Transcription
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCA Trial Trifectaª THE JORDAN JENSEN STORYA Personal Narrative in Three Partsª ª ª CHAPTER 1: OCD IS HELLª CHAPTER 2: MY ROCKY ROAD OF ROMANCEª CHAPTER 3: CAREER CRUCIBLES1
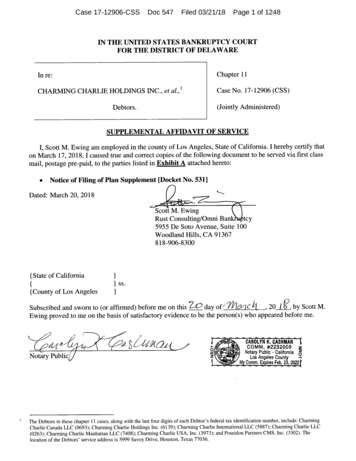
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCCHAPTER 1THE JORDAN JENSEN STORYPART Iª OCD IS HELL“In the quiet heart is hiddenSorrow that the eye can’t see.”– Susan Evans McCloud(1945-Present)Obsessive-compulsive disorder (OCD) affects approximately 2 percent of the population. Thisharrowing affliction touches lives in every corner of society. Many high profile persons from a variety ofsocietal sectors have suffered, or were believed to have suffered, from OCD. These individuals come froma wide range of fields, including art (Michelangelo), the armed forces (Thomas J. “Stonewall” Jackson),science (Charles Darwin and Albert Einstein), music (Ludwig Van Beethoven), business (Donald Trump),athletics (David Beckham), and entertainment (Justin Timberlake, Katy Perry, Harrison Ford, PenélopeCruz, and others).OCD symptoms include obsessive thoughts and compulsive behaviors. For persons suffering withOCD, obsessive thoughts are unwanted and often turn into agonizing ruminations that cause great mentalanguish. Compulsive behaviors are then undertaken to reduce the anxiety produced by the obsessivethoughts – often evolving into irrational rituals. While everyone may experience some obsessive thoughtsand compulsive behaviors, a person with clinical OCD often experiences symptoms that consumesignificant amounts of time and interfere with normal, daily functioning.CAUSES OF OCDIt is hard to identify exactly what causes OCD, but a combination of genetic, social, chemical, andenvironmental variables are typically involved in its onset and exacerbation. It is sometimes referred to as“the doubting disease,” and common obsessions include intrusive doubting, sexual thoughts, religiousblasphemy, incurring harm to self and others, order, symmetry, cleanliness, and fear of germs. Typicalcompulsions include washing, checking, ordering, and repeating words and prayers. Compulsions can beaccompanied by involuntary body, facial, and verbal tics. Trichotillomania (hair plucking and skin picking)may also accompany an OCD diagnosis. Personally, I have struggled with trichotillomania in the form ofskin pulling for much of my life.OCD’S INSIDIOUS CYCLEOCD manifests itself in a three-step, cyclical process. The first step involves intrusive, unwanted,obsessive thoughts that trigger anxiety. The second step involves ritualistic, compulsive behaviorsperformed in hopes of alleviating the anxiety. The third step involves the experience of relief. The pattern2
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCthen painfully repeats itself until a combination of time and/or therapy, medication, and personal growthcan break the cycle.ReliefObsessionANXIETYCompulsionFigure 14.1 OCD’s Insidious CycleOne of my mental health counselors explained it this way: All people have a variety of would-bethoughts waiting to enter their minds at any given moment. However, human brains have a screen-likefiltering process that filters out most OCD-oriented thoughts. For those with OCD, however, the “holes” inthe brain’s screen become enlarged, allowing a host of thoughts to pass into the mind that would typicallynot rise to the level of conscious thought. It is believed that certain medications (i.e., selective serotoninreuptake inhibitors, or SSRIs) may decrease the size of these holes and thereby prevent obsessive thoughtsfrom slipping past the mind’s filter. Symptom alleviation for many patients, including my own, serve tocorroborate this medicinal hypothesis.THE IMPACT OF OCD ON LOVED ONESHaving OCD can produce negative effects on family members and friends. A substantialpercentage of those with OCD do not marry. Those who do wed tend to marry later in life and have troublesustaining healthy marital relationships.1 Negative effects can impact other family members as well. Inmore serious cases, these effects can include “serious disruption of family functioning and overt conflict.”2While serving my LDS mission, my mission president suggested that my OCD would influencemy role as a husband and father. I chose to interpret his observation as an important caveat for my future.Desperately desiring to avoid the dangers and damages to family life I knew OCD could create, and hyperaware of the negative influence my father’s bipolar disorder had on my parent’s marriage, this forewarningwas a trigger that motivated me to “attack” my OCD with exceptional vigor. This cautionary advice, inconcert with a pathological romantic letdown that occurred shortly after returning home from my mission,led me to seek out regular therapy. I yearned for emancipation from my OCD.12De Silva, P. (2003). The Phenomenology of Obsessive-Compulsive Disorder. In R. G. Menzies & P. de Silva (Eds.), ObsessiveIbid. Page 36.3
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCMETHODS OF TREATMENTThere are many methods of treating OCD. The two most common are cognitive-behavioraltherapy (CBT) – including exposure response prevention (ERP) – and medication. Other, lesser known,treatment options also exist. Examples of lesser-known treatments for OCD include: homeopathy,acceptance and commitment therapy (ACT), progressive relaxation training (PRT), repetitive transcranialmagnetic stimulation (rTMS), and in extreme cases, neurosurgery. My experience with treatment includesCBT, medication, as well as self-help and spiritual approaches that involved a combination of regularprayer and short-term fasting. My fasts usually lasted 24-hours or less, and were performed, on average,once per month.COGNITIVE-BEHAVIORAL THERAPYCognitive therapy (CT) focuses on what a patient is thinking. Behavioral therapy (BT) focuses onwhat a patient is doing. The goal of CBT is to rationalize, minimize, diminish, or eliminate obsessivethought processes and their accompanying behaviors. CBT is usually undertaken with a licensedprofessional, such as a counselor, psychologist, or clinical psychiatrist. Generally speaking, CBT—including exposure response prevention (ERP), which is a form of CBT that will be explained in detail inthe next section—is considered the best method for treating OCD.CBT was vital to my successful, long-term management of OCD. In therapy, I was introduced toDr. David Burns’ list of cognitive distortions:1). All-or-nothing thinking2). Overgeneralization3). Mental filter4). Disqualifying the positive5). Jumping to conclusions6). Magnification (catastrophizing) or minimization7). Emotional reasoning8). Should statements9). Labeling and mislabeling10). Personalization3My personal and therapeutic goals were to escape the shackles of these cognitive distortions, manyof which had a near-stranglehold on me. I wanted to see things as they really were, not as my troubled mindfiltered them to appear. By applying insights from my counseling sessions, I was able to apprehend,confront, and replace cognitive distortions with more accurate conceptions of reality. This, in turn, led intime to much personal growth and progress.EXPOSURE RESPONSE PREVENTIONExposure response prevention – known as ERP – is one of the most prominent and successfulmethods of cognitive-behavioral therapy used to treat OCD. ERP is a counterintuitive healing method inthat it requires a patient to confront (consciously think more about) the very thoughts he has been trying toavoid, and to refuse to act on any concomitant compulsions she feels duty bound to perform. Initially, ERPis likely to increase a patient’s anxiety (sometimes severely). However, if he persists, his heightenedanxiety will eventually diminish. Repeated mental and physical exposure tends to lead to a welcomedreprieve from obsessions and compulsions over time.ERP takes courage and commitment. But the long-term benefits almost always outweigh the shortterm anxiety and pain. Research continually validates ERP as one of the best methods of treating OCD.Research further corroborates that ERP and other forms of cognitive-behavioral therapy have the capacity3Burns, D. (2009). Feeling Good: The New Mood Therapy (Revised and Updated Edition). New York, NY: Harper Health. Pages42-43.4
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCto positively affect—and even alter—brain chemistry in the long run. This is significant because it meansthat ERP may be able to permanently accomplish what medication can only temporarily manipulate.From my own experiences, I can vouch for CBT’s (including ERP’s) capacity to alter brainfunctioning. In conjunction with medication, CBT, ERP, and other approaches, I have been able todrastically reduce, and in some cases virtually eliminate, many strains of obsessions and compulsions Isuffered dreadfully from in the past.MEDICINAL TREATMENTSMedicinal approaches (i.e., drug treatments) are also commonly used to treat OCD. Selectiveserotonin reuptake inhibitors (SSRIs) are typically the drugs of choice for pharmacotherapy. Examples ofSSRIs include citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), fluvoxamine (Luvox),paroxetine (Paxil), and sertraline (Zoloft). Other drugs used to treat OCD include the tricyclicantidepressant (TCA) clomipramine (Anafranil), the serotonin-norepinephrine reuptake inhibitor (SNRI)venlafaxine (Effexor), and the benzodiazepine (BZD) alprazolam (Xanax).Common side effects of these drugs include lethargy, restlessness, and dizziness. Minor sexualside effects are also common. An OCD patient should work closely with one’s doctor to achieve the rightdosage to maximize benefits and minimize side effects. The effectiveness of one drug over another dependson the patient and her genetic makeup and physiology. Family members tend to respond similarly tovarious medicinal treatments.4Since 1997, when I was first diagnosed with OCD, I have personally been treated by six of thesedifferent drugs. I currently take 20 milligrams of escitalopram (Lexapro) once each day—to my benefit.While the medication does not eradicate all my symptoms, and though it cannot achieve the same long-termresults of—or replace—CBT and ERP, it does serve to take the edge off, which helps me keep my OCDshrunk down to a “faint hum in the background of my life, rather than a blaring bugle in the forefront”thereof.5 Indeed, I am grateful for the benefits that medication have brought to my life, and to this day,continue to utilize it as one weapon in my war chest for combatting both OCD and depression.HOMEOPATHY & SELF-AWARENESSHomeopathy is a lesser-known treatment method. Australian Mark Simblist promoteshomeopathic treatments that could potentially align effectively with SAL practices. Homeopathic methodsinclude “a humane and caring approach” that focuses on comprehensive treatment plans including:6 Different forms of vibrational medicine (e.g., flower or shell essences).Counseling, therapy, or group therapy.Regression techniques to confirm facts (e.g., kinesiology, hypnotherapy).Various forms of energy clearing techniques, breath and bodywork.Techniques to change a person’s “core beliefs” (e.g., affirmations).Meditation and raised spiritual consciousness.The homeopathic similimum.7While I have never pursued any extensive homeopathic treatments for my own OCD, I am aproponent of Simblist’s philosophy that therapy should be comprehensive, holistic, and ultimately selfreliant. I also believe individual patients should consider, and perhaps even try, a variety of treatmentoptions in a diligent quest to find what treatment approach works best for one’s individual case of OCD.This is because, unlike physical maladies, which tend to operate more predictably from person-to-person,every case of OCD is unique to the individual. There is, therefore, no “one-size-fits-all” method of4I learned this point from one of my psychiatrists. In addition, several members of my family have taken Celexa for depression, andall of us have found similarly positive results.5This is a paraphrased quote from one of my psychiatrists, Dr. Brent L. Griffin, of Provo, Utah.6Simblist, M. (1998). Homeopathy and Obsessive-Compulsive Disorder. The Journal of Australian Homeopathic Association Inc.Volume 11, Issue 2, p 18-21. Page 20.7Ibid. Page 20.5
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCtreatment, nor is their a set timetable for healing.MY EXPERIENCES WITH OCDCOARSELY CROSSEDCoarsely crossed, the angst-filled smartOf agony did fill my heart.An outgrowth of my humbling path,Bedecked with the refiners wrath,That ripped my soul and taxed my mind,Beat me through life’s unending grind,That was ordained to make a king,Who after night is o’er will singA thousand praises to the cause,That aided an end to my flaws.As to the realms of royal right,I will transcend the cold dark night,And gratefully begin to seeThe road into eternity’sA path that starts and ends with He.And all between calls upon me!THE UNPARDONABLE SINI grew up in a religious family that valued faith, fellowship, and freedom. Moreover, I was, bynature, sensitive to religious and spiritual matters. Adding OCD to this mix concocted a toxic cognitivecocktail to my life, causing me to developing strain of OCD known as “religious OCD” (ROCD),8 orscrupulosity.9This section details an experience that occurred in 1992 when I was just starting junior high(seventh grade). At that point in time, I was still four-plus years away from any awareness that I wassuffering from a clinically diagnosable mental disorder.According to my church’s theology, the most severe of all sins is becoming a “son of perdition,”which involves denying the Holy Ghost. LDS doctrine is very clear on this point: “For behold, if ye denythe Holy Ghost when it once has had place in you, and ye know ye deny it, behold, this is a sin which isunpardonable.”10 According to Mormon theology, denying the Holy Ghost is a sin that relatively fewpeople are even capable of committing because it typically requires sentient experience with Deity (anabsolute knowledge of God). It further requires that such a person turn wholesale against God and workintentionally to destroy His work after having once been fully committed thereto. The problem was, I wasnot fully aware of these important details at the time, and in seventh grade, I began to obsessively fear that Icould be found guilty of this most heinous of sins against God by involuntarily ruminating on thoughts ofdenial.Such thoughts were anathema to me, and that is precisely what triggered the obsession. OCD is avicious bully that takes great glee in diabolically dangling everything a patient holds most dear over thecliff of cognitive distortions. It is, therefore, not uncommon for OCD to create massive cognitivedistortions about a person’s most precious beliefs and ideals. The more awful and repulsive the thought oraction, the more the OCD mind seeks to replay it—to the great pain of the patient.In grave desperation, and naively fearing for the welfare of my soul, I finally confessed my8See Himle, J. A., Chatters, L. M., Taylor, R. J., & Nguyen, A. (2011). The Relationship Between Obsessive-Compulsive Disorderand Religious Faith: Clinical Characteristics and Implications for Treatment. Psychology of Religion and Spirituality.Volume 3, Issue 4, p. 241-258. DOI:10.1037/a0023478.9See Rosmarin, D. H., Pirutinsky, S., Pargament, K. I., & Krumrei, E. J. (2009). Are Religious Beliefs Relevant to Mental HealthAmong Jews? Psychology of Religion and Spirituality. Volume 1, Issue 3, p. 180-190.10Alma 39:6 (The Book of Mormon).6
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCproblem to my parents. Lacking the insight to discern the symptoms of a mental disorder, they mistakenlyperceived my plight to be a mere case of childlike misunderstanding—which it certainly was. As concernedand loving parents, they assured me I was in no danger of becoming a son of perdition.Mom and Dad were not the slightest bit worried about my spiritual state, but these clarificationshelped a great deal in easing my mind in the matter. Clearly, I was not a candidate for perdition. In helpingme to this conclusion, my parents had unwittingly extended a healthy dose of cognitive therapy.Fortunately, it worked. Unfortunately, this was just the beginning of a whole slew of OCD symptoms thatwere about to latch on to my troubled brain. As my obsessions surrounding religious blaspheme began tosubside, other, just as insidious symptoms began to plague my mind. Thus began an on-going saga thatwould last over a decade whereby I found myself continually shackled in one mental prison or another.UNWANTED SEXUAL THOUGHTSUnwanted sexual thoughts are among the most common symptoms of OCD. As a teenager, I likedgirls and was therefore naturally curious about female anatomy and sex. Most of my sexual thoughts,however, were not triggered by my natural inclinations, but by my OCD. My sexual obsessions were alsostrongly influenced by my ROCD. The connection between unwanted sexual thoughts and scrupulosity wastriggered by my church’s counsel to avoid preoccupation with sexual thoughts. The operative word in theecclesiastical injunction was, of course, “preoccupation,” which is good advice for any teenager. However,due to OCD, my brain tended to see things in “all-or nothing” dichotomies.11 At the time, I did not clearlyunderstand the difference between “preoccupation with” and natural, passing thoughts on the matter.Worried that I was sinning by merely having a sexual thought, my mind began to involuntarilyobsess about thoughts of having sex with girls and women. Any female I saw would trigger the unwantedobsession, and I would become very anxious about the possibility of someone—especially the girl orwoman—discovering my thoughts. It was a wretched experience.After a few weeks of horrific mental and spiritual anguish, I again went to my parents. Once morethey assured me I was okay. My father, who clearly—albeit erroneously—viewed my problem as thenatural inclinations of a typical teenage boy, was especially reassuring and said, “Jordan, there isn’t athought you’ve thought that I haven’t thought a lot more and a lot longer than you have.” Such anoutpouring of love, concern, and attention from Mom and Dad made all the difference—for about a day. Iwent to bed feeling free and comforted, only to wake up the next day and find that my mind—everdetermined to magnify misery—shifted my obsession from heterosexual to homosexual thoughts.Agonizing over this new variation on a theme, my suffering continued for months. When I couldtake it no more, I went again—in tears—to my parents for comfort and relief. It was evident this timearound that they were growing increasingly perplexed at the pattern that was developing with their sixthchild. Unaware of the root cause of my affliction, they simply didn’t know how to best help me.Following this third, dramatic, tear-filled episode, I stopped opening up to my parents on a regularbasis about my obsessions. First of all, it was difficult—and embarrassing—to disclose intimate details ofsuch thoughts to my parents, despite our close and healthy relationship. Second, over time, reality set inwhereby I realized that I likely had “miles to go before I slept” with regards to this malicious mentalmalaise.12 Third, unaware I had a mental disorder and could seek out professional help, I increasinglybegan to think—and to some degree accept—that I was just really weird or that there was somethingterribly wrong with me.GERMS, BLOOD, AND STEROIDSOver time, an evolution in my unwanted sexual thoughts localized around contact with germs. Ibecame an obsessive hand washer, although not to the degree that marks some sufferers of OCD. I alsobecame fearful of blood—my own, and that of others. My fear was born out of a dubious associationbetween blood (generally speaking) and the concomitant fear of contracting the acquired immune1112Burns, D. (2009). Feeling Good: The New Mood Therapy (Revised and Updated Edition). New York, NY: Harper Health. Page32.A paraphrased line from Robert Frost’s poem, Stopping By Woods on a Snowy Evening (1923).7
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLCdeficiency syndrome (AIDS), a condition caused by the human immunodeficiency virus (HIV). Myirrational fear was that I could somehow pick up HIV from someone else, even though I was not engagingin any behavior that put me at risk. Even more nonsensical was my fear that I might somehow infectsomeone else with my own blood, even though my blood was contaminant free of HIV or any otherdisease. This fear led to the development of compulsive Band-Aid wearing, which was ironicallyexacerbated by a mild form of trichotillomania (skin picking) that caused my skin to occasionally bleed. Italso led to a general avoidance of touching objects I believed could have been exposed to blood in any way.As I became more involved with athletics in high school, my germ, blood, and AIDS obsessionevolved into a new fear that I might accidentally ingest anabolic steroids into my body. The use of bannedsubstances is always against the rules in ethically run sporting programs. The word “rules” became thetrigger, because another of my compulsion’s had developed around my obsessive need to adhere to rulesand regulations with exactness—often to a ridiculous and illogical degree. Because I was obsessed withkeeping certain rules, my mind would obsessively conjure up ways in which I might inadvertently break therules—like my fear of capriciously ingesting steroids, which was completely irrational.To be clear, I never used steroids. I did not even know of anyone in my community who used—orhad access to—steroids. I never had an opportunity to even see, much less use, banned substances.Moreover, I never had the slightest desire, temptation, or intention to do so. I nonetheless remained fearful Imight somehow ingest them in my body and would therefore be “breaking the rules,” thereby becoming a“dishonest person” whose achievements were illegitimate and deceitful. In response to these obsessions, Ideveloped various compulsive behaviors involving when, where, and how I would wash and clothe myself.These even dictated where I placed personal belongings to avoid the calamitous event of accidentallyingesting steroids or picking up particles of blood that would somehow end up in my bloodstream.I recall one day watching my older brother get dressed after taking a shower and feeling jealous ofhis ability to put his clothes on with such ease – without having to tip-toe around, or complete any of theother time- and energy-consuming compulsions I felt I “had” to do just to don my own clothes.During my junior year, I became increasingly successful as a runner. My victories caused mysteroid obsessions and compulsions to grow even more severe and debilitating. It seemed as though themore races I won, the worse the symptoms became. It was as if my brain was intent on sabotaging thesuccess (or at least the satisfaction of the success) I was starting to enjoy. I experienced the worst of it inthe two weeks leading up to the state championship race—which I eventually won. As I packed for the trip,I obsessively stressed about it; as my team and I rode up to Salt Lake City for the meet, I obsessed evenmore. In the hours leading up to the race itself, the obsessions and related compulsions maintained a firmgrip on my mind and behavior. evenmoreconsciousthoughtandenergy.HONESTY THE BEST POLICY?Paralleling my unwanted thoughts surrounding sexuality, germs, blood, and steroids was anothergrowing obsession involving honesty that would torment me for many years. It included following “therules” to the letter, always doing “the right thing,” and telling “the truth, the whole truth, and nothing butthe truth, so help me OCD.” Such efforts—inherently good in and of themselves—became pathological asthe vice grip of OCD squeezed tighter and tighter around my mind. Because this obsession was triggeredand influenced by ROCD, I became something of a well-intentioned Pharisee, perpetually unable to see theforest for the trees.A particular event during ninth grade triggered this new and metastasizing obsession. In myseminary class, I was reintroduced to a verse of scripture I had read over several times previously in mylife. This time, however, it struck my mind with obsessive force and would not let go. The verse read,“Woe unto the liar, for he shall be thrust down to hell.”I had always been an inherently honest person. It was not in my nature to lie, cheat, or steal.Nevertheless, after reading about liars being hurled to Hades, my already honest nature was seized upon byan honesty compulsion that was, to say the least, absurd.That same semester, I had procured a license to go mule deer hunting. One day, I was up on mydad’s land hunting with a cousin. As we took turns shooting at deer within the sights of our rifles, a pickuptruck came rolling along the dusty dirt road where we had been firing. When it arrived where we stood, aman got out of the truck and confronted us about where we had been shooting. As it happened, his home8
A Trial Trifecta Self-Action Leadership ³ Dr. Jordan R. Jensen ³ 2015 Freedom Focused LLC(and family) was about three-quarters of a mile or so from where we had been firing, and he was thereforeunderstandably concerned about where we had been aiming our high-powered rifles. He asked me if wehad been shooting in the direction of his house—to the east of us. My mind nervously replayed the shotswe had taken toward the west, and I quickly blurted out that we had not taken shots toward the east.Almost as soon as I said it, I realized that we actually had taken a few shots to the east. When Irealized the half-truth I had inadvertently told, I began to feel sick to my stomach. Too afraid to admit mypartial deception after my inner realization, the man parted ways with us after adding a word or two inpromotion of safe hunting practices. As we climbed on the all-terrain vehicle that carried us home thatnight, I was beside myself knowing I had not been completely honest with the man—even though my fibhad been unintentional.For the better part of the next year, I might as well have gone to hell because of the mentalanguish over that small accidental mistruth. I replayed the incident and reflected on it over and over again.As I did, the guilt, fear, and agony I suffered reached proportions of the most poignant extremity. Manytimes I contemplated going back to the man’s house to confess my lie, but as bad as my obsessive guiltwas, my fear of confession was even worse. Every time I would drive by his home, and on countless otheroccasions, the obsessions and vacillations would return. My mind could find no peace.It was common for my obsessive thoughts to swoop down and do their worst at the very momentswhen I was feeling happiness or peace—thus sucking the joy out of many otherwise positive experiences.For example, one night, as I lay in bed thinking about my future as a competitive runner, I was filled with aspontaneous, joyful anticipation of the future. It was a wonderful feeling! In the midst of this joy, however,my obsessive mind interjected into my thoughts to remind me of the accidental mistruth I had told the man.Suffice it to say, all of the evening’s erstwhile joy had been squelched.Finally, after about nine months had gone by, I could take it no more. Mustering up all my courageand praying for strength, I returned to the man’s house one Sunday afternoon after church. I knocked on hisdoor, confessed my error, apologized, and then drove home having finally relinquished one of the mostexcruciating burdens I had ever borne. I had repented of my sin, and could finally find peace. The man wasnot angry and I felt better after confessing; I was finally able to put the matter to rest.This act, while morally noble in my own mind, reeked of obsessive-compulsivity on another (had Iintentionally lied to the man, it would have been a different story). My inability to recognize I hadcommitted a momentary mistake—not a malicious deception—allowed OCD to begin its vicious cycle. Asa result, the confession actually made things worse in the sense that it reinforced the cycle of compulsivebehavior to alleviate anxiety. Giving in to compulsions guarantees not only that the obsessions will return,but increases the likelihood they will return with greater force. While confessing my accidental “white lie”brought my conscience temporary peace, it also further fueled my honesty obsession. It was only a matterof time before the next trigger would start a whole new cycle of unnecessary anxiety and guilt.The deeper I plunged into this new strain of obsessive thinking, the more closely my obsessivemind stringently policed my every word and deed. In my mind, the slightest deviation from the absolutetruth, regardless of the situation, was not to be tolerated. The problem with this, of course, is that 100percent completely honest communication in every situation is not only unrealistic, but can also be bothunwise and unkind. No matter how well intentioned a person might be in regards to truth-telling, there aremany flaws in human communication that make it virtually impossible to live up to the standard my OCDdemanded I uphold. This strain of OCD created many awkward social situations, and my compulsiveconfessions and apologies sometimes did more harm than good. They certainly surprised—and probablyconfused—a lo
OCD symptoms include obsessive thoughts and compulsive behaviors. For persons suffering with OCD, obsessive thoughts are unwanted and often turn into agonizing ruminations that cause great mental anguish. Compulsive behaviors are then undertaken to reduce the anxiety produced by the obsessive