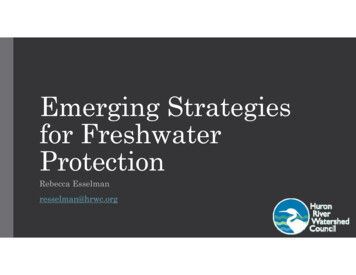
cell to live and multiply indefinitely. Unless the body’s immune systemremoves these abnormal cells, they can become cancerous.Cancer, or malignancy, is a disease in which abnormal cells gain theability to multiply uncontrollably. When these cells accumulate, theyform a mass called a tumor that can interfere with normal organfunction.HOW CANCER FORMS INSIDE THE BODYNormal cell divisionCancer cell divisionDamaged or senescent cellDamaged cell does not self-destruct,and starts to multiply9Understanding Non-Hodgkin LymphomaProgrammed cell death (apoptosis)Groups of abnormal cellsmay form tumors
What Are the Different Types of Blood Cells?There are three main classes of blood cells: Red blood cells (or erythrocytes) — Red blood cells carry oxygenfrom the lungs to all tissues in the body. Red blood cells also removethe carbon dioxide waste produced by cells and bring it to the lungsto be exhaled. A low number of red blood cells is called anemia. Aperson with anemia may feel tired, weak, and/or short of breath.White blood cells (or leukocytes) — White blood cells work aspart of the immune system to help the body fight infections. A lownumber of leukocytes is called leukopenia. The main types of whiteblood cells are:– Lymphocytes — These are discussed on the following page.– Granulocytes — There are three types of granulocytes:neutrophils, basophils, and eosinophils. Neutrophils help fightbacterial infections. A low number of neutrophils in the blood iscalled neutropenia. People with neutropenia are more likely to getinfections (mostly bacterial infections) than people with normalnumbers of neutrophils. Basophils are cells that take part ininflammatory reactions. Eosinophils also help fight infections —particularly those caused by parasites — and they can becomeplentiful during allergic reactions.– Monocytes — These also play an important role in immunityand are usually the first cells to recover after an episode ofneutropenia. Monocytes can give rise to macrophages which helpthe immune system to fight infections. Platelets (or thrombocytes) — Platelets are tiny cells that clumpLearning the Basics10Part 1Most cancers are named after the organ or cell type of their origin. Acancer of the lymphocytes is called a lymphoma or lymphocyticleukemia, depending on whether the cancerous lymphocytes originateprimarily in the lymph nodes and other lymphatic tissues (lymphoma)or primarily in the bone marrow (Waldenström macroglobulinemia) andthe blood (lymphocytic leukemia). Although named for their origin,lymphocytic cancers may be found in other compartments of the body.
together in a blood clot to stop bleeding from broken blood vessels.A low number of platelets is called thrombocytopenia. People withthrombocytopenia are more likely to bruise and bleed with minortrauma. They are also more likely to have severe and recurringnosebleeds and bleeding gums.Because blood cells have a limited lifespan, the body needs to constantlyreplenish its supply of these cells. Red blood cells live for about 120days; most white blood cells have a much shorter life, ranging from a fewhours to a few weeks. New blood cells are made by hematopoietic(blood-forming) stem cells, which are immature (non-specialized) cellsthat can develop into any kind of blood cell. Hematopoietic stem cells arefound mainly in the bone marrow (the spongy, material inside large bonessuch as the pelvis, and vertebrae).What are Lymphocytes?Lymphocytes are one type of white blood cell. There are three maintypes of lymphocytes: 11B lymphocytes (B cells) — B cells make antibodies to fightinfections.T lymphocytes (T cells) — T cells are the “quarterbacks” of theimmune system and help direct immune responses. There are manytypes of T cells. Some T cells help B cells make antibodies, someattack and kill infected cells, some make chemicals called cytokinesthat help the body get rid of viruses and cancer cells, others helpcontrol or regulate the way other parts of the immune systemfunctions.Natural killer (NK) cells — NK cells attack and kill cancer cells andvirus-infected cells. They also make cytokines.Understanding Non-Hodgkin Lymphoma
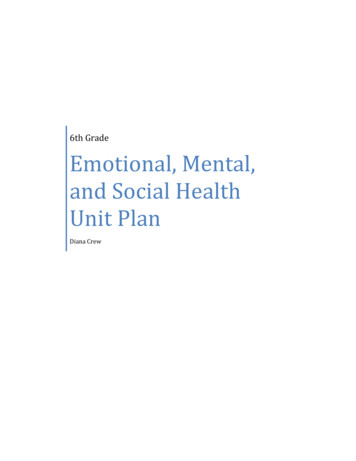
What Is the Lymphatic System?THE LYMPHATIC SYSTEMTonsilThymusLymphnodesArteryVeinLymph nodeDiaphragmSpleenLymphvesselsLearning the Basics12Part 1As shown in the image below, the lymphatic system is a circulatorysystem made up of a spidery network of thin tubes called lymphvessels or lymphatic vessels. Like blood vessels, lymphatic vesselsbranch out into all tissues of the body. Lymphatic vessels carry lymph,a liquid that contains lymphocytes to help fight infection.
Within this huge network of vessels are groups of small, bean-shapedorgans called lymph nodes, which are also commonly known asglands. Lymph nodes filter the lymph fluid, removing bacteria, viruses,and other foreign substances from the body. Hundreds of lymph nodesare found at locations throughout the body, including the neck,underarms, chest, abdomen, and groin. Lymphocytes can mostly befound in lymph nodes, where they monitor the body’s immune systemfor signs of infection. The lymph nodes can change in size, becomingbigger or smaller depending on the number of lymphocytes insidethem. Lymph nodes are often tender when they react to an infection,but they may not be tender when they enlarge due to lymphoma.How Does the Immune System Work?The immune system is the body’s defense against things that mightcause it harm. The immune system has multiple components and ismade up of a network of cells, tissues, and organs that work togetherto detect and destroy invaders—such as bacteria, viruses, andparasites—that can make people sick. The skin, mucous membranes,stomach acid, and the cough reflex provide a barrier to invaders. Thethymus gland, spleen, tonsils, bone marrow, circulatory system, andlymphatic system provide adaptive (meaning adapting to externalforces or threats) immunity. B cells and T cells, the two main types oflymphocytes, carry out the adaptive immune response by recognizingand either deactivating or killing specific invading organisms. Theadaptive immune system can then “remember” the identity of theinvader, so that the next time the body is infected by the same invader,the immune response will develop more quickly and strongly.13Understanding Non-Hodgkin Lymphoma
What Is Lymphoma?What Is Non-Hodgkin Lymphoma?In the United States, NHL (including chronic lymphocytic leukemia andsmall lymphocytic lymphoma) is the fifth most common type of canceraffecting adults. NHL is not a single disease but rather a large groupof closely related cancers that come from abnormal lymphocytes.The World Health Organization (WHO) classifies more than 80types of NHL, and ongoing research continues to identify new types.While these various types share many common features, certaincharacteristics set them apart from each other, including: How do cells appear when viewed under a microscope Genetic and other molecular characteristics How and where they grow in the body How their growth and spread affects patients How the disease should be treated Likely outcome of treatment (curable vs not curable, but treatable)NHL is divided into the following two major groups (as well as somesubgroups that are not discussed here): B-cell lymphomas — These lymphomas develop from abnormalB lymphocytes and are the most common, comprising about 90percent of NHL in the United States.Learning the Basics14Part 1A lymphoma is a type of cancer that originates from lymphocytes.Lymphocytes are concentrated in the lymph nodes and other tissues inthe lymphatic system but can be found in all tissues of the body. Thereare two major categories of lymphomas: non-Hodgkin lymphoma(NHL) and Hodgkin lymphoma (HL). Both of these categories arefurther subdivided into numerous types, which differ in the way theydevelop and spread, as well as in the way they are treated. Therapyand prognosis are based on the stage at which the disease isdiagnosed and also are determined by the lymphoma type, in additionto a variety of other factors like age and other medical issues.
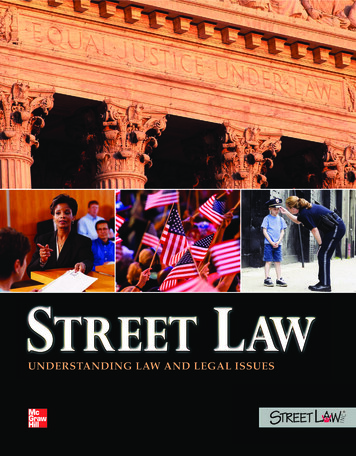
T/NK-cell lymphomas — These lymphomas develop from abnormalT lymphocytes or NK cells. They are less common and constitute upto 10 percent of patients with an NHL diagnosis.RELATIVE FREQUENCIES OF B-CELL LYMPHOMAS INTHE UNITED STATESChronic/Small lymphocyticleukemia/lymphoma: 25%Mantle cell lymphoma: 4%Lymphoplasmacytic lymphoma/Waldenström macroglobulinemia: 3%Precursor Non-Hodgkinlymphoma, B-cell: 6%Diffuse large B-celllymphoma (DLBCL): 29%B-cell not otherwisespecified: 7%Burkitt lymphoma/leukemia: 2%Hairy-cell leukemia: 1%Splenic MZL: 0.8%Extranodal MZL, MALT(c) type: 5%Follicular lymphoma: 14%Nodal MZL: 3%Percentages are based on the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) data,2008-2017. Some very rare types are not shown in the graph.15Understanding Non-Hodgkin Lymphoma
RELATIVE FREQUENCIES OF T-CELL LYMPHOMAS INTHE UNITED STATESSézary syndrome: 0.9%Angioimmunoblastic T-celllymphoma: 7%Subcutaneouspanniculitis-likeT-cell lymphoma: 0.6%Precursor Non-Hodgkinlymphoma, T-cell: 2%Non-Hodgkin lymphoma,not otherwise specified: 0.3%Prolymphocytic leukemia, T-cell: 2%T-cell large granular lymphocyticleukemia: 0.4%NK(c)/T-cell lymphoma, nasal-type/agressive NK(c)-leukemia: 4%Adult T-cell leukemia/lymphoma: 13%Anaplastic large celllymphoma, T-cell ornull-cell type: 9%Hepatosplenic T-celllymphoma: 0.6%Enteropathy-type T-celllymphoma: 0.7%Cutaneous T-cell lymphoma,not otherwise specified: 11%Primary cutaneous anaplastic largecell lymphoma: 4%Percentages are based on the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) data,2008-2017. Some very rare types are not shown in the graph.Another way to group NHL types is by how quickly they grow: Indolent (also called low-grade) lymphomas usually grow slowly andinitially exhibit few symptoms. Indolent lymphomas are generallynot curable, but they are usually highly treatable. Patients canlive a long time with these types of lymphomas because theytend to respond well to treatment and can remain in remission(disappearance of signs and symptoms) for many years or evendecades. However, over time, some indolent lymphomas maytransform into aggressive lymphomas.Aggressive lymphomas grow and spread more quickly than indolentlymphomas. However, aggressive lymphomas can often be cured bytreatments that kill rapidly dividing tumor cells.Learning the Basics16Part 1Mycosis fungoides: 25%Peripheral T-cell lymphoma, nototherwise specified: 20%
Pathologists (doctor who specializes in the diagnosis of diseases bystudying the cells from a patient’s body fluids and tissue samples) cantell the difference among the many different types of NHL byexamining biopsy tissue samples and blood and bone marrowsamples under a microscope and by carrying out various laboratorytests. This information is critically important in deciding how to treat thedisease in each patient.Table 1.1. Main Types of Indolent and Aggressive NHLs(Listed Alphabetically)Indolent NHLsAggressive NHLsChronic lymphocytic leukemia/smalllymphocytic lymphoma (CLL/SLL)Anaplastic large cell lymphoma (ALCL)Follicular lymphoma (FL)Lymphoplasmacytic lymphoma/Waldenström macroglobulinemia (WM)Marginal zone lymphoma (MZL)Mycosis fungoides (MF) (subtype ofcutaneous T-cell lymphoma)Angioimmunoblastic T-cell lymphoma(AITL)Burkitt/Burkitt-like lymphomasDiffuse large B-cell lymphoma (DLBCL)Lymphoblastic leukemia/lymphomaMantle cell lymphoma (MCL)Peripheral T-cell lymphoma, nototherwise specified (PTCL-NOS)Primary mediastinal large B-celllymphoma (PMBL) (subtype of DLBCL)Sézary syndrome (advanced subtype ofcutaneous T-cell lymphoma)17Understanding Non-Hodgkin Lymphoma
Common Types of Indolent Non-Hodgkin B-Cell and T-CellLymphomasIndolent B-Cell LymphomasChronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma(SLL) are a type of NHL involving small lymphocytes that can beprimarily in the bone marrow and blood (leukemia) or primarily in thelymph nodes (lymphoma). While these used to be considered twoseparate diseases, recent research has shown that CLL and SLLare essentially the same disease. If the malignant lymphocytes arefound mainly in the lymph nodes, the disease is called SLL. If morethan 5,000 malignant lymphocytes per microliter of blood are foundin the bloodstream, then the disease is called CLL. Because they areessentially the same disease presenting in different parts of the body,the two terms are grouped together as CLL/SLL. The most commonsigns and symptoms of CLL/SLL are swollen lymph nodes, fatigue,shortness of breath, anemia, bruising easily, and frequent infections.However, many patients may not experience any signs or symptoms,so CLL/SLL is often discovered during routine blood tests and/ora physical examination. More than half of CLL/SLL cases occur inpeople over the age of 70. Over time, CLL may occasionally progressto a more aggressive type of lymphoma, typically diffuse large B-celllymphoma (DLBCL); this is called a Richter transformation.For a more detailed description of CLL/SLL, see the UnderstandingCLL/SLL: A Guide for Patients, Survivors, and Loved Ones guide onthe Lymphoma Research Foundation’s (LRF’s) website atlymphoma.org/publications, or visit lymphoma.org/CLL.Learning the Basics18Part 1Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma
Follicular LymphomaFollicular lymphoma (FL) is the second most common type of NHLdiagnosed each year in the United States. Although it can affectpeople at any age, the average age at diagnosis is 60. FL usuallyappears in lymph nodes throughout the body, causing them to swell.Often one of the first signs is painless swelling in the neck, underarms,or groin caused by these enlarged lymph nodes. FL sometimestransforms into a more aggressive form of the disease.For more information on transformation, please see the TransformedLymphomas fact sheet on LRF’s website at lymphoma.org/publications.Follicular lymphoma is graded from 1 to 3 depending on the numberand pattern of certain large cells called centroblasts seen in biopsysamples. Grades 1 and 2 FL, which have no or only a fewcentroblasts, are considered to be low grade. Grade 3 FL can beeither grade 3a or 3b. Grade 3a is considered to be low grade andsimilar to grades 1 and 2; grade 3b FLs have more large cells, behavemore aggressively and are typically treated the same as transformedlymphoma/diffuse large B-cell lymphoma (DLBCL).For more information on FL, please visit LRF’s website atlymphoma.org/FL, or view the Follicular Lymphoma and FollicularLymphoma: Relapsed/Refractory fact sheets on LRF’s website atlymphoma.org/publications.Lymphoplasmacytic Lymphoma/Waldenström MacroglobulinemiaLymphoplasmacytic lymphoma is an uncommon B-cell lymphoma,with about 9,000 people newly diagnosed in the United States eachyear. Historically, the term Waldenström macroglobulinemia (WM) wasused to describe this type of lymphoma specifically characterized byabnormally high levels of a protein called immunoglobulin M (IgM) inthe blood, which causes the blood to thicken (hyperviscosity). Thedisease usually affects older adults and is primarily found in the bonemarrow, although the lymph nodes and spleen may sometimes beinvolved. Symptoms include fatigue, increased bleeding or bruising19Understanding Non-Hodgkin Lymphoma
easily, headache, dizziness, vision changes, abdominal pain,
*Thomas M. Habermann, MD, Mayo Clinic, Rochester, MN *Brad S. Kahl, MD, Washington University Medical School *Ann S. LaCasce, MD, MMSc, Dana-Farber Cancer Institute/ Harvard Medicine *John P. Leonard, MD, New York-Presbyterian Hospital/Weill Cornell Medicine *Peter Martin, MD, New York-Presbyterian Hospital/Weill Cornell Medicine