Transcription
Volume 39 Number 3January 31, 2016Radiologic Differentiation of Adrenal Lesions and ItsImpact on Patient ManagementElizabeth Chorney, MD, Ally Rosen, MD, Sara Lewis, MD, Eric Wilck, MD, andWilliam Simpson, MDAfter participating in this activity, the radiologist should be better able to recognize the appearance and distinguishingimaging features of common and distinctive adrenal lesions and become aware of the necessary follow-up recommendations.Category: General RadiologySubcategory: GUModality: CTKey Words: Imaging of Adrenal Lesions, Adrenal Adenoma,Adrenal Myelolipoma, Adrenal Hemorrhage, Pheochromocytoma,Adrenocortical Carcinoma, Adrenal MetastasisAdrenal lesions are a relatively common incidental findingand are estimated to be present in 4.4% of all abdominal CTscans.1 The detection of an adrenal lesion often necessitatesa thorough clinical evaluation that frequently requires a comprehensive patient history, biochemical studies, and radiologic studies such as dedicated adrenal protocol CT or MRI.The primary goal of additional radiologic studies is to differentiate benign from malignant adrenal lesions. It is, therefore, important for the radiologist to be familiar with a varietyof benign and malignant adrenal lesions and to recognizedistinctive imaging characteristics that can help make thisdistinction. This article reviews typical and useful imagingfeatures of more commonly encountered benign and malignant adrenal lesions.Evaluation With CT and MRICT and MRI are first-line imaging modalities used toevaluate incidental adrenal lesions. CT has the advantages ofbeing accessible, quick, and relatively inexpensive, particularly noncontrast CT. If an adrenal lesion has a density of 10HU or less, a diagnosis of lipid-rich adenoma can be madeconfidently with noncontrast CT.2 If the density of the adrenal lesion is above 10 HU, the addition of multiphase, contrast enhanced CT can be helpful to distinguish betweenadrenal adenomas and nonadenomas using absolute andrelative contrast washout percentages. These are calculatedfrom HU obtained during standard portal venous and 15-minutedelay acquisitions, as follows:Absolute Percentage Washout Relative Percentage Washout Dr. Chorney is Abdominal Imaging Fellow, Department of Radiology, Hospitalof the University of Pennsylvania, Philadelphia, Pennsylvania; Dr. Rosen isAssistant Professor of Radiology, Dr. Lewis is Assistant Professor of Radiology,Dr. Wilck is Assistant Professor of Radiology, and Dr. Simpson is AssociateProfessor of Radiology, Department of Radiology, Mount Sinai Medical Center, 1Gustave L Levy Place, Box 1234, New York, NY 10029; E-mail: william.simpson@mountsinai.org.All authors and staff in a position to control the content of this CME activity, andtheir spouses/life partners (if any), have disclosed that they have no relationshipswith, or financial interests in, any commercial organizations pertaining to thiseducational activity.Enhanced CT (HU) Delayed CT (HU) 100Enhanced CT (HU) Unenhanced CT (HU)Enhanced CT (HU) Delayed CT (HU)Enhanced CT (HU) 100An absolute percentage washout (APW) of more than 60%and a relative percentage washout (RPW) of more than 40%are typical of an adrenal adenoma.3In- and opposed-phase chemical shift imaging on MRI alsocan be useful to diagnose adrenal adenomas containing various amounts of microscopic intracellular fat. An adrenaladenoma can be diagnosed when there is loss of signalon T1 out-of-phase MR images compared with T1 in-phaseMR images because of the presence of microscopic fat.Lippincott Continuing Medical Education Institute, Inc., is accredited by the Accreditation Council for Continuing Medical Education to provide continuingmedical education for physicians. Lippincott Continuing Medical Education Institute, Inc., designates this enduring material for a maximum of 2 AMA PRACategory 1 Credits . Physicians should only claim credit commensurate with the extent of their participation in the activity. To earn CME credit, you must readthe CME article and complete the quiz and evaluation on the enclosed answer form, answering at least seven of the 10 quiz questions correctly. This continuing medicaleducation activity expires on January 30, 2017.1
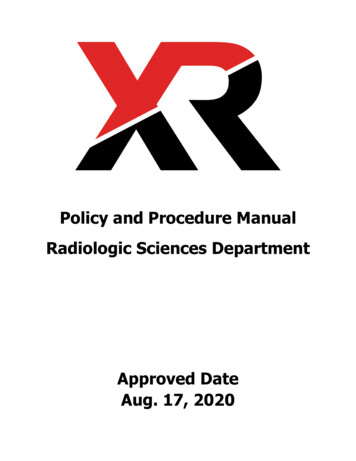
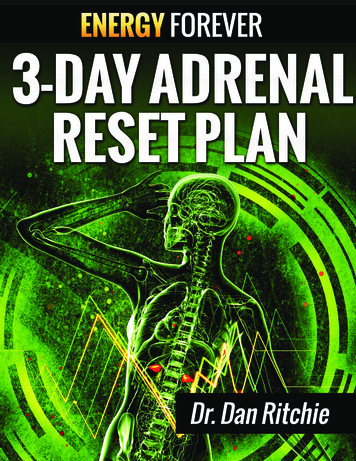
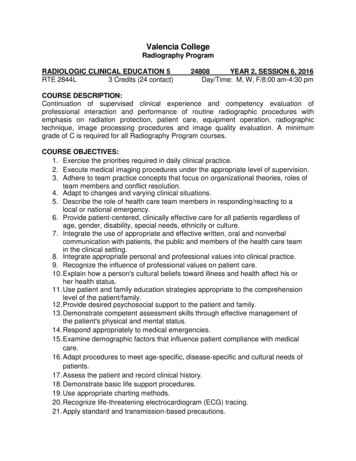
If quantitative measurement is desired, an adrenal signalintensity index can be calculated as follows4:Adrenal Signal Intensity Index Sl on In-Phase – Sl on Opposed-Phase 100Sl on In-PhaseAn adrenal signal intensity index greater than 16.5% istypical for a lipid-rich adrenal adenoma.4CT and MRI also are excellent imaging modalities to detectthe presence of macroscopic fat, which is a distinguishingfeature of adrenal myelolipomas. Other imaging characteristics that are not specific but can aid in assessment of incidental adrenal lesions include size, changes in size, enhancement,and morphology. CT and MRI analyses, in conjunction witha thorough clinical history that includes a history of nonadrenal malignancy, clinical biomarkers, and symptoms, alsoare important for the evaluation of incidental adrenal lesions.Benign Adrenal LesionsAdrenal Adenomas. Adrenal adenomas comprise themajority of incidentally detected adrenal lesions. Two keycharacteristics of adrenal adenomas that aid in radiologicdiagnosis include the presence of intracellular fat and rapidwashout of IV contrast medium. Lipid-rich adrenal adenomas contain various amounts of intracellular fat, which canbe evaluated using noncontrast CT and chemical shift MRIas described in the previous section. The majority of adrenal adenomas are lipid rich and can be characterized asAFigure 1. Axial, noncontrast CT scan demonstrates a smooth,well-delineated right adrenal mass (arrow) with homogeneousinternal attenuation and a density of 4 HU, compatible with anadrenal adenoma.lipid-rich adenomas with noncontrast CT or chemical shiftMR imaging (Figures 1 and 2). Some adrenal adenomascontain inadequate amounts of intracellular lipid and areindeterminate on noncontrast CT and chemical shift imaging; these adrenal lesions are considered lipid-poor adrenaladenomas, and they represent approximately 10% to 40%of all adrenal adenomas.3 Rapid washout of IV contrastmedium is a reasonably sensitive and specific way to diagnose an adrenal adenoma.Other, less-specific imaging features of adrenal adenomasinclude smooth, well-defined margins; homogeneous attenuation; and relatively small size.3 After the administration ofBFigure 2. A: Axial, T1-weighted, in-phase MR image demonstrates a round, well-delineated right adrenal lesion (arrow). B: Axial,T1-weighted, out-of-phase MR image demonstrates loss of signal because of the presence of microscopic fat, compatible withan adrenal adenoma.The continuing education activity in Contemporary Diagnostic Radiology is intended for radiologists.Contemporary Diagnostic Radiology (ISSN 0149-9009) is published bi-weekly by Lippincott Williams & Wilkins,Inc., 16522 Hunters Green Parkway, Hagerstown, MD 21740-2116. Customer Service: Phone (800) 638-3030;Fax (301) 223-2400; E-mail: customerservice@lww.com. Visit our website at LWW.com. Publisher, Randi Davis.Copyright 2015 Wolters Kluwer Health, Inc. All rights reserved. Priority Postage paid at Hagerstown, MD, and atadditional mailing offices. POSTMASTER: Send address changes to Contemporary Diagnostic Radiology, SubscriptionDept., Lippincott Williams & Wilkins, P.O. Box 1600, 16522 Hunters Green Parkway, Hagerstown, MD 21740-2116.PAID SUBSCRIBERS: Current issue and archives (from 1999) are available FREE online at www.cdrnewsletter.com.Subscription rates: Individual: US 723; international 1059. Institutional: US 1197, international 1359.In-training: US resident 146 with no CME, international 170. GST Registration Number: 895524239.Send bulk pricing requests to Publisher. Single copies: 52. COPYING: Contents of Contemporary DiagnosticRadiology are protected by copyright. Reproduction, photocopying, and storage or transmission by magnetic orelectronic means are strictly prohibited. Violation of copyright will result in legal action, including civil and/orcriminal penalties. Permission to reproduce in any way must be secured in writing; go to the journal website(www.cdrnewsletter.com), select the article, and click “Request Permissions” under “Article Tools,” or e-mailcustomercare@copyright.com. Reprints: For commercial reprints and all quantities of 500 or more, e-mail reprintsolutions@wolterskluwer.com. For quantities of 500 or under, e-mail reprints@lww.com, call 866-903-6951, or fax410-528-4434.2EDITOR: Robert E. Campbell, MD, Clinical Professor of Radiology,University of Pennsylvania School of Medicine, Philadelphia, PennsylvaniaEDITORIAL BOARD:Teresita L. Angtuaco, MDGeorge S. Bisset III, MDWilliam G. Bradley Jr., MD, PhDLiem T. Bui-Mansfield, MDValerie P. Jackson, MDMary C. Mahoney, MDJohnny U. V. Monu, MBBS, MscPablo R. Ros, MD, MPH, PhDWilliam M. Thompson, MDOpinions expressed do not necessarily reflect the views of the Publisher, Editor,or Editorial Board. A mention of products or services does not constituteendorsement. All comments are for general guidance only; professional counsel should be sought for specific situations. Indexed by Bio-Science InformationServices.
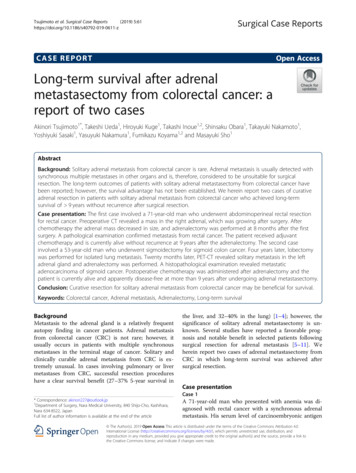
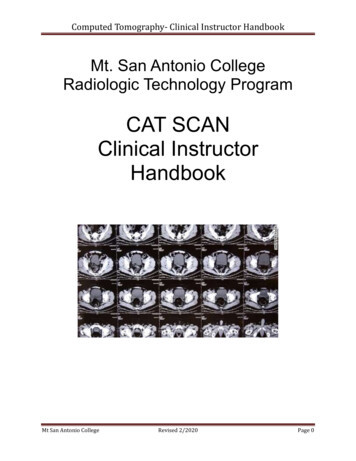
Figure 3. Axial, contrast enhanced CT scan demonstrates a leftadrenal mass with hazy soft tissue attenuation, fat attenuation,and a pseudocapsule (arrow), compatible with an adrenalmyelolipoma.contrast medium, enhancement is typically homogeneousand may demonstrate an arterial blush.5 It is important toremember that adrenal adenomas may hemorrhage, whichcan alter the attenuation characteristics. Compared with otheradrenal lesions such as metastasis, pheochromocytoma, andadrenocortical carcinoma, adenomas are typically smaller,with an average size of 2 to 2.5 cm; the largest adenomasmeasure approximately 3 cm.3Biochemical analysis is required to distinguish betweenfunctional and nonfunctional adrenal adenomas. Radiologicstudies are unable to distinguish between them; however,contralateral adrenal gland atrophy may suggest the presenceof a functioning lesion.3 Fortunately, the vast majority ofadrenal adenomas are hormonally nonfunctioning.Adrenal Myelolipomas. Adrenal myelolipomas arebenign tumors that contain macroscopic fat and hematopoietic tissue. The presence of macroscopic fat is their key distinguishing feature on CT and MRI (Figures 3 and 4). Themajority of adrenal myelolipomas have a pseudocapsule andcontain various amounts of soft tissue and macroscopic fat.Myelolipomas are typically asymptomatic; however, theymay become clinically apparent if they undergo hemorrhageor are symptomatic because of mass effect. Calcificationswithin them also may be present. A potential pitfall to recognize is that in rare cases, other adrenal tumors have beenreported to contain macroscopic fat, including adrenal adenomas, adrenocortical carcinoma, pheochromocytomas, andadrenal metastases.3AFigure 5. Coronal, noncontrast CT scan demonstrates a large rightadrenal hemorrhage with mixed internal attenuation, with areas ofmore acute high-attenuation hematoma (white arrow) and areasof more low-attenuation chronic hematoma (black arrow). Thelinear calcifications indicate a more chronic hematoma.Adrenal Hemorrhage. Adrenal hemorrhage has a varietyof etiologies but often is associated with an acute physiologicstress such as shock, sepsis, and surgery; and anticoagulationand hemorrhagic diathesis. Neonates are at a relatively higherrisk of adrenal hemorrhage compared with older children andadults. Adrenal hemorrhage can have a variable imagingappearance depending on the age of the hemorrhage and sizeof the hemorrhage. Acute and subacute hemorrhage willappear hyperattenuated on CT with progressive decrease inattenuation over time as the hemorrhage evolves (Figure 5).Chronic hematomas may develop calcifications. On MRI,adrenal hemorrhage will have variable T1 and T2 signaldepending on the age of the hematoma. Over time, a T1- andT2-hypointense rim may develop around the hemorrhagebecause of the presence of hemosiderin (Figure 6). The sizeof the adrenal hemorrhage should decrease over time anddemonstrate no postcontrast enhancement. Bilateral adrenalhemorrhage is caused more typically by systemic etiologies,such as sepsis and shock; whereas unilateral adrenal hemorrhage is caused more frequently by blunt trauma. Posttraumaticand neonatal stress-related adrenal hemorrhage more ofteninvolves the right adrenal gland, which has been attributedto the compression of the right adrenal gland between theBFigure 4. A: Axial, T2-weighted, HASTE MR image demonstrates a right adrenal lesion with a pseudocapsule (arrow). B: Axial,fat-saturated, T2-weighted, HASTE MR image demonstrates loss of signal on the fat-suppressed image because of the presenceof macroscopic fat in an adrenal myelolipoma (arrow). HASTE, half-Fourier acquisition single-shot turbo spin-echo.3
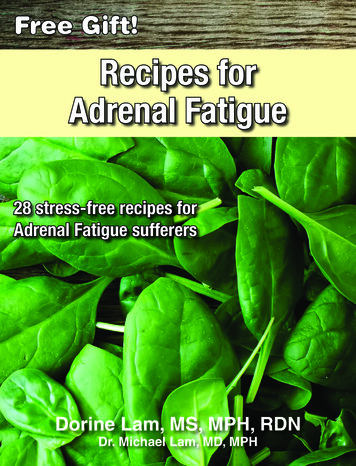
Figure 6. Coronal, HASTE MR image in the same patient as inFigure 5, obtained 2 months later, demonstrates a developinglow-signal hemosiderin ring (arrow) around the adrenal hematoma.liver and the right kidney. It is important to exclude an underlying adrenal lesion, such as an adenoma or myelolipoma,as the source of adrenal hemorrhage.Malignant Adrenal LesionsAdrenal Pheochromocytoma. Pheochromocytomas arecatecholamine (e.g., epinephrine and norepinephrine)-secretingtumors. Patients may have subclinical symptoms or presentwith symptoms of catecholamine excess including paroxysmal hypertension, diaphoresis, tachycardia, flushing, andheadache. Classically, pheochromocytomas appear hyperintense on T2-weighted MR images and can have internalareas of cystic necrosis (Figure 7). Pheochromocytomas arevascular tumors and typically avidly enhance after the administration of contrast medium. On T1- and T2-weighted MRimages, prominent vessels can create low-signal flow voidsagainst a hyperintense background, resulting in a classicallydescribed “salt and pepper” appearance (Figure 8).Figure 7. Axial, T2-weighted, HASTE MR image demonstratesa left cystic-appearing adrenal pheochromocytoma that is hyperintense (arrow).4Figure 8. Axial, fat-saturated, T1-weighted, contrast enhancedMR image demonstrates a large left adrenal pheochromocytomawith the classic “salt and pepper” appearance with heterogeneousenhancement and hypointense flow voids (arrows).The majority of pheochromocytomas are benign; however,approximately 10% of pheochromocytomas are malignant.Although both benign and malignant pheochromocytomastypically follow nonadenoma washout characteristics (APW 60% and RPW 40%), it is important to recognize thatpheochromocytomas may have washout characteristics thatcan mimic those of a benign adrenal adenoma.6Pheochromocytomas may be associated with familial syndromes such as multiple endocrine neoplasia 2, neurofibromatosis type 1, and von Hippel-Lindau disease. Theclinical and familial history and coexisting lesions in otherorgans (e.g., thyroid nodules, renal and pancreatic cysts,enlarged parathyroid glands, and central nervous systemhemangioblastomas) may offer clues to this diagnosis.Adrenal Metastasis. The imaging features of adrenalmetastases are nonspecific. Adrenal metastases may be bilateralor unilateral. Some adrenal metastases may have internalhemorrhage or necrosis (Figure 9). Typically, adrenal metastases will have slower washout compared with adrenal adenomas on delayed contrast imaging (APW 60% and RPW 40%). However, it is important to recognize that hypervascular metastases, such as renal cell carcinoma and hepatocellular carcinoma, may have similar washout to adrenaladenomas, particularly lipid-poor adrenal adenomas, ondelayed contrast imaging.7 Other highly suspicious imaginingfeatures of adrenal metastasis include large lesions ( 4 cm) orinterval growth between imaging studies. An adrenal lesionin a patient older than 60 years or with a personal history ofa malignancy should be scrutinized for metastasis.Adrenocortical Carcinoma. Similar to adrenal metastases, the imaging features of adrenocortical carcinoma arenonspecific. Typically, adrenocortical carcinoma will be a largeadrenal mass with heterogeneous enhancement (Figure 10).Hormonally functional adrenocortical carcinoma may presentat smaller sizes because of clinically apparent symptoms such as
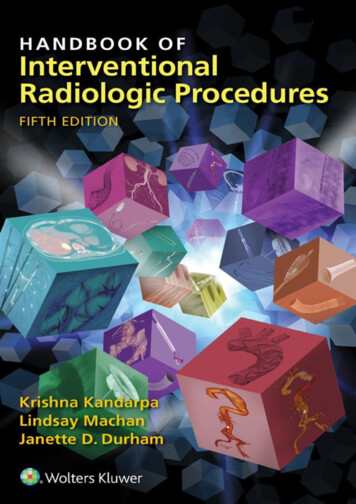
Figure 9. Coronal, contrast enhanced CT scan demonstrates alarge, partially necrotic, right adrenal metastasis with heterogeneous enhancement in a patient with hepatocellular carcinoma.Cushing syndrome, virilization, or feminization. Adrenocortical carcinoma may have areas of necrosis, and up to 33% willhave calcifications.3 As mentioned previously, it is importantto recognize that in rare cases, adrenocortical carcinoma maycontain macroscopic or microscopic fat, and it should not bemistaken for an adrenal myelolipoma or adenoma, respectively. Invasion of an adrenocortical carcinoma into the inferior vena cava is an important and well-known complicationto observe.Patient ManagementKey questions that guide patient management in the evaluation of an adrenal lesion include: what is the size of the lesion;and can the lesion be characterized as benign or malignant?Lesion size is an important but imperfect predictor of adrenalmalignancy. Smaller lesions tend to be benign, whereas largerlesions ( 4 cm) are more likely to be malignant. Therefore,adrenal lesions larger than 4 cm typically are considered forresection.8 A patient with no history of malignancy and anadrenal mass that is smaller than 4 cm with benign featuresgenerally is monitored.9 The frequency of surveillance isvariable depending on which organization’s consensus statement is followed. The American Association of ClinicalEndocrinologists recommends that patients with an adrenalincidentaloma not meeting criteria for surgical resectionshould have radiologic reevaluation at 3 to 6 months and thenannually for up to 1 to 2 years.8 The American College ofRadiology recommends a 12-month follow-up to confirmstability if there are no prior studies for comparison.10 Itshould be noted that more long-term biochemical follow-upmay be necessary to evaluate autonomous function. If anadrenal myelolipoma or a simple adrenal cyst can be diagnosed, there is usually no additional follow-up; however,surgical evaluation may be necessary if the lesion is symptomatic or large. If a lesion is indeterminate or has suspiciouscharacteristics, including but not limited to large size, increasein size, heterogeneous enhancement, or necrosis, furtherevaluation with biopsy or surgery may be necessary. It isimportant for the radiologist to recognize and consider typical imaging characteristics of a pheochromocytoma becausehemorrhage and hypertensive crisis have been reported asbiopsy complications.ConclusionAdrenal lesions are a relatively common finding in abdominalimaging, and the majority of adrenal lesions are benign.Familiarity with the imaging features of common benign andmalignant adrenal lesions is important to help guide patient management and follow-up. This CME activity emphasizes distinguishing imaging features of the more common benign andmalignant adrenal lesions that radiologists should recognize.ReferencesFigure 10. Axial, contrast enhanced CT scan shows a large (7.7 cm),right adrenocortical carcinoma with heterogeneous postcontrastenhancement.1. Bovio S, Cataldi A, Reimondo G, et al. Prevalence of adrenal incidentalomain a contemporary computerized tomography series. J Endocrinol Invest.2006;29:298-302.2. Blake MA, Cronin CG, Boland GW. Adrenal imaging. AJR Am J Roentgenol.2010;194:1450-1460.3. Johnson PT, Horton KM, Fishman EK. Adrenal mass imaging with multidector CT: pathologic conditions, pearls and pitfalls. Radiographics. 2009;29:1333-1351.4. Fujiyoshi F, Nakajo M, Fukukura Y, et al. Characterization of adrenal tumorsby chemical shift fast low-angle shot MR imaging: comparison of four methods of quantitative evaluation. AJR Am J Roentgenol. 2003;180:1649-1657.5. Rodacki K, Ramalho M, Dale BM, et al. Combined chemical shift imagingwith early dynamic serial gadolinium-enhanced MRI in the characterizationof adrenal lesions. AJR Am J Roentgenol. 2014;203:99-106.6. Boland GW. Adrenal imaging: from Addison to algorithms. Radiol Clin NorthAm. 2011;49:511-528.7. Choi YA, Kim CK, Park BK, et al. Evaluation of adrenal metastases fromrenal cell carcinoma and hepatocellular carcinoma: use of delayed contrastenhanced CT. Radiology. 2013;266:514-520.8. Zeiger MG, Thompson GB, Duh Q, et al. American Association of ClinicalEndocrinologists and American Association of Endocrine Surgeons MedicalGuidelines for the Management of Adrenal Incidentalomas. Endocr Prac.2009;15:1-20.9. NIH State-of-the-Science Statement on Management of the clinically inapparent adrenal mass (“incidentaloma”). NIH Consens State Sci Statements.2002;19:1-23.10. Remer EM, Casalino DD, Bishoff JT, et al. Incidentally discovered adrenalmass. https://acsearch.acr.org/list. American College of Radiology. AccessedJune 19, 2015.5
CME QUIZ: VOLUME 39, NUMBER 3To earn CME credit, you must read the CME article and complete the quiz and evaluation on the enclosed answer form, answering at leastseven of the 10 quiz questions correctly. Select the best answer and use a blue or black pen to completely fill in the correspondingbox on the enclosed answer form. Please indicate any name and address changes directly on the answer form. If your name andaddress do not appear on the answer form, please print that information in the blank space at the top left of the page. Make a photocopy ofthe completed answer form for your own files and mail the original answer form in the enclosed postage-paid business reply envelope. Onlytwo entries will be considered for credit. Your answer form must be received by Lippincott CME Institute, Inc., by January 30, 2017. At theend of each quarter, all CME participants will receive individual issue certificates for their CME participation in that quarter. These individualcertificates will include your name, the publication title, the volume number, the issue number, the article title, your participation date, theAMA credit awarded, and any subcategory credit earned (if applicable). For more information, call (800) 638-3030.All CME credit earned via Contemporary Diagnostic Radiology will apply toward continuous certification requirements. ABRcontinuous certification requires 75 CME credits every 3 years, at least 25 of which must be self-assessment CME (SA-CME) credits.All SAM credits earned via Contemporary Diagnostic Radiology are now equivalent to SA-CME credits (www.theabr.org).Online quiz instructions: To take the quiz online, log on to your account at www.cdrnewsletter.com, and click on the “CME” tab at the topof the page. Then click on “Access the CME activity for this newsletter,” which will take you to the log-in page for http://cme.lww.com. Enter yourusername and password. Follow the instructions on the site. You may print your official certificate immediately. Please note: LippincottCME Institute will not mail certificates to online participants. Online quizzes expire on the due date.1. The majority of lipid-rich adrenal adenomas can be characterized on the basis ofA. noncontrast CT densityB. appearance on radiographyC. ultrasound echotextureD. PET FDG avidityE. T2 MR signal5. Which one of the following primary carcinomas is most likelyto cause hypervascular metastases to the adrenal glands?A. PancreaticB. ColorectalC. BronchogenicD. GastricE. Renal cell2. Which one of the following adrenal lesions is most likely todemonstrate a low-signal rim about its periphery on MRI?A. Colonic metastasisB. Chronic hematomaC. Adrenocortical carcinomaD. AdenomaE. Pheochromocytoma6. An axial, contrast enhanced CT scan reveals an 8.0-cm adrenal mass with heterogeneous enhancement and associatedinvasion of the inferior vena cava. The most likely diagnosis isA. adrenal adenomaB. adrenal myelolipomaC. adrenocortical carcinomaD. adrenal cystE. adrenal hemorrhage3. A young male adult presents to the emergency departmentwith paroxysmal hypertension, tachycardia, flushing, and headache. A fat-saturated, contrast enhanced, T1-weighted, MRimage of the abdomen demonstrates an adrenal mass with a“salt and pepper” appearance. The most likely diagnosis isA. myelolipomaB. adenomaC. pheochromocytomaD. adrenocortical carcinomaE. metastatic hepatocellular carcinoma4. Figure 11 is an axial, unenhanced CT scan of the abdomenthat demonstrates an incidental left adrenal lesion. The mostlikely diagnosis isA. adrenal metastasisB. acute adrenal hematoma without an underlying adrenallesionC. pheochromocytomaD. adrenal myelolipomaE. adrenocortical carcinoma7. All of the following adrenal lesions can contain macroscopicfat, exceptA. adenomaB. acute adrenal hematoma without underlying adrenallesionC. myelolipomaD. adrenocortical carcinomaE. pheochromocytoma8. Which one of the following is required to differentiate a functional from a nonfunctional adrenal adenoma?A. Physical examinationB. History of malignancyC. Biochemical analysisD. Imaging CT washout study9. All of the following are causes of adrenal hemorrhage, exceptA. surgeryB. overhydrationC. shockD. sepsisE. anticoagulation10. The APW on CT required to diagnose an adrenal lesion asa benign adenoma is more thanA. 40%B. 45%C. 50%D. 55%E. 60%Figure 11.6
ious amounts of microscopic intracellular fat. An adrenal adenoma can be diagnosed when there is loss of signal on T1 out-of-phase MR images compared with T1 in-phase MR images because of the presence of microscopic fat. Volume 39 † Number 3 January 31, 2016 Dr. Chorney is Abdominal Imaging Fellow, Department of Radiology, Hospital