Transcription
9/14/2015Fascial ManipulationCarl Heldman PT, DPT, MA, MTC, ATC, FAAOMPT1
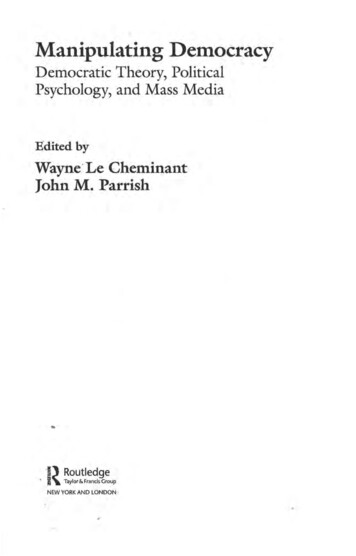
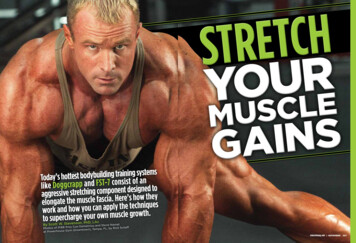
9/14/2015FASCIAL MANIPULATION Fascia is a connectivetissue: All connective tissueis derived fromembryological mesodermlayerLEVEL 1: DEEP FASCIAAND EPIMYSIAL LAYER(Perimysium and endomysium)LEVEL 2: DEEP FASCIAAND RETINACULALEVEL 3: SUPERFICIALFASCIA INTERNALDYSFUNCTIONCNSMODULATIONCATEGORIES OF THE PAINAND MOVEMENT REASONINGMODEL.Diagram overviewREGIONALINFLUENCESLOCALSTIMULATION2
9/14/2015Convergence Somatic-somatic Viscero-somatic(Level 3 FMID)Kinetic chain Hypermobility Hypomobility cs Weakness Parasthesias Reflexes Neural/connective tissue interfaceKINETIC CHAINSUGGEST DYSFUNCTION REMOTE TO THE SITEOF PAIN Biomechanically-related tissues such asproprioception, hypermobility, and hypomobility Assumption is that when elements of the “chain”are not providing normal support or alternatively,flexibility, then movement along the chain can beadversely effected Takes into consideration that muscles, joints, andconnective tissues are a continual matrix and theirmovements are inter relatedCENTRAL ORIGIN OFMPS“There is evidence of central nervous system sensitizationand of hyperalgesia and temporal summation of pain in aspecific area. Another hypothesis would suggest afacilitated processing of pain messages in the centralnervous system, perhaps manifested by neuralreorganization in the brain, brainstem, and spinal cord.”Younger JW, Shen YF, Goddard G, Mackey SC.; Chronic myofascial temporomandibular pain isassociated with neural abnormalities in the trigeminal and limbic systems. ; Pain. 2010May;149(2):222-8.3
9/14/2015PERIFERAL ORIGIN OFMPS“The peripheral theory suggests, in contrast, thatmyofascial pain is due to an alteration of innervations orof nerve stimulation of muscles or of fascia. This theoryis based to the hypothesis that the fascia could beconsidered as a proprioceptive organ, and that it couldbe altered by trauma, overuse and surgery.”Stecco C, Stern R, Porzionato A, Macchi V, Masiero S, Stecco A, De Caro R; Hyaluronan within fasciain the etiology of myofascial pain.; Surg Radiol Anat. 2011 Dec;33(10):891-6.4
9/14/20151.Fascial Layers2. Histology3. InnervationSOME QUESTIONS WHY DO MUSCLES INSERT ONTOOR ORIGINATE FROM FASCIA? FASCIA HAS AN INTRICATESTRUCTURE, SO WHY ONLYDESCRIBED AS HAVING A ROLE FORCONTAINMENT? CAN MUSCLES PERFORM MORETHAN ONE MOVEMENT, AND ISFIBER ACITIVATION TASKORIENTED? COULD FASICA PLAY AN ACTIVEROLE IN MOTOR LARCOLLAGEN FIBERS LAYEREDORGANIZATIONAPONEUROTIC FASCIAEPIMYSIALFASCIA5
9/14/2015FASCIALLAYERS(Perimysium and endomysium)SUPERFICIAL FASCIA The retinacula cutis provide an anchorageof skin to underlying tissues and of thesuperficial fascia to the deep fascia. In this way a flexible and yet resistantmechanism of transmission of themechanical loads from multi-directionalforces could be recognized. Regional specializations determine thevariations in mobility of the skin withrespect to underlying tissues.Classification of the deep fascia6
9/14/2015DEEP FASICA NAMED FOR THE SEGMENT ITSURROUNDS; i.e brachia fascia, cruralfascia LOOKS LIKE A SECOND SKIN BENEATHTHE SUPERFICIAL FASCIADEEP FASCIA IT’S CONTINUOUS WITH LIGAMENTS,RETINACULA, TENDONS AND EPIMYSIUM IN PART IT IS FREE TO GLIDE OVERMUSCLES, AND IN PART IT IS FIRMLYANCHORED TO BONEDEEP FASCIA IT’S INNER SURFACE PROVIDESINSERTIONS FOR MUSCLE FIBERS pectoralis major fascia in continuity with thebrachial fascia7
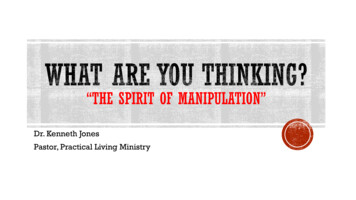
9/14/2015DEEP FASCIADEEP FASCIA UNDULATED PARALLEL COLLAGEN FIBERS,FEW ELASTIC FIBERS ARRANGED INLAYERS WITH DIFFERENT ORIENTATION LOOSE CONNECTIVE TISSUE BETWEENTHE LAYERSDEEP FASCIALCTLCTLCTLCTTHIGHARMBoth the fasciae are formed by two to three layers of collagenfibre bundles separated by a thin layer of loose connective tissue(LCT) that permits the different layers to slide one on the other.Magnified view8
9/14/2015SemiaponeuroticLayersBoth the fasciae are formed by two to three layers of collagenfibre bundles separated by a thin layer of loose connective tissue(LCT) that permits the different layers to slide one on the other.DEEP FASCIAThe presence of loose connective tissueinterposed between adjacent layers permits localsliding, and so from a mechanical point of viewthe single layers could be consideredindependently.EXTRACELLUALRMATRIX9
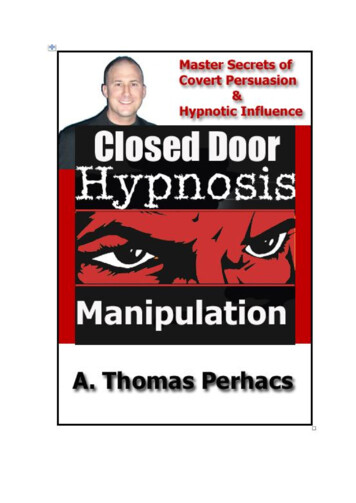
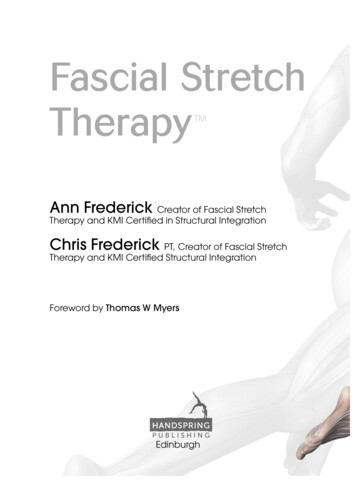
9/14/2015FASCIA IS WELL INNERVATED2007 C Stecco et al. Anatomy of the deepfascia of the upper limb. Second Part: studyif innervation. MorphologiePer cm2BrachialFasciaLacertusFibrosisAntebrachial FlexorFasciaretinaculumFree nerve 60.260.66Ruffini0.29Corpuscles0.10.260.55Others agree Tesarz J et al 2011 NeuroscienceSensory Innervation of thoracolumbar fascia in ratsand humansCorey, S.M. et al. 2011 Cell Tissue Organs SensoryInnervation of the nonspecialized connective tissuein low back of the ratWhat we find in fasciaMyelinated AxonNonmyelinated n.axonMUSCLESPINDLESScwann cellsFREE NERVEENDINGSMyofibroblastElastic fibersRUFFINICORPUSCLESCollagen ARAHYPAXIALMUSCLECOMPARTMNTL3PSPSQLQL2THREE LAYERMODELES11ES2TWO LAYERMODELPosterior layer1Posterior layerMiddle layer2Anterior layerAnterior ournal of AnatomyVolume 221, Issue 6, pages 507-536, 27 MAY 2012 DOI: ull#f310
9/14/2015EPIMYSIUMIN SERIES, ATTHE END OFEACH MUSCLETO FORM THEPARATENON,ANDCONTINUESINTO THEPERIOSTEUMP.P. Purslow / Comparative Biochemistry and Physiology Part A133 (2002) 947–966Aponeurotic Fascia Covers the ExtremitiesProximal boneinsertionsAponeuroticfasciaDistalinsertion intodeep fasciaEnvelopes muscles and connects them by wayof myofascial expansions (insertions) aroundjoints. Inserts into the periosteum, paratenon,neurovascular sheath and fibrous capsules ofthe jointsSlides on muscle due to loose connectivetissue between the “Aponeurosis” andEPIMYSIUM.Transmits forces generated by whole muscle.Connects to underlying muscle only atDistalmyofascial expansions. These occur generallyinsertioninto bone at joints and can merge with epimysium andparamysium.Stecco, C. Functional Atlas of the Human Fascial System. Elsevier 2015, ahead ofprintCourtesy of Warren Hammer, DC11
9/14/2015THE ANATOMICAL AND FUNCTIONAL RELATION BETWEEN GLUTEUS MAXIMUSAND FASCIA LATA THE DISTAL INSERTIONS OF THEGLUTEAL MUSCLES ARE MOREFASCIAL THEN OSSEOUS SUGGEST THAT VASTUS LATERALISAND BICEPS FEMORIS WORKTOGETHER TO STABILIZE THE LIMB THE FASCIA LATA FORMS THEINTERMUSCULAR SEPTUMBETWEEN HAMSTRINGS AND VASTI SEPTUM IS NOT JUST A SEPARATING ELEMENT ASSISTS WITH MOVEMENT COORDINATIONSurg Radiol Anat (2009) 31:35–42 DOI10.1007/s00276-008-0395-5Pectoral and femoral fasciae: common aspects andregional specializationsE1- Glute MaxE2 Glute MedE3- TFLSurg Radiol Anat (2009) 31:35–42 DOI10.1007/s00276-008-0395-512
9/14/2015Special Section: Series of Fascia Congress Abstracts - Part 3 (pp. 73-92)Volume 13, Issue 1, January 2009, Pages 53-62MYOFASCIAL SEQUENCEANATOMY OF THE DEEP FASCIA OF THE UPPER LIMB, SECONDPART:STUDY OF INNERVATION(C STECCO ET AL., MORPHOLOGIE 2007)DUE TO THE INNERVATION(AND STRUCTURE)OBSERVED, LUIGI AND CARLASTECCO, HYPOTHESIZED APROPRIOCEPTIVE ROLE OFTHE DEEP FASCIA“IT’S STRUCTURE IS IDEALFOR THE PERCEPTION OFDIRECTION TENSION”13
9/14/2015MECHANICAL BEHAVIOR MUST CONSIDER THE SUPERFICIAL AND DEEPRETINACULA CUTIS WITH SKIN MOVEMENT, THE SUPERFICIAL ADIPOSETISSUE MOVES MORE THAN THE DEEP ADIPOSELAYER IF THE RETINACULA ARE SHORT, STRONG ANDVERTICAL ALLOWS FORCE TRANSMITTED TO THEDEEPER PLANES IF THE RETINACULA ARE THIN, LONG AND OBLIQUE,THEY HAVE GREATER CAPACITY TO MUTE FORCETRANSMISSION TO DEEPER PLANES IMPORTANT TO PROTECTING VESSELS AND NERVESTHAT CROSS THE DEEP FASCIA MOST NOTABLY, ASSURES THE RECEPTORS IN THEDEEP FASCIA WILL NOT BE ACTIVATED DURINGNORMAL STRETCHING OF THE SKINMECHANICAL BEHAVIOR IN ADDITION TO MUTING SKIN STRESSES TO SUBQ TISSUES,HELP PREVENT HARMFUL EFFECTS FROM MUSCULARCONTRACTIONS TO THE SKIN NORMALLY WHEN MUSCLE CONTRACT THEY SLIDE EASILYUNDER THE SUBQ TISSUES AND THE SKIN IS NOT INVOLVED OCCURS BECAUSE, MUSCLE MOVEMENT ALWAYS STRETCHESSPECIFIC PORTIONS OF THE DEEP FASCIA, AND THEIR ACTIONINTO THE SKIN IS MITIGATED BY THE DAT AND THESUPERFICIAL FASCIAMECHANICAL BEHAVIOR RETINACULA CUTIS MUST BE FUNCTIONING NORMALLY FOR SLIDE GLIDEAND SEPARATION BETWEEN DF AND SF ALLOWS FOR SEPARATION OF ROLES SUPERFICIAL FASCIA- THERMOREGULATORY, LYMPHATIC FLOW,VENOUS/ARTERIAL PROTECTION, NERVE PATHWAYS TO PERIPHERY DEEP FASCIA- PROPRIOCEPTION, PERIPHERAL MOTOR CONTROL DEEP ADIPOSE TISSUE (DAT) FEWER NERVES, SERVES AS A WATERSHEDBETWEEN THE EXTEROCEPTIVE AND THE PROPRIOCEPTIVE SYSTEMS WHERE THE DAT DISSAPEARS, AND THE DEEP FASCIA AND SUPERFICIALFASCIA FUSE, THE EXTEROCEPTIVE AND PROPRIOCEPTIVE SYSTEMSUNITE REASON FOR HAND AND FOOT DEXTERITY-FACILITATES PERCEPTION OFFORM, VOLUME, AND STRUCTURE GUARANTEEING ADEQUATE MOVEMENT14
9/14/2015MECHANICAL BEHAVIOR WHAT HAPPENS WHEN THERE IS NOT NORMALSLIDE/GLIDE BETWEEN THESE LAYERS? WHAT HAPPENS WHEN A SCAR FORMS AND JOINSTHE SUPERFICIAL FASCIA WITH THE DEEPFASCIA? IN THESE SITUATIONS WHERE DENSE AND/ORFIBROUS TISSUE IS “FUSING” TOGETHER SKIN, SFAND DF STRETCHING THE DEEP FASCIA COULD AFFECTTHE SUPERFICIAL FASCIA AND VICE VERSA. IN THESE CASES, EVEN NORMAL MUSCLECONTRACTION OR SKIN STRETCHING COULDRESULT IN OVERSTIMULATION OFEXTEROCEPTORS AND/OR PRIOPRIOCEPTORSSO . Fascia is an intricate structure Muscles insert onto and originate from fascia Could play an active role in motor controlFASCIAL MANIPULATION ADOPTINGREASONING AND ASSESSMENT BASEDON:DIRECTION OF MOVEMENTCLASSICAL ANATOMYHAS SOME CONTRADICTIONS WITH REGARDS TO MOVEMENTDIRECTION AND TERMS I.E. HIP FLEXION OCCURS IN THE SAME DIRECTION AS KNEEEXTENSION PRONATION/SUPINATION ARE SIMILAR TOINVERSION/EVERSIONTraditionally we think that our motor cortex refersto muscles with origins and insertions that movebones but we will see how thinking in terms ofmovement direction serves us better15
9/14/2015PROPRIOCEPTIONBUILDING BLOCKSMUSCLE SPINDLEGOLGI TENDON ORGANJOINT REPLACEMENT SURGERY-CAPSULE REMOVEDJOINT RECEPTORS -PRIMARILY AT ENDRANGE, “LIMITDETECTORS” UNABLE TO SIGNALDIRECTION OF MOVEMENTOR POSITION IN “NORMALRANGE” SLOW RESPONDINGSKIN RECEPTORS 4 TYPES OFRECEPTORS SKIN STRETCH ALONECOMMONLYPRODUCED ILLUSORYMOVEMENTS CNS CONCEIVES MOVEMENTS ASFINALIZED GETSURES OR PATTERNS OFMOVEMENTS, STORED AS MULTIPLEREPRESENTATIONS IN THE CEREBRALCORTEX, AND NOT IN SINGLE MUSCLEACTIVITY THE NERVOUS SYSTEM INTERPRETS ANDPROGRAMS MOVEMENTS IN TERMS OFSPATIAL DIRECTIONS AND ANGLESMOTOREQUIVALENCEFINAL GESTURES16
9/14/2015Defining new boundaries on the human body14 segments.Each segment is controlled by 6 myofascial units (MFU)In 6 directions‐ 3 spatial planesTHE MYOFASCIAL (MF) UNIT1. Motor units, innervating fibres inmonoarticular and biarticular muscles, tomove a body segment in a specific direction2. the joint that is moved3. nerve and vascular components4. the fascia that connects these elementstogetherMOTOR UNITS INNERVATE MUSCLE FIBRESA Motor Unit one alpha-motorneurone and the musclefibres it innervates.May innervate 10 to 1000 muscle fibres.When activated all of its fibres contract.617
9/14/2015PARTITIONING HYPOTHESISTHE MYOFASCIAL (MF) UNITEach mf unit has a: Centre of Coordination (CC)where vectors from muscle fibrecontraction converge. Centre of Perception (CP)where movement occurring at thejoint is perceived9Anterior knee jointCENTER OF PERCEPTION (CP)Each MFU has a CENTER OF PERCEPTION (CP),where movement occurring at the joint is perceived. A vectoral center Resultant traction onto the joint capsule, tendons andligamentsA CP can become painful if, the unidirectional forces of the MFU are notsynchronized Mechanoreceptors in the capsule, ligaments andtendons are subjected aberrant forces18
9/14/2015CENTERS OF COORDINATIONHYPOTHESISCOULD BE POSSIBLE BECAUSE:1. Part of the deep fascia is fixed to bone2. Part of the deep fascia is free to glide1. The fascia is tensioned by myotendinousinsertions onto the fascia, and musclefibers inserting directly onto fasciaFUNCTION OF THE MYOFASCIAL UNITTHE CC OF A SEGMENT CORRESPONDS TOTHE CENTER OF VECTORS FORMED BY THECORRECT: TRACTIONS FROM MUSCLE FIBERS OFTHAT MOTOR UNIT TENSION THROUGH THE ENDOMYSIUMAND PERIMYSIUM TENSION OF THE LOCAL SEGMENT OFDEEP FASCIA (APONEUROTIC FASCIA OREPIMYSIAL FASCIA)“A PHYSIOLOGICAL SLIDING SYSTEM IN THE CC ISNECESSARY TO CREATE A CORRECT FINALVECTOR”19
9/14/2015CENTER OF FUSION (CF) CC-REGULATES UNIDIRECTIONALMOTOR UNITS OF A SINGLE MFU CF-COORDINATES INTERMEDIATEMOTOR UNITS, ACTIVATED DURINGMOVEMENT BETWEEN MFUs INDIFFERENT SPATIAL PLANES FASCIA ACTS AS ARHEOSTAT/REGULATOR activity of oneMFU andincreasingactivity ofanother.ANLADIAGONALS A DIAGONAL IS ASERIES OFCENTERS OFFUSION THATCOORDINATE TWOADJACENTSEQUENCESDURING AMOVEMENT IN ANINTERMEDIATEDIRECTION20
9/14/2015CF LOCATIONSCENTERS OF FUSION ARELOCATED IN: THE RETINACULA NEAR JOINTS, THE TENDONS, AND THE TRUNK, ALONG LINES OFUNIONS OF SOME MUSCLESDIFFERENCESBETWEEN CCs and CFsCENTERS OF COORDINATION OVER MUSCLE BELLIES ALONG LINES OF SPATIAL PLANES RECRUITED BY FORCEFUL UNIDIRECTIONALMOVEMENTSCENTERS OF FUSION OVER RETINACULA AND PERIARTICULAR STRUCTURES INTERMEDIATE POSITIONS RECRUITED BY GESTURES OR COMPLEX MOVEMENTSHyaluronic Acid HA is a large simple carbohydrate polymer of the ECM differs from other GAG in ECM as has no protein HA acts as a hydrating, space filling polymer Located within and between the interface of tissues (i.e deep fascia layers, muscle spindlecapsule) A LUBRICANT for fascia to glide Under conditions of stress, HA becomes depolymerized- PROMOTESIMFLAMMATION (inflammatory phase of wound repair is abundant in HA) HA acts as a promoter of early inflammation, which is crucial in the whole skinwound-healing process, W. Y. John Chen and Giovanni Abatangelo, Wound Repairand Regeneration, 1999, 7: 79–8921
9/14/2015DENSIFICATION- fibrotic tissuewhenever the denseconnective tissuecomponent is altered alteration of the looseconnective tissue (adiposecell, GAG, and HA). Caninvolve one or all three. correlates with amacroscopicrearrangement of thecomposition andconformation of theentire fascia tissue. alteration of the quantity orquality of the component ofthe loose connective tissuemay change the viscosityand therefore the function ofthe lubricant that the looseconnective tissue facilitatesD Y S F U N C T I O NFIBROSIS- VISCOSITY CHANGE DECREASED GLIDE CHANGE IN VECTOR JOINT INCCORDINATION COMPENSATIONSEQUENCES OFMYOFASCIALUNITS “3 dimensional movement andstabilization of each segment isguaranteed by synergy and synchronybetween the proximal and the distal,and the agonist and the antagonist MFunits” “Unidirectional MF units linked bymyofascial insertions form themyofascial sequences”22
9/14/2015TECHNIQUE Elbow, knuckles or fingers adhere to the skin Pressure must be sufficient enough to cross looseconnective tissue DEEP FASCIA AND IT’S DERIVATIVES ARE THETARGET TISSUE Treatment is applied away from the site of pain Visualize muscle anatomy and bony landmarks tolocate deep fascia to be treated.TREATMENT TIMEHYALURONIC ACID 0-15minOnset of inflammatory reactionThe smallestproducts of theHA cataboliccascade canturn about andsuppress theaction of oflargerpredecessors,and therebymodifying theireffects 15min-12hIncrease in inflammatoryreaction: Heat, edema. pain 12h-24Peak of inflammatory reactionStern R 2006 24hResolving of inflammatory reaction23
9/14/2015THANK YOUFor More Information www.fascialmanipulation.com www.myopainseminars.com myofascialphysiocare@gmail.com24
Fascial Manipulation Carl Heldman PT, DPT, MA, MTC, ATC, FAAOMPT. 9/14/2015 2 (Perimysium and endomysium) Fascia is a connective tissue: All connective tissue is derived from embryological mesoderm layer LEVEL 1: DEEP FASCI